Severe Aortic Regurgitation with New Congestive Heart Failure Following Fetal Aortic Valvuloplasty – A Case Report
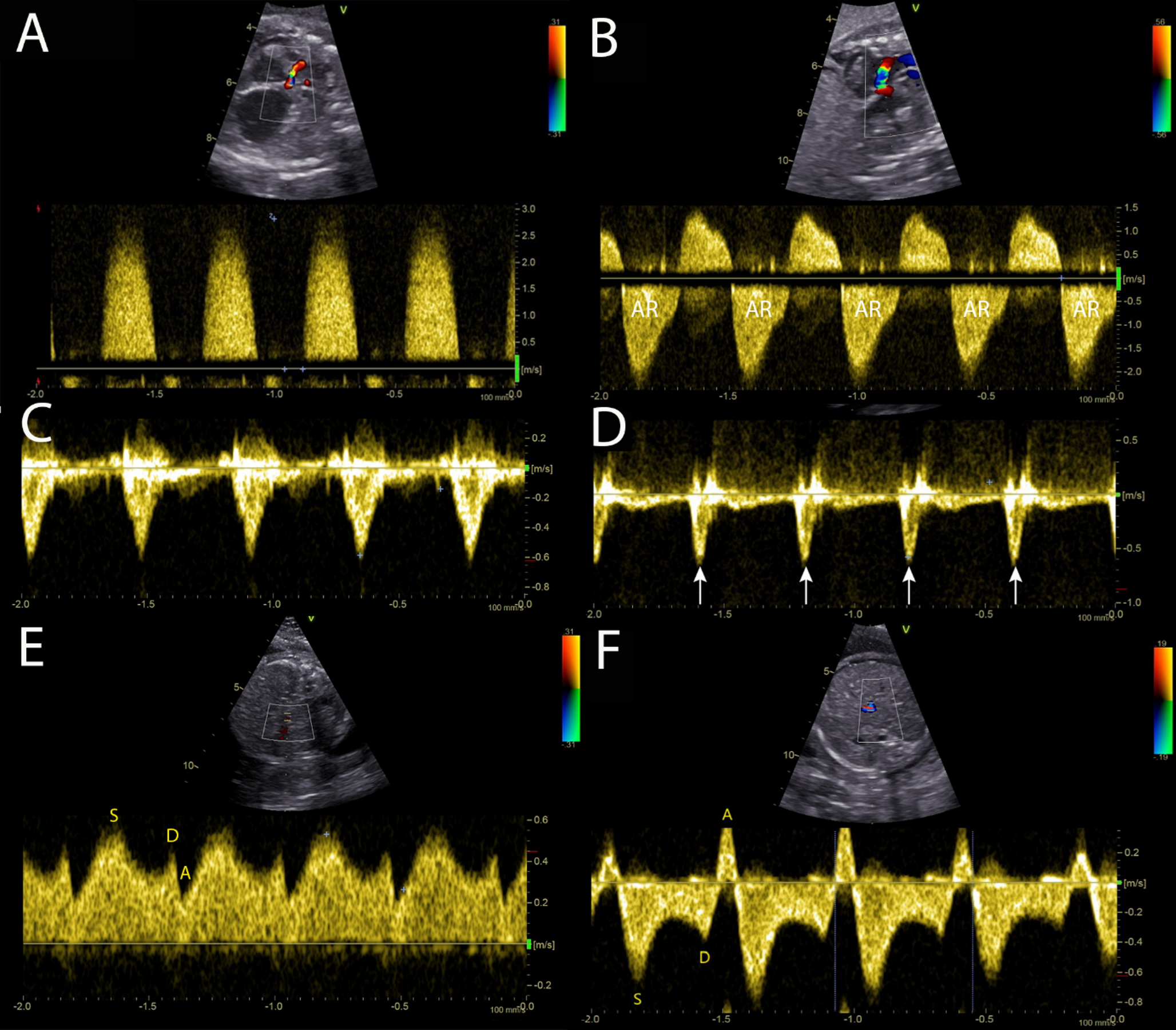
Fetal aortic valvuloplasty (FAV) is performed in fetuses with critical aortic stenosis (CAS) to prevent progression to hypoplastic left heart syndrome (HLHS). While successful FAV often results in new-onset aortic regurgitation (AR), this typically improves during gestation. We present a rare case of persistent severe AR following FAV, complicated by fetal congestive heart failure. A 28-year-old woman was referred at 23 + 0 weeks of gestation due to CAS of the fetus. Fetal echocardiography showed CAS with a peak velocity of 2.79 m/s, significant LV dysfunction and grade 2–3 endocardial fibroelastosis. No signs of heart failure were seen. The decision to perform FAV was made and the aortic valve was dilated to 115% of the valve diameter. After successful intervention, fetal echocardiography on the next day showed improved antegrade aortic valve flow with severe AR and signs of new RV dysfunction. Three days after intervention, development of ascites was observed. Due to further increase of ascites and poor cardiac function, the already established transplacental digitalization was increased. In the following weeks, hemodynamic stabilization could be observed with right ventricular function gradually improving and ascites resolving completely by 37 weeks of gestation. After elective C-section, the decision to perform early Ross-Konno surgery on the second day of life was made due to severe diastolic runoff. This case highlights the drastic hemodynamic changes associated with new significant AR after FAV and shows that successful in-utero treatment of congestive heart failure in this condition is possible.


Comments (0)