Key factors
The aim of this scoping review was to clarify the concept of complex mental health care needs through the identification of key factors in recent literature. Housing insecurity, poverty, physical health issues and substance use were the factors mentioned most frequently in the included studies.
Some of these factors bear great resemblance to the social determinants of health (SDH), defined by the World Health Organization (WHO) as the ‘non-medical factors that influence health outcomes’37. What is considered a SDH is broad and constantly evolving [38]. In a 2018 systematic review on the social determinants of mental disorders, five also emerged as individual-level factors in this scoping review: housing insecurity, poverty, education & employment, cultural barriers and limited social support [39].
Several of these factors are interrelated: just as it is known that poverty is a significant SDH [38], it is also a risk factor for homelessness [40] and homelessness is in turn associated with high rates of physical health conditions, harmful substance use and severe mental illness [41]. This prompts the question whether these characteristics can truly be described as “individual” and links to the call for “an approach that attends to structural issues instead of treating poverty and inequality (solely) as symptoms of individual mental disorders”42.
Development of services that adequately meet complex, intersecting needs will require balancing tailored, person-centered interventions with strategies that address the societal inequalities driving these needs. Complex mental health care needs are not defined by a fixed set of factors but emerge from the cumulative impact of individual- and system-level issues. The intersecting nature of the identified factors is central to understanding wat makes mental health care needs complex [33, 43].
Despite this, evidence from this review suggests that the current care systems often fail to fully recognize these intersections, considering substance use or behavioral problems as “lifestyle choices”, assessing needs independently from one another [10] and failing to increase accessibility [10, 28, 30, 35] and quality [10, 27, 30,31,32] of care for those with complex care needs.
Although intersectional thinking increasingly finds its way into mental health care research, much of it remains conceptual [44]. Further research into practical implementation of an intersectional lens is essential to support the move away from hyperspecialized service providers working in siloed care organizations, toward truly integrated and adaptive care systems that are responsible to the unpredictable patterns of people with complex mental health care needs [27].
Strengths and limitations of the scoping review
To the best of our knowledge, this is the first scoping review to study complex mental health care needs. This review has several limitations and some strengths.
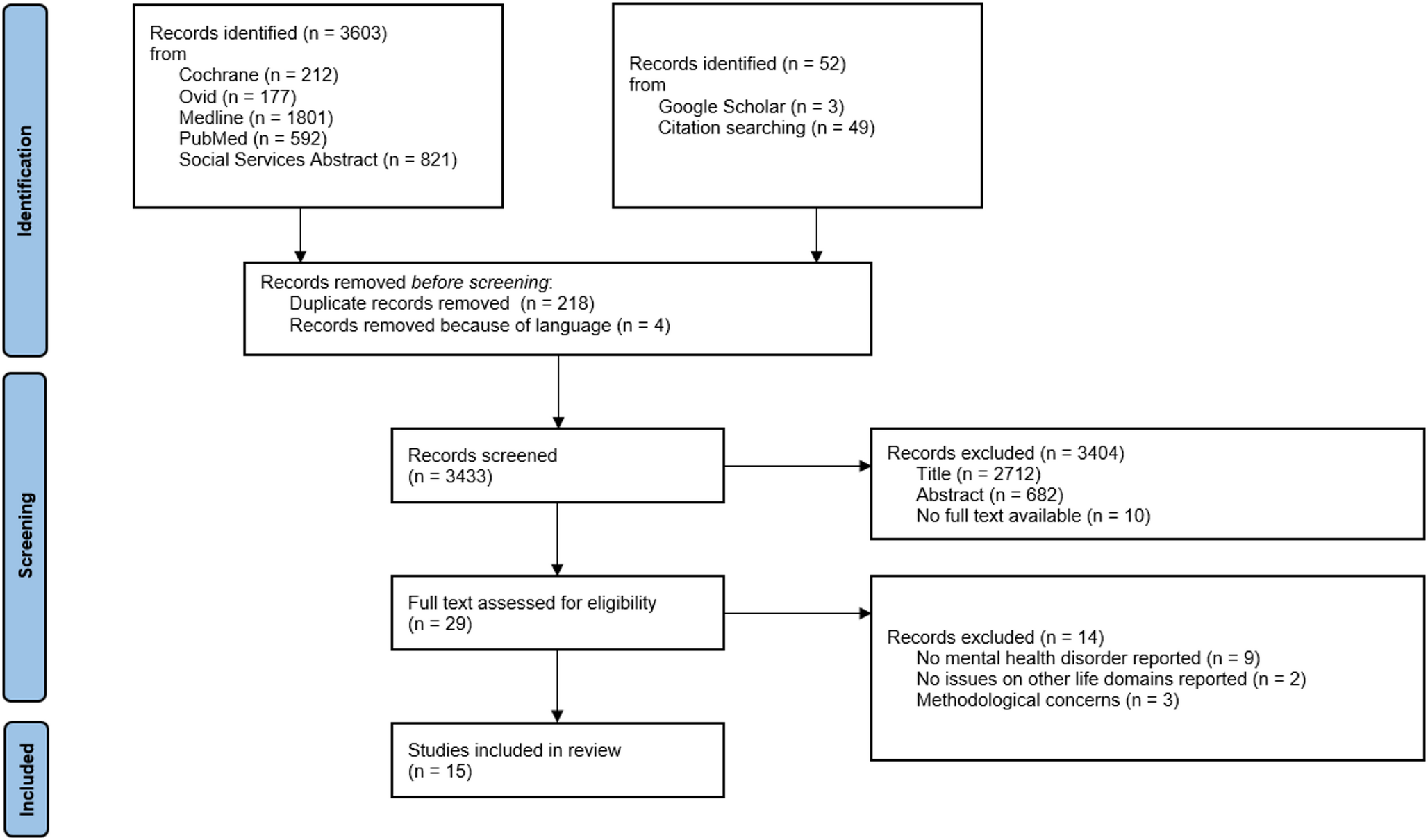
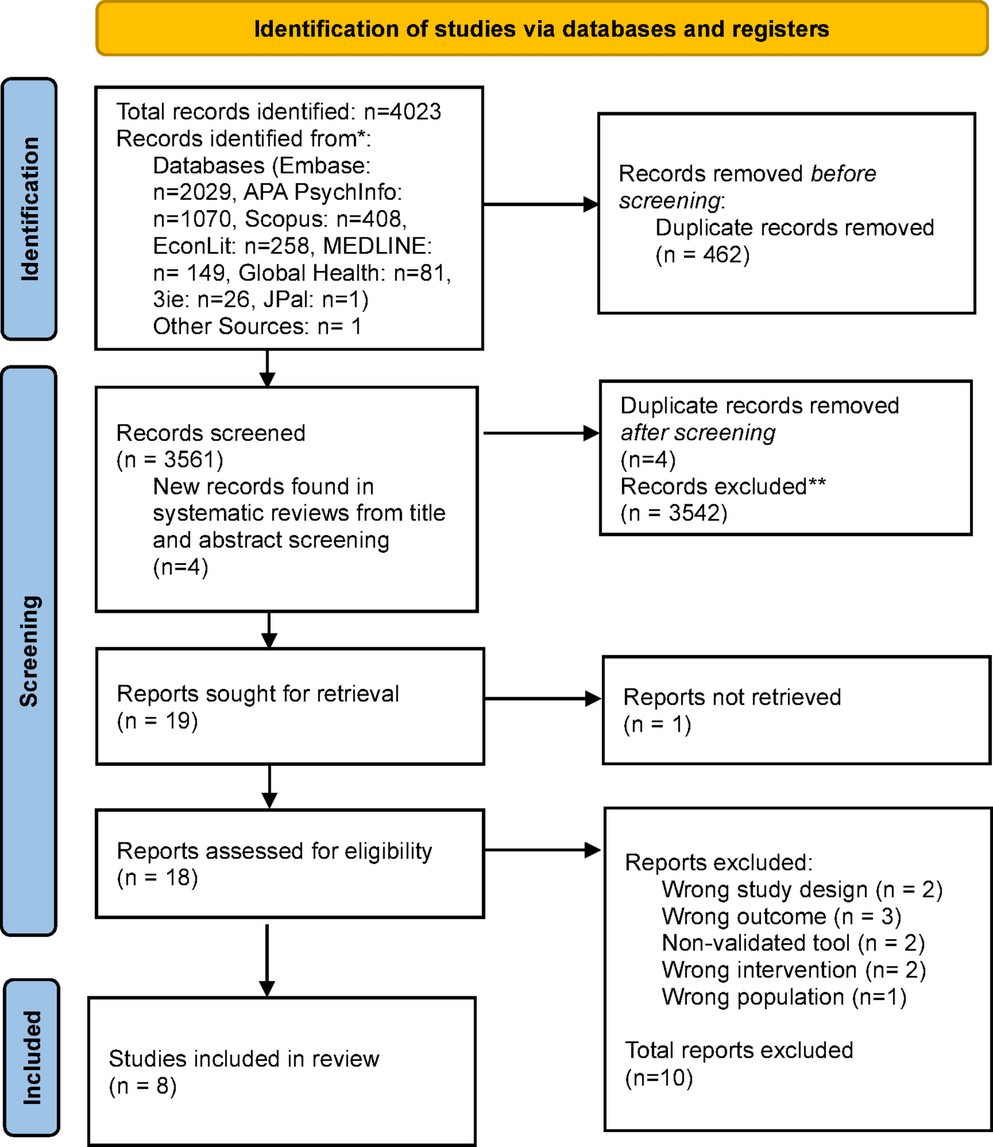
Although a comprehensive search strategy was applied, only a limited number of articles were included in this review. It is possible that some relevant articles were missed due, to the heterogenous use of terminology (see Table 2, ‘concepts’), or that additional databases should have been consulted.
The heterogeneity of terminology was noticeable in the understanding of mental health, that differed substantially across articles or was insufficiently specified. This was also the case for several of the identified factors, many of which the authors only mentioned or listed without further elaboration or definition (e.g. “[…] combined with physical illness, disabilities, cognitive impairment and/or substance misuse”34).
In line of thought with the inverse care law described in the introduction, some researchers have described an ‘inverse research law’: a disparity between the amount of research done and the contexts where needs are the highest [45]. The limited number of articles included in this review might also be a symptom of a general underrepresentation of people with complex mental health care needs in research. Future research into the concept could consider applying alternative research methods, for example a Delphi process. Research into the prevalence and distribution of complex mental health care needs is indicated as well.
A strength is that this review approached the concept of complex care needs from multiple contexts (i.e. mental health, primary, community and social care). Similar factors and challenges were found across contexts, supporting the assumption that people with complex care needs are to be found in different echelons of care and that challenges should be addressed in an intersectoral way. We deliberately focused on care as delivered in practice, thereby excluding the public health context and adjacent sectors such as education. This may to some extent limit the broader application of our findings, and could by some be considered a limitation. Another missing perspective in the article included is that of informal caregivers, on which none of the articles focused.
The factors identified in this scoping review are all problem-focused. This deficit-based research is typical for health research, but carries a risk of perpetuating stereotypes and stigma [46]. Identifying strengths and resilience of people with complex care needs will also be important in the development of interventions and the adaptation of services.
All studies are from high-income countries, limiting the generalizability of the findings to low- or middle-income settings. Moreover, nine studies originated from countries such as the United States, Canada, and Australia, where health insurance and social security systems differ substantially from those in other high-income countries. As social security plays a mediating role in the accessibility and cost of care, these differences might have influenced the findings. Still, socio-economic factors are mentioned across countries.
Ethical implications oflanguage and epistemic power
A complex patient or a patient with complex needs? Language holds power and helps shape the way care is organized and provided [47, 48] as well as the therapeutic relationship between clinician and patient [49]. For example, research has shown that physicians found a “substance abuser” to be more personally culpable and less in need of treatment than someone “having a substance abuse disorder”50. In that sense, it is interesting to note the evolution of the language used to describe this patient population over the course of the years: from a hateful patient in 1978[51] to a frustrating (1991)[52] or difficult (2001)[53] one. A 1988 article introduced the neologism heartsink, for patients who make their practitioners heart sink into their stomachs [54]. More recent articles included in this scoping review talk about complex or vulnerable patients or those experiencing disadvantages, separating the problems from the individual.
Clinicians as well as researchers hold testimonial power: great credibility is often given to their words, more than to service users [48, 55]. The evolution of mental health care away from the era of paternalism towards recovery-oriented care calls for critical evaluation of the normative language and the epistemic injustice still too prevalent in clinical practice and research.
When researching a concept like complex care needs, no conclusions can be drawn without reflecting on the disbalance in power still in place between care providers and service users [56]. Both in research and in practice thoughtful consideration should be given to the terminology used, given the impact this has on quality of care and experience of service users. For example, “high-need, high-cost” invokes other associations than “vulnerable” or “disadvantaged”.
An important limitation of this study is that no researchers with lived experience were involved in the development of this scoping review. LVS is a mental health nurse and junior researcher. The senior researchers involved are GD, JF and MD (psychiatrists), KvdB (clinical psychologist) and JM (sociologist with expertise on complexity and health).
Bearing this in mind, validation of the findings of this scoping review by people with lived experience should be sought and, further research on this topic should adopt research methods that do justice the reality of people with complex care needs, for example by in-depth, mixed-method case studies [57] or ethnographic narratives [31] to gain a deeper understanding of the barriers and facilitators influencing (intersectoral) care delivery to this population. Preferably, future research is developed in collaboration or co-creation with people with lived experience and their significant others [58, 59] with attention for strengths-based approaches [46].

Comments (0)