
Remember me



Cardiovascular diseases (CVD) remain the foremost cause of morbidity and mortality worldwide, representing a significant public health challenge. Risk stratification tools such as the SCORE2 and SCORE2-OP scales have been developed and tailored for use across diverse European populations, with adjustments reflecting country- specific epidemiological data on cardiovascular disease prevalence and outcomes. Despite their widespread clinical adoption and utility in risk stratification, these models possess inherent limitations. Notably, a proportion of individuals categorized as low risk at baseline may still experience adverse cardiovascular events during follow-up, highlighting the need for improved predictive accuracy and the integration of additional biomarkers.
In recognition of these limitations, the European Society of Cardiology (ESC) guidelines emphasize the critical role of subclinical organ damage assessment in refining cardiovascular risk categorization. Patients with established markers of subclinical organ damage- such as left ventricular hypertrophy, carotid atherosclerotic plaques, or increased arterial stiffness measured by pulse wave velocity (PWV) exceeding 10 m/s- should be reclassified into higher risk strata beyond that predicted by traditional SCORE2/SCORE2-OP scales. This approach aligns risk stratification more closely with the underlying pathophysiological burden and is pivotal for guiding intensified preventive strategies.
Sex-specific differences in cardiovascular risk profiles further complicate risk assessment. Available cardiovascular risk scales consistently indicate that women have lower estimated risk scores compared to men within equivalent age groups. This observation appears paradoxical in light of epidemiological evidence showing substantial cardiovascular mortality among women, which in some populations exceeds that of men [7]. Our study confirms this paradox by demonstrating significantly lower SCORE2/SCORE2-OP risk estimates in female participants relative to their male counterparts. Importantly, within the subgroup of women with coronary artery disease (CAD), most were aged 60 years or older, indicating a postmenopausal status exceeding a decade- an interval characterized by significant hormonal changes that affect cardiovascular physiology and risk. Conversely, women without CAD were generally younger (aged 50–59), corresponding to the early postmenopausal period. This temporal aspect of the menopausal transition is crucial for clinicians, as it highlights the need for targeted and timely intervention to mitigate emerging cardiovascular risk during this critical window.
Despite the recognized disease burden, women are disproportionately under-referred for diagnostic procedures evaluating myocardial ischemia, including functional stress testing and invasive coronary angiography. Consequently, revascularization interventions are less frequently undertaken in women compared to men, contributing to diagnostic and therapeutic gaps. This disparity is substantiated by a robust body of literature indicating underdiagnosis and undertreatment of stable angina in women, which adversely impacts clinical outcomes [8].
The importance of integrating subclinical organ damage markers into risk stratification is further illustrated by longitudinal cohort studies such as that by Sehestedt et al., which evaluated nearly 2000 Danish individuals [9]. Their analysis demonstrated that the inclusion of subclinical organ damage markers alongside traditional SCORE risk scale significantly enhances the prediction of cardiovascular mortality. Notably, they observed a dose-response relationship whereby increasing burden of subclinical organ damage correlated with escalating cardiovascular risk, affirming the prognostic value of these markers.
Consequently, both the European Society of Cardiology and the European Society of Hypertension advocate for the incorporation of subclinical organ damage parameters-including left ventricular hypertrophy, carotid artery plaques and elevated PWV into comprehensive risk assessment frameworks. Patients exhibiting these pathophysiological changes should be considered for escalation to higher risk categories, thereby prompting more aggressive preventive and therapeutic interventions aligned with their true cardiovascular risk profile.
5.2 The Role of the Ankle-Brachial Index (ABI), Intima-Media Thickness (IMT) and Pulse Wave Velocity (PWV) in Cardiovascular Risk AssessmentRecent literature has increasingly focused on the ankle-brachial index (ABI) as a critical marker in cardiovascular risk stratification. Patients diagnosed with lower extremity arterial disease (LEAD) require meticulous evaluation, as 40–60% of these patients have concomitant ischemic heart disease. Moreover, among patients presenting with intermittent claudication, 25–50% exhibit atherosclerotic changes in cerebral arteries, while up to 60% suffer from coronary artery disease, cerebrovascular disease, or both [10]. Conversely, approximately 40% of patients with coronary artery or cerebrovascular disease also manifest LEAD [11].
In our study, significant negative correlations between ABI and carotid intima-media thickness (IMT) were observed in women with hypertension, regardless of the presence of coronary artery disease (CAD). In contrast, such correlations were noted in men within the CAD without hypertension and in group without CAD and hypertension.
ABI measurement provides high diagnostic accuracy for hemodynamically significant peripheral arterial stenosis, with a sensitivity of approximately 90% and specificity nearing 100% [2]. Beyond diagnostic utility, ABI serves as an important indicator of overall cardiovascular risk, a finding corroborated in our cohort by the observed correlation between ABI and cardiovascular risk according to the SCORE2/SCORE2-OP scales. Notably, this correlation was significant only in women.
McKenna et al. evaluated the prognostic significance of LEAD severity in a cohort of 744 patients, demonstrating a striking disparity in five-year survival rates: 44% in patients with ABI < 0.4 versus 90% in those with ABI >0.85 [10]. Similarly, findings from the Systolic Hypertension in the Elderly Program (SHEP) and the Edinburgh Artery Study identified low ABI as a strong independent predictor of total and cardiovascular mortality, irrespective of metabolic syndrome or other conventional risk factors [12].
The advent of non-invasive vascular imaging modalities, such as Doppler duplex ultrasound, has enhanced the visualization of arterial morphology and atherosclerotic lesions [13]. These techniques are advantageous due to their non-invasiveness, reproducibility, and lack of adverse effects, thus rendering them indispensable in the assessment of subclinical organ damage. Consequently, carotid intima-media thickness (IMT) measurement was a pivotal component of our study.
Within the hypertensive subgroup without CAD, men exhibited significantly higher IMT and PWV values than women. IMT serves as an objective marker of cardiovascular risk, with our data revealing significant correlations between IMT and SCORE2/SCORE2-OP risk estimates in hypertensive women without CAD. In the group without CAD and hypertension, this correlation was observed in both sexes. IMT reflects vascular biological age, which frequently diverges from chronological age [14] and serves as a marker of systemic atherosclerosis affecting coronary, renal, and lower extremity arteries [15]. This phenomenon aligns with the concept of parallel atherosclerosis development across vascular beds. Given the accessibility of carotid and peripheral arteries, early atherosclerosis detection strategies appropriately prioritize these vascular territories over intracranial or coronary vessels.
Chambless et al. reported that an IMT exceeding 1 mm was associated with a 5-fold increase in cardiovascular risk in women and a 1.85-fold increase in men over a three-year follow-up [16], highlighting sex differences in the predictive value of IMT. Several clinical trials have confirmed that IMT adds incremental value to cardiovascular risk stratification, especially in individuals at intermediate risk [16]. A meta-analysis by Lorenz et al. involving patients without prior cardiovascular disease demonstrated that each 0.1 mm increase in IMT beyond 1 mm correlates with a 10–15% increased risk of myocardial infarction and a 13–18% increased risk of stroke [15]. The SMART study further linked IMT progression to incident cardiovascular events among patients with symptomatic CAD, peripheral arterial disease and carotid atherosclerosis [17]. Supporting evidence from cohort studies such as KIHD [18], ARIC [19], and CHS [20] reinforces the role of IMT as a robust predictor of myocardial infarction and stroke risk in asymptomatic individuals, with incremental risk evident even at modest increases in IMT. Secondary prevention research suggests that cardiovascular event risk escalates with IMT increments as small as 0.03 mm [19]. These findings collectively underscore the necessity of adjusting cardiovascular risk estimations by incorporating vascular age, as reflected by IMT, alongside chronological age [20].
Measurement of aortic pulse wave velocity (PWV) constitutes a non-invasive, validated method for quantifying arterial stiffness, particularly via carotid-femoral PWV assessment [21]. Arterial stiffness is recognized as an independent risk factor for cardiovascular morbidity and mortality among both healthy and hypertensive populations [22]. In our control group without CAD and hypertension, PWV demonstrated a significant correlation with SCORE2/SCORE2-OP risk exclusively in men, suggesting sex-specific applicability. Among hypertensive patients without CAD, men exhibited significantly higher PWV than women.
Extensive literature documents the prognostic relevance of aortic stiffness in predicting all-cause mortality, cardiovascular death, coronary events, and stroke across diverse patient populations including those with uncomplicated hypertension [23], type 2 diabetes mellitus [24], end-stage renal disease [25], elderly individuals [26] and the general population [27]. Landmark clinical trials such as CAFE and the REASON study highlight arterial stiffness as a key determinant in cardiovascular event prediction [28]. PWV measurement enhances risk stratification by identifying patients initially categorized as low or moderate risk who, in fact, possess elevated arterial stiffness and thus higher true cardiovascular risk. The Rotterdam Study established aortic PWV as an independent predictor of coronary heart disease and stroke in asymptomatic individuals [29], while the Framingham Heart Study linked increased aortic stiffness to the risk of a first cardiovascular event [30]. Reflecting its clinical utility, current ESC and ESH guidelines designate aortic PWV values exceeding 10 m/s as markers of subclinical organ damage warranting upclassification in cardiovascular risk assessment [31].
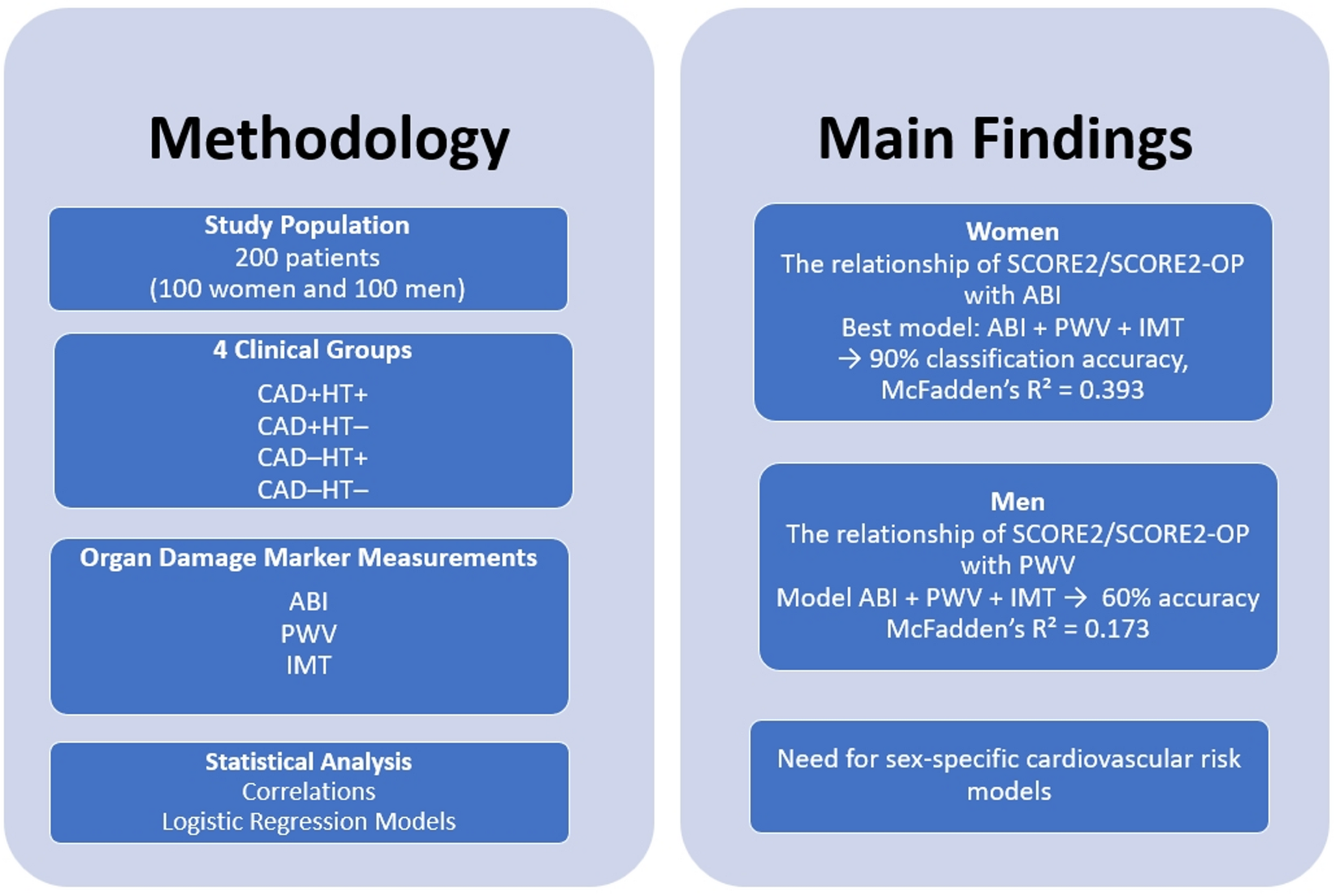
5.3 Logistic Regression ModelThe logistic regression model incorporating the simultaneous effects of Ankle-Brachial Index (ABI), Pulse Wave Velocity (PWV), and Intima-Media Thickness (IMT) demonstrates superior classification accuracy of cardiovascular risk according to the SCORE2/SCORE2-OP scale in women compared to men, with classification rates of 90% versus 60%, respectively. Furthermore, the model fit, as assessed by McFadden’s Pseudo R2, is markedly higher in women (0.393) than in men (0.173), indicating a substantially better explanatory power in the female cohort.
These findings suggest that logistic regression models integrating vascular biomarkers such as ABI, PWV and IMT may enhance cardiovascular risk stratification in patients undergoing primary prevention. Notably, the superior model performance in women highlights the potential for improved diagnostic precision in this population, which is frequently underdiagnosed or misclassified due to atypical clinical presentations and the traditional underestimation of cardiovascular risk in females.
Given that women often exhibit non-classical symptoms and are subject to diagnostic delays, the utilization of multifactorial models that incorporate subclinical vascular measurements could be instrumental in refining risk assessment protocols. This approach may ultimately contribute to more timely and targeted preventive strategies, reducing the burden of cardiovascular morbidity and mortality among women (Fig. 1).
Fig. 1
Methodology and Main Findings
5.4 Limitations of the StudyThis study has limitations that should be considered when interpreting the results. First, the sample size (n = 200 patients), especially after stratifying by sex and clinical subgroups, may reduce the statistical power and affect the stability of multivariable models. Second, the single-center design and the homogeneity of the Central European study population may limit the generalizability of the findings to other ethnic and geographic populations. Third, the cross-sectional design of the study does not allow for a definitive determination of causal relationships between vascular biomarkers: ABI, PWV, IMT and cardiovascular risk according to the SCORE2 and SCORE2-OP scales.
Moreover, although patients with diabetes, renal disease, and other significant comorbidities were excluded to minimize confounding, this may have introduced a selection bias and reduced the external applicability of the results to real-world populations.
Lastly, while logistic regression models were used to assess the joint effects of ABI, PWV and IMT, their overall discriminatory performance, particularly among men, suggests that additional biomarkers or risk modifiers may be required to optimize individual cardiovascular risk stratification.
Nevertheless, the study offers valuable insight into sex-specific differences in subclinical vascular markers and their relation to cardiovascular risk. These findings underscore the need for further multicenter, prospective research involving larger and more diverse populations. Importantly, the current results may serve as a solid foundation for future investigations aiming to refine cardiovascular risk prediction beyond conventional clinical parameters.
The results reflect associations rather than causal inferences, underscoring the need for prospective studies to confirm these findings. The observations highlight their associative, rather than causal, nature, and clearly indicate that prospective investigations are required to validate these outcomes.
Comments (0)