
Remember me
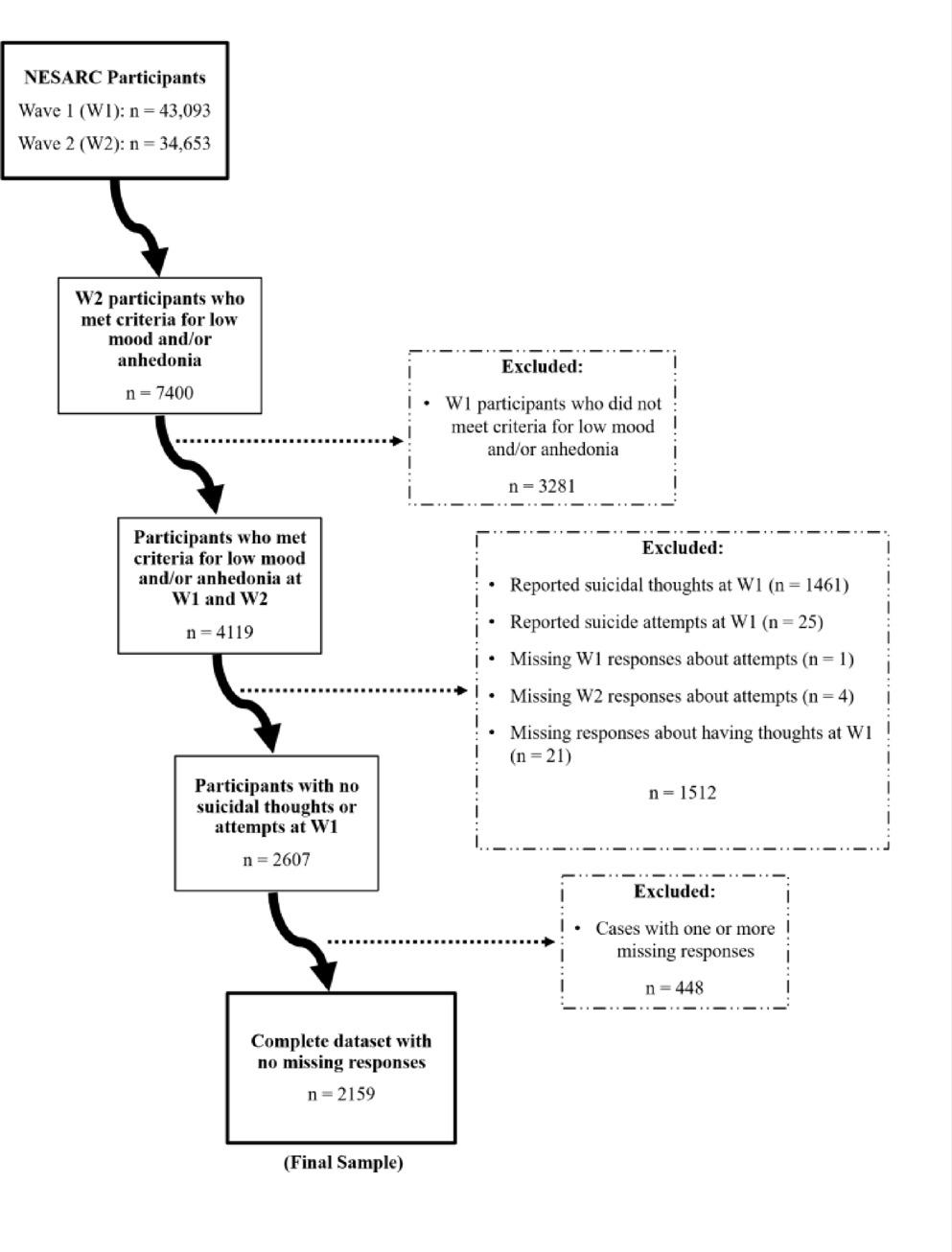
Participant demographics are summarised in Table 1. The final sample consisted of n = 3,702 participants, representing an overall response rate of 24.2%. Response rate was observed to fluctuate across year of data collection (2021: 16.1%, 2022: 36.3%, 2023: 22.9) and was higher among individuals who were offered an incentive to participate (40.5% vs. 16.7%). Respondents were aged between 16 and 36 years (Median:19, IQR:18–20), the majority of whom were women (60%; men: 37.4%, gender queer: 2.6%), cisgender (96.6%), heterosexual (73.7%), identified as being of Pākehā (European) descent (60.7%; Māori, 14.4%; Pacific peoples, 4.0%; Asian, 15.9%; Middle Eastern Latin American African [MELAA], 5.0%), and studying fulltime (94.4%; parttime, 2.2%; Non-degree/other, 3.4%).Approximately two-thirds were studying Arts and Science (63.6%; Medical Sciences, 12.1%; Commerce, 19.5%; Laws, 4.8%) and had at least one parent with at least a university degree (63.8%).
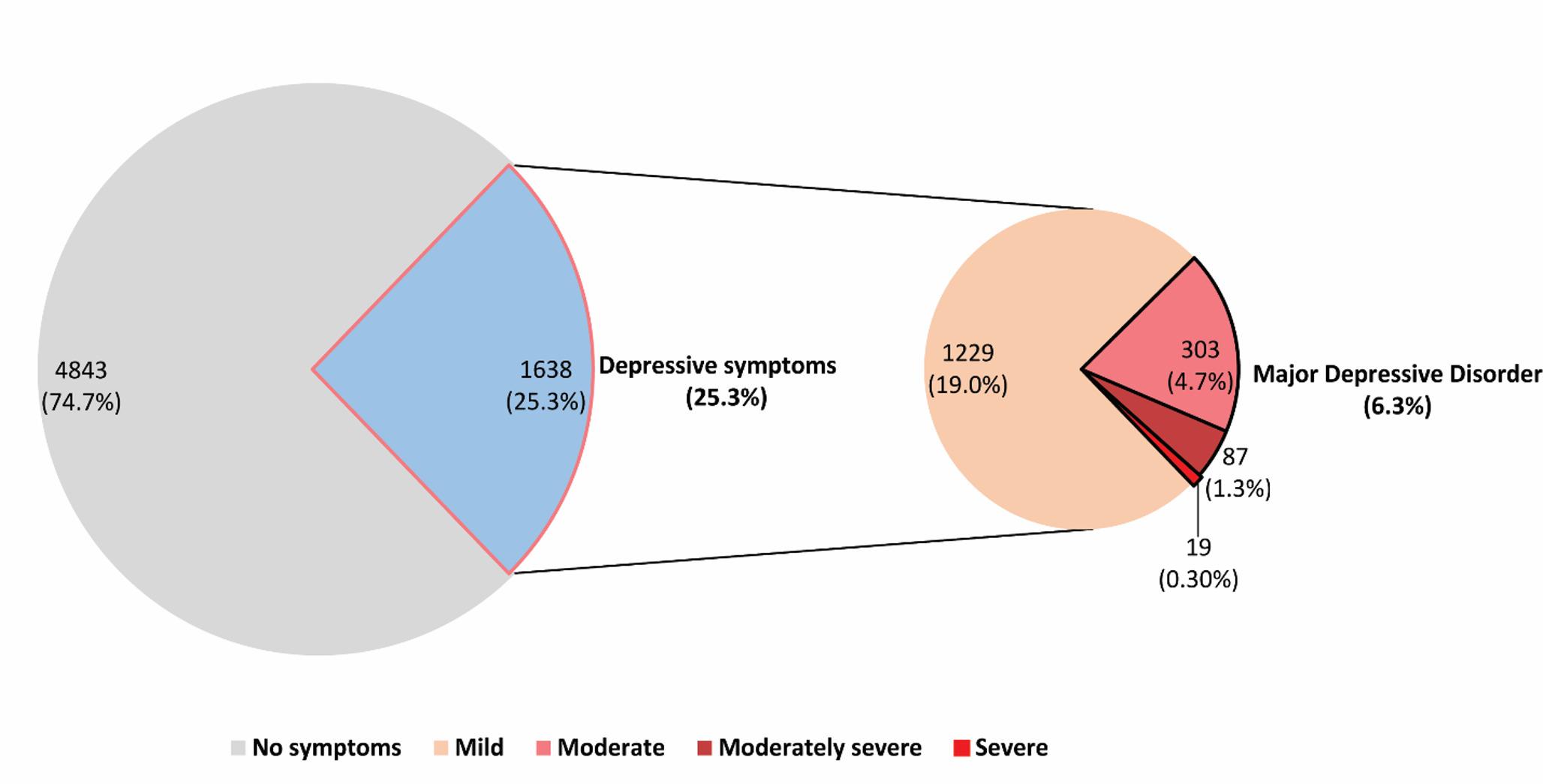
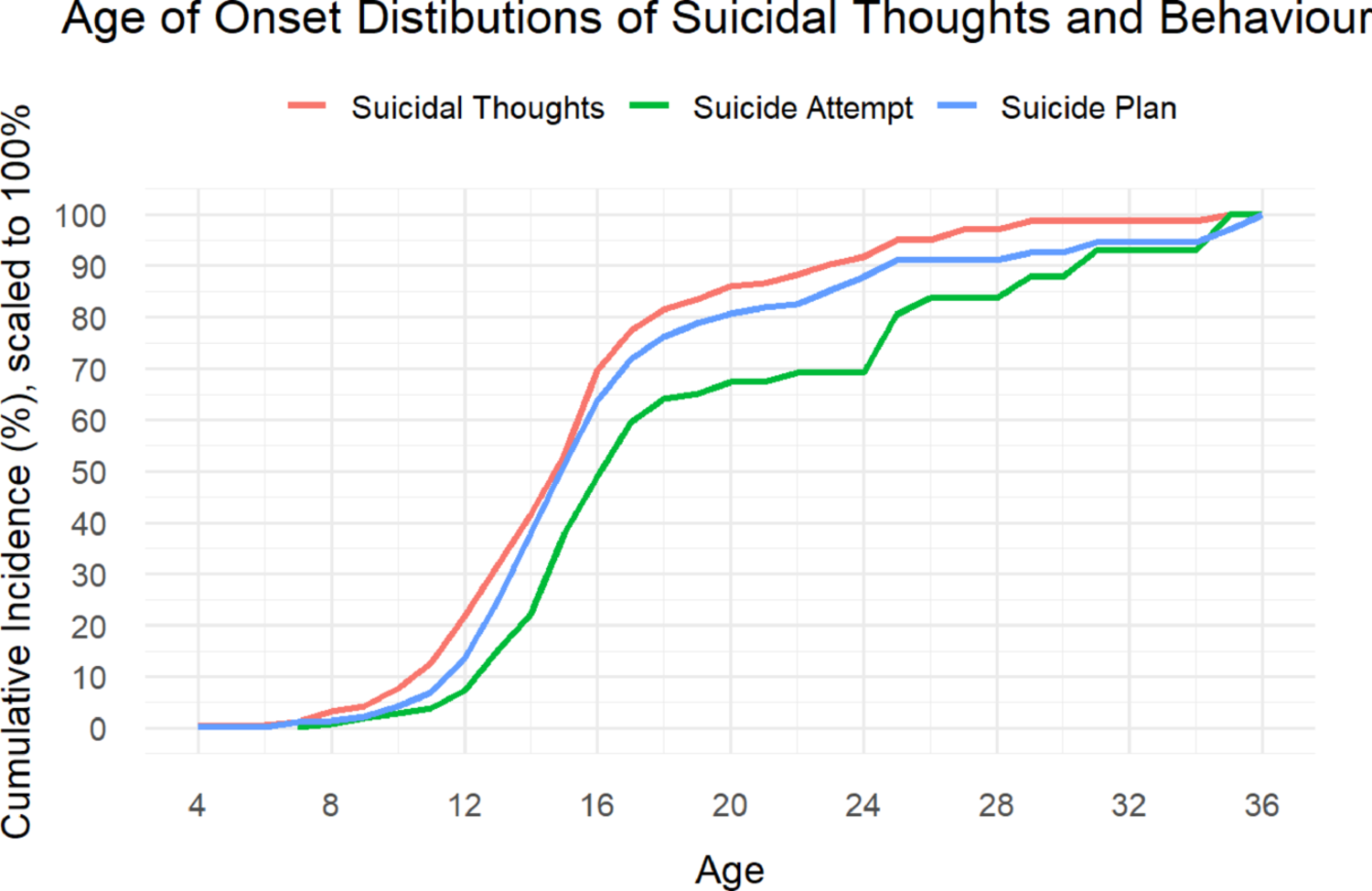
Table 1 Weighted demographic characteristics of the overall sample and those with or without any lifetime suicidal thoughts or behaviours, n = 3,702, % (SE)Prevalence, persistence, and age-of-onset of suicidal thoughts and behavioursEstimates are reported in Table 2. The lifetime prevalence for suicidal ideation was 54.1% (SE:1.0), suicide plans, 29.6% (SE:1.0), and suicide attempts 10.1% (SE:0.7), and the 12-month prevalence for these outcomes were ideation, 37.0% (SE:1.1), plans, 18.2% (SE:0.9), and attempts, 2.8% (SE:0.4). Of those reporting lifetime prevalence of suicidal thoughts or plans, the majority continued to experience thoughts (68.3%, SE:1.5) or plans (60.3%, SE:2.2) in the past 12 months. Approximately one-quarter of those who had made at least one lifetime suicide attempt had also attempted in the past 12 months (26.5%, SE:3.6). Median age-of-onset for each of these outcomes was 15 years (IQRs:12–16; Fig. 1).
Table 2 Lifetime and 12 month prevalence and persistence of suicidal thoughts and behaviours among 3,702 new Zealand university students, % (SE)Fig. 1
Age of Onset of Suicidal Thoughts and Behaviours
Among those reporting suicidal thoughts, about half of the respondents had made a suicide plan (Lifetime: 54.8%, SE: 1.6; Past 12 Months: 49.1%, SE: 2.0) and a minority had attempted suicide (Lifetime: 18.7%, SE: 1.2; Past 12 Months: 7.4%, SE: 1.1). Among respondents who reported having made a suicide plan, around one-third had also made at least one suicide attempt (Lifetime: 29.8%, SE: 1.9; Past 12 Months: 14.5%, SE: 2.0).
Associations of socio-demographics variables and mental disorders with lifetime suicidal thoughts and behaviours and progression along the suicidal trajectoryUnivariable models (Table 3) show that lifetime experiences of suicidal thoughts and behaviours and progression along the suicidal trajectory were most strongly and generally consistently associated with experiences of co-occurring lifetime mental disorders, and that the size of these associations increased as the number of co-occurring disorders the respondent had experienced also increased (F range 6.58–162.19, p < 0.05). These associations were strongest for suicide attempts, particularly for respondents with BP (RR: 5.84, 95% CI: 3.62–9.42) or PTSD (RR: 9.02, 95% CI: 5.82–13.94) who were five and nine times, respectively, more likely to have attempted suicide than their peers without these mental disorders. Among socio-demographic variables, being gender queer, transgender, or having a non-heterosexual orientation were associated with increased risk of suicide-related outcomes. Again, this was most striking for suicide attempts where these respondents were two-to-three times more likely to have attempted suicide than their female (RR: 2.48, 95% CI: 1.48–4.14), cis-gender (RR: 3.21, 95% CI: 1.98–5.20), or heterosexual peers (RR: 2.79, 95% CI: 2.05–3.79). Those who were transgender or non-heterosexual were also more likely to have progressed along the suicidal trajectory if they had thought about suicide, relative to their cisgender (e.g., attempt if ideation, RR: 1.92, 95% CI:1.26–2.92) or heterosexual peers (e.g., attempt if ideation, RR: 1.59, 95% CI:1.22–2.05), though interestingly, were not more likely to have attempted suicide if they have previously made a plan (transgender, RR: 1.46, 95% CI: 0.62–1.68; non-heterosexual, RR: 1.02, 95% CI: 0.79–1.31). Finally, no differences were found for ethnicity on any of the suicide-related outcomes or risk of progressing along the suicidal trajectory.
Table 3 The associations of demographics variables and lifetime experiences common mental disorders with lifetime suicide-related outcomes and transition along the suicidal trajectory, RR (95% CI)The fully adjusted multivariable models showed marked attenuation of independent associations as compared to the univariable associations. Notably, the associations for mental disorders were generally observed to approximately halve in magnitude and the majority of the associations with socio-demographic variables were no longer significant. Sequential multivariable modelling (shown in Supplementary Table A) reveals that these changes were largely explained by the mutual adjustment of mental disorder and to a lesser extent, the mutual adjustment of socio-demographic variables.
Within the fully adjusted models, non-heterosexual orientation was consistently associated with greater risk of lifetime suicide-related outcomes. Most strikingly, compared to their heterosexual peers, non-heterosexual students were approximately 62% more at risk of suicide plan (RR: 1.62, 95% CI: 1.41–1.87) and 45% more likely to attempt suicide (RR: 1.45, 95% CI:1.10–1.90). Additionally, non-heterosexual respondents who were already thinking about suicide were about 24% less likely to only experience suicidal thoughts (RR: 0.76, 95% CI: 0.64–0.91) and about 20% more likely to make a suicide plan than their heterosexual peers (RR: 1.22, 95% CI: 1.08–1.38). Modest increases in risk for suicidal ideation were also observed for students who were of Asian ethnicity (RR:1.17, 95% CI: 1.06–1.30) or studying commerce (RR:1.10, 95% CI: 1.02–1.19), and students studying medical sciences had lower risk of making a suicide plan (RR:0.77, 95% CI:0.61–0.98). No associations were found between age, gender, gender modality, enrolment status and parental education and lifetime suicide-related outcomes or progression along the suicidal trajectory.
Among respondents who had experienced a mental disorder, those with BP or PTSD were most at risk of having made a suicide attempt (BP, RR: 3.07, [95% CI:1.99–4.73]; PTSD, RR: 3.03, [95% CI: 1.77–5.20]) or progressing along the suicidal trajectory to attempt (e.g., attempt if plan, BP, RR: 1.89, [95% CI:1.23–2.88]; PTSD, RR: 1.98, [95% CI: 1.14–3.45]). MDD was also consistently, albeit more modestly, associated with increased risk of suicide-related outcomes (e.g., suicide attempt, RR: 1.80 [95% CI: 1.23–2.64]) and progression if the individual had experienced suicidal thoughts (e.g., attempt if ideation, RR: 1.49 [95% CI: 1.02–2.18]) yet lower risk of experiencing suicidal thoughts alone (RR: 0.78, 95% CI:0.65–0.94). Interestingly, the association between ADHD and suicidal ideation flipped between the univariable and fully adjusted multivariable models such that, in the adjusted model, ADHD conferred less risk of suicidal thoughts (RR: 1.59, [95% CI:1.48–1.70] vs. RR: 0.80, [95% CI: 0.67–0.97]). AUD was associated with reduced risk of suicidal ideation (RR: 0.75, 95% CI: 0.64–0.87) and plans (RR: 0.69, 95% CI: 0.53–0.92) within the multivariable models but was not associated with reduced risk within the univariable models (ideation, RR: 1.05 [95% CI:0.96–1.14], plan, RR: 1.12 [95% CI: 0.94–1.33]).
Associations of socio-demographics variables and mental disorders with 12-month suicidal thoughts and behaviours and progression along the suicidal trajectoryThe pattern of associations for past 12-month experiences of suicidal thoughts and behaviours and progression along the suicidal trajectory (shown in Table 4, with sequential models shown in Supplementary Table B) were largely consistent with those observed for lifetime experiences of these outcomes. For this reason, we have only commented on the substantive differences (Table 4).
Table 4 The associations of demographics variables and past 12-month experiences of common mental disorders with past 12 month suicide-related outcomes and transition along the suicidal trajectory, RR (95% CI)Of greatest interest was that, in the fully adjusted 12-month models, the risk of suicidal ideation and plans for non-heterosexual respondents increased by about 10% relative to the effect sizes observed in the lifetime models (ideation, RR: 1.50 [95% CI: 1.35–1.67], plans, RR: 1.72 [95% CI: 1.40–2.11]) yet, sexual orientation was no longer associated with risk of suicide attempt (past 12 months, RR: 1.74 [95% CI: 0.96–3.15] vs. lifetime, RR: 1.45 [95% CI: 1.10–1.90]). Similarly, the effect sizes also increased for the associations for MDD and BP, most notably for risk of suicide attempt where the risk doubled (MDD, RR: 3.65 [95% CI: 1.37–9.73] vs. RR: 1.80, [95% CI: 1.23–2.64]; BP, RR: 7.34 [95% CI: 2.20–24.45.20.45] vs. RR: 3.07 [95% CI: 1.99–4.73]). Notably, PTSD was not associated with risk of attempting suicide in the past 12 months, despite being one of the strongest predictors of lifetime suicide attempts (RR: 2.07 [95% CI: 0.94–4.57] vs. RR: 3.03 [95% CI: 1.77–5.20]).
Associations of socio-demographics variables and mental disorders with persistence of suicidal thoughts and behavioursAgain, we see a similar pattern for 12-month as for the lifetime models when testing associations between socio-demographics and persistence of suicidal ideation (see Table 5, and Supplementary Table C for sequential models). Non-heterosexual orientation and experiences of MDD and BP were associated with persistence of suicidal thoughts across univariable models and, to a lesser degree, multivariable models (e.g., non-heterosexual, univariable, RR: 1.22 [95% CI: 1.11–1.34] vs. multivariable, RR: 1.12 [95% CI: 1.02–1.23]). With the exception of AUD, all mental disorders were associated with greater risk of persistent suicidal ideation in univariable models; the effects for PD (RR: 1.30 [95% CI: 1.20–1.46] vs. RR: 1.05 [95% CI: 0.94–1.17]), PTSD (RR: 1.34 [95% CI: 1.21–1.49] vs. RR: 1.10 [95% CI: 0.98–1.23]), DUD (RR: 1.19 [95% CI: 1.05–1.33] vs. RR: 1.06 [95% CI: 0.93–1.21]), and ADHD (RR: 1.23 [95% CI: 1.11–1.37] vs. RR: 0.99 [95% CI: 0.78–1.26]) did not continue across multivariable models, however. In contrast to the lifetime models, older age was found to be associated with reduced persistence of suicidal thoughts (RR:0.84, 95% CI: 0.74–0.95) while experiences of GAD were found to increase risk of suicidal thoughts (RR:1.11, 95% CI:1.01–1.22). For persistence of suicide plans, only co-occurring BP was found to be associated with increased risk (RR:1.42, 95% CI: 1.06–1.92) and for suicide attempts, no statistically significant associations were observed.
Table 5 The associations of demographics variables and past 12-month experiences of common mental disorders with persistence of suicide-related outcomes in the past 12 month, given lifetime cases, RR (95% CI)
Comments (0)