
Remember me




A 45-year-old man was first admitted to our hospital because of worsening right-flank pain that had developed without trauma or other triggers.His mother had previously been diagnosed with the same disease.
The patient was diagnosed with ADPKD at the age of 40 when he visited a local clinic complaining of abdominal pain.At that time, the patient had a creatinine level of 1.0 mg/dL (eGFR 67.3 mL/min/1.73 m2), and hypertension (150/90 mmHg) was noted, which was managed with calcium channel blockers alone. The abdominal pain improved with observation alone. Subsequently, the patient occasionally experienced episodes of abdominal pain, but all symptoms improved with observation alone.
One week prior to admission to our hospital, the patient presented with right abdominal pain and visited a nearby clinic. This episode was the most intense attack of abdominal pain he had ever experienced. He was diagnosed with subcapsular hemorrhage of the right upper kidney. At that time, his creatinine level was 1.3 mg/dL and hemoglobin level was 15.9 g/dL. Simultaneously, he developed hypertension (190/110 mmHg) with hyperreninemia (renin activity 12 ng/mL/h), and was treated with a calcium channel blocker (amlodipine 10 mg) and an angiotensin II receptor blocker (olmesartan 20 mg). He was observed, but the pain intensified and the hemorrhage spread from the lower pole of the right kidney to the inguinal region, so it was decided that conservative management was not sufficient, and he was transferred to our hospital.
On admission, the patient was 179 cm tall and weighed 86 kg. His blood pressure was 132/79 mmHg and heart rate, 112 bpm. The results of laboratory tests were as follows: hemoglobin was 13,9 g/dL; albumin, 3.8 mg/dL; blood urea nitrogen, 21 mg/dL; creatinine, 1.3 mg/dL; estimated glomerular filtration rate, 48.8 mL/min/1.73 m2; prothrombin time, 89% (reference range, 70%-130%), activated partial thromboplastin time, 32.1 s (reference range, 24–36 s); and urinary protein excretion, 0.2 g/day. The urinary erythrocyte sediment contained less than 1 per high-power field. Cerebral aneurysm was ruled out by magnetic resonance angiography.
At the time of the renal hemorrhage, the Hb level was 15.5 g/dL.One week later, upon transfer to our hospital, the Hb level had decreased to 13.8 g/dL prior to TAE. As previously mentioned, renal hemorrhage beneath the renal capsule can compress the renal parenchyma from the outside, leading to a condition known as Page kidney, which is characterized by high-renin hypertension and requires urgent treatment such as surgical nephrectomy or TAE [1,2,3,4,5]. Based on this, we opted for TAE over nephrectomy.
After admission, bleeding into the right subcapsular space continued, so a right renal angiogram was immediately performed according to a previously reported method [6, 7]. Bleeding from the right capsular artery branch was confirmed, and renal TAE was immediately performed with four microcoils, after which hemostasis was confirmed (Fig. 1a). TAE stopped the progression of anemia and improved the pain, and subsequently, renal function decline no longer progressed. On admission day 20, the patient was discharged. Renin activity at discharge normalized to 0.3 (0.2–2.30 ng/mL/hr).
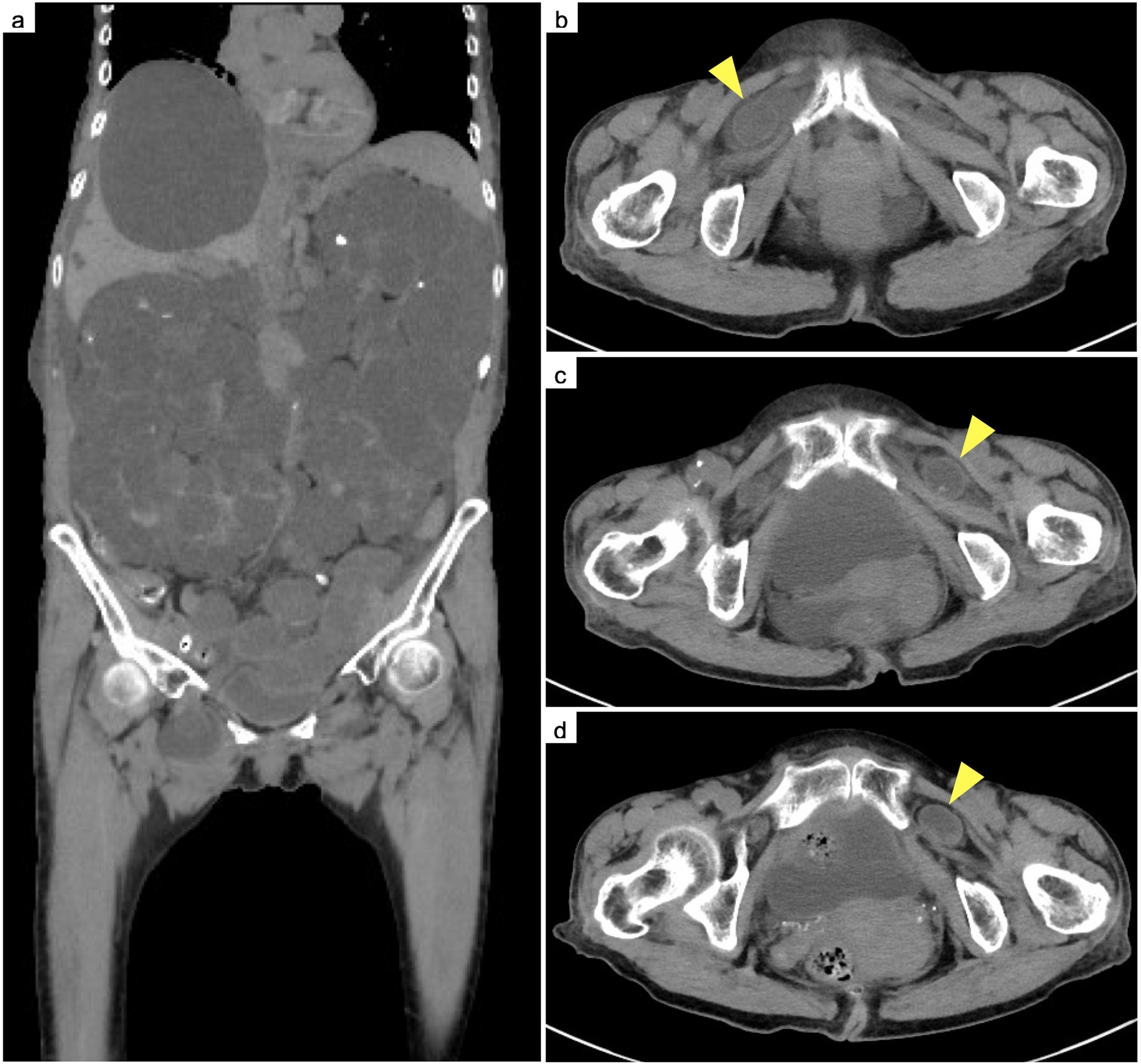
Fig. 1
a First bleeding episode A: Coronal computed tomography (CT) showed bleeding into the right subcapsular space (arrow). B: Right renal angiogram showed bleeding from the right capsular artery branch (arrow). C: Renal transarterial embolization (TAE) with four microcoils (arrow) was performed on the right capsular artery branch. b: Second bleeding episode A: CT showed bleeding into the subcapsular space of the upper pole of the left kidney. B: Left renal angiogram showed bleeding from the left superior capsular artery branch (arrow). C: Renal TAE with four microcoils (arrow) was performed on the left superior capsular artery branch (arrow).c: Third bleeding episode A: CT showed bleeding into the subcapsular space of the inferior pole of the left kidney (arrow). B: Left renal angiogram showed bleeding from the inferior pole branch of the left renal artery (arrow). C: Renal TAE with four microcoils (arrow) was performed on the inferior pole branch of the left renal artery. d: Fourth bleeding episode A: CT showed bleeding into the subcapsular space in the medial part of the upper pole of the left kidney (arrow). B: Left renal angiogram showed bleeding from the medial part branch of the upper pole of the left kidney. C: Renal TAE with four microcoils (arrow) was performed on the medial part branch of the upper pole of the left kidney
At age 50, the patient developed left-sided flank pain, and bleeding was identified in the subcapsular space of the upper pole of the left kidney. Since the condition worsened during follow-up observation in the first episode, TAE was immediately selected this time. Renal TAE was immediately performed with 4 microcoils on the left superior capsular artery branch, and hemostasis was achieved (Fig. 1b).
Four months later, bleeding was observed in the subcapsular space of the inferior pole of the left kidney. The bleeding was diagnosed as coming from the inferior pole branch of the left renal artery and was stopped with 5 microcoils (Fig. 1c).
At the age of 52 years, bleeding developed into the subcapsular space in the medial part of the upper pole of the left kidney. Renal TAE was performed with 2 microcoils, and hemostasis was achieved (Fig. 1d).
Five months after the fourth renal TAE, renal function progressively declined and hemodialysis was started. One year later, renal hemorrhage developed in both kidneys. Renal TAE was performed to occlude all bilateral renal arteries.
At the time of writing this manuscript, 4 years after the fifth renal TAE, no further bleeding has occurred. During the entire clinical course, no bleeding complications were seen outside the kidneys.
Genetic testing for Ehlers-Danlos syndrome was performed because of the patient’s tendency to bleed, but no genetic abnormality was identified.
Comments (0)