4.1 The Sequential Afatinib–Osimertinib Strategy: A Durable and Accessible Alternative
The principal finding of our study is that sequential afatinib-to-osimertinib therapy achieved a median OS of 55 months (95% CI 53.2–66.4), substantially exceeding outcomes with alternative second-line strategies (32.3 months [95% CI 30.2–35.6]; aHR 0.43 [95% CI 0.35–0.52], p < 0.001) and demonstrating remarkable durability that appeared competitive with, or potentially superior to, contemporary first-line combination strategies. This sequential strategy leverages the complementary mechanisms of second-generation irreversible pan-HER inhibitors followed by selective third-generation EGFR-TKI therapy targeting both sensitizing and T790M resistance mutations [15, 16]. The biological rationale underlying this strategy is supported by the high T790M positivity rate (96%) among patients who progressed on afatinib and subsequently received osimertinib therapy, consistent with afatinib’s potent and irreversible EGFR inhibition that preferentially selects for T790M-mediated resistance over alternative bypass mechanisms [20]. This finding is consistent with previous research showing that prolonged first-line EGFR-TKI therapy promotes the emergence of T790M-mediated resistance. Huang et al. reported that patients treated with first-generation EGFR-TKIs for more than 11 months were significantly more likely to develop T790M mutations, reflecting the sustained selective pressure that drives this resistance mechanism [21]. Our data corroborate these observations in the context of afatinib, where potent and irreversible EGFR inhibition appears to preferentially select for T790M rather than alternative bypass pathways.
The survival advantage observed with sequential second- to third-generation EGFR-TKI therapy in our study is further supported by the Korean RESET real-world cohort, in which patients receiving sequential TKIs achieved approximately twofold longer survival than those who did not receive such sequencing [22]. This consistency across independent Asian real-world cohorts—the GIANT study in Taiwan and the RESET study in Korea—strengthens the evidence base for sequential TKI strategies and underscores the biological and clinical validity of this treatment paradigm in routine practice.
From a pragmatic healthcare perspective, sequential afatinib–osimertinib therapy offers several practical advantages that merit consideration, particularly in resource-limited settings and healthcare systems with reimbursement constraints. Sequential monotherapy strategies avoid the cumulative toxicities associated with combination chemotherapy–TKI regimens, potentially improving treatment tolerability and patients’ quality of life [23]. The substantial cost difference between sequential monotherapies and upfront combination strategies represents a meaningful consideration for healthcare systems and patients facing financial toxicity. Furthermore, reserving osimertinib therapy for T790M-positive progression enables biomarker-guided precision therapy, ensuring that the most advanced TKI reaches patients who are most likely to benefit while maintaining therapeutic options for subsequent lines. Under the constraints of Taiwan’s National Health Insurance reimbursement policies during the study period, this sequential strategy maximized therapeutic benefit and promoted more efficient resource utilization in clinical practice.
4.2 Patient Population Differences and Real-World Representativeness
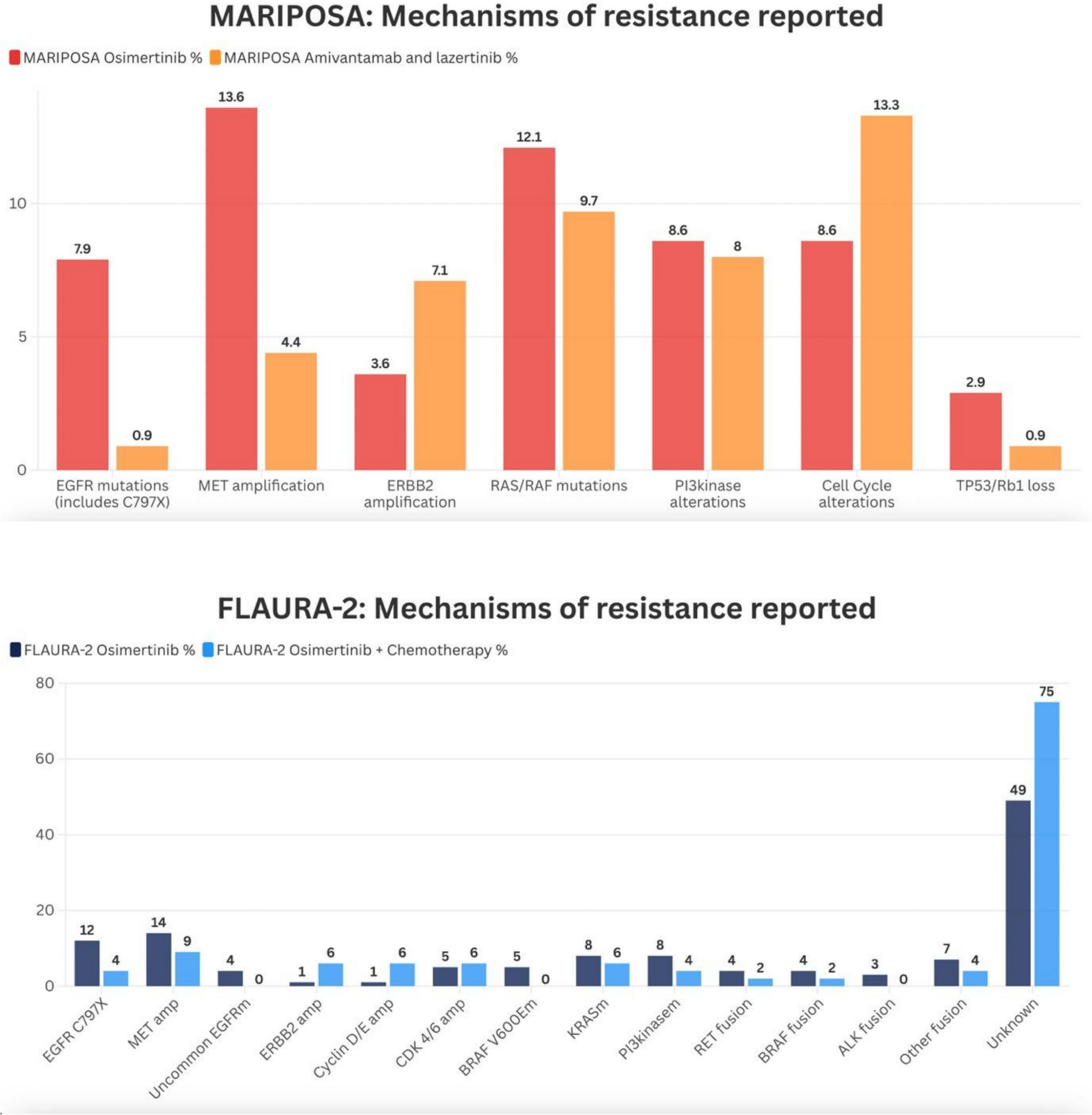
Critical evaluation of our study cohort reveals important differences in patient eligibility and baseline characteristics compared to landmark clinical trials. The FLAURA-2 and MARIPOSA trials enrolled highly selected patient populations with stringent inclusion criteria, including a mandatory ECOG performance status of 0–1, adequate organ function, and specific exclusion criteria that eliminated many patients encountered in routine practice. In contrast, 5.6% of the patients enrolled in the GIANT study had an ECOG performance status of ≥ 2, reflecting real-world practice patterns where treatment decisions must accommodate patients with compromised performance status. When we restricted our analysis to patients enrolled in the GIANT study who met the trial eligibility criteria for performance status (ECOG 0–1), survival outcomes remained robust and closely aligned with those in the trials, suggesting that the effectiveness of the sequential strategy translates across performance status strata.
The baseline prevalence of central nervous system (CNS) disease also differed across studies, with brain metastases present in 32–34% of patients enrolled in the GIANT study compared to 40–44% in the FLAURA-2 and MARIPOSA trials. This difference may reflect varying screening practices, with contemporary trials mandating baseline brain imaging while real-world practice employs symptom-driven assessment. Importantly, our subgroup analyses demonstrated consistent survival benefits with sequential afatinib–osimertinib therapy regardless of baseline brain metastasis status, with the median OS exceeding 51 months in patients with CNS involvement—a remarkable outcome given the historically poor prognosis of this population. These findings support the effectiveness of sequential TKI strategies in managing intracranial disease, likely attributable to osimertinib’s superior CNS penetration and activity against brain metastases [24].
Supportive care, imaging technologies, molecular diagnostics, and clinical management strategies underwent substantial evolution during the GIANT study period, spanning 2016 to 2024. In our study cohort, earlier patients received treatment in the era before the approval of first-line osimertinib therapy, when sequential strategies represented standard practice, while later patients were treated in an era with expanding awareness of combination approaches. This temporal heterogeneity introduces complexity in outcome interpretation but simultaneously provides valuable real-world evidence that spans the evolution of clinical practice.
4.3 Study Limitations and Considerations
The GIANT study has several important limitations that warrant acknowledgment. To begin with, its retrospective design introduces inherent selection bias, confounding by indication, and incomplete data capture that limit causal inference [25, 26]. In addition, treatment allocation was non-randomized and influenced by clinical factors, T790M testing availability, physician preferences, and reimbursement considerations. For instance, the prolonged PFS with first-line afatinib therapy of 20.4 months in the osimertinib-sequenced group substantially exceeded the 10.3 months observed in the chemotherapy group, suggesting that patients who ultimately received osimertinib therapy may have had more indolent disease biology or superior treatment adherence. Indeed, the significantly higher response rate to first-line afatinib therapy in this group (79% vs. 64%, p < 0.001) supports this interpretation.
Furthermore, T790M testing was not performed uniformly across the study cohort, with 34% of patients lacking post-progression molecular assessment. The T790M rate in this study (59%) is higher than that previously reported [27]. A possible explanation is that we did not systematically track biopsy adequacy or failure rates, which could have inflated our T790M positivity rate. That said, we did not exclude non-evaluable or failed samples from the denominator; instead, cases without confirmed T790M status were categorized as “unknown/not done.” Another limitation is that detailed procedural-level biopsy data were not consistently available for all centers, reflecting the retrospective and multicenter nature of this study. In addition, the GIANT dataset spans multiple years (2016–2024), during which changes in Taiwan’s National Health Insurance reimbursement policies and improvements in diagnostic testing accessibility could have influenced treatment continuation patterns and clinical outcomes. For example, patients treated in the earlier years of the study received care before the widespread availability of liquid biopsy technologies and before osimertinib was accessible as a first-line option, whereas patients treated later benefited from expanded molecular testing capabilities and evolving treatment paradigms.
Lastly, cross-trial comparisons represent indirect analyses subject to substantial confounding from differences in patient populations, treatment eras, supportive care practices, and outcome assessment methodologies [28]. Individual patient-level data from the FLAURA-2 and MARIPOSA trials were unavailable, precluding robust statistical adjustment for baseline differences. Finally, the predominantly Taiwanese patients in our cohort population may limit the generalizability of our findings to other ethnic populations with different EGFR mutation distributions and treatment responses.
4.4 Value of the GIANT Study as Real-World Evidence and Clinical Implications
Despite these limitations, the GIANT study provides valuable real-world evidence that complements RCT findings by reflecting clinical practice beyond controlled settings. Real-world data capture authentic treatment decisions, drug accessibility constraints, patient heterogeneity, and management approaches that characterize routine oncology care. In this context, the study’s limitations can be reframed as strengths—demonstrating how sequential TKI therapy performs in populations with comorbidities, variable performance status, financial constraints, and treatment discontinuations that would typically exclude them from clinical trials. The concordance between our real-world survival outcomes and those reported in highly selected RCT populations further suggests that the sequential afatinib–osimertinib strategy delivers robust clinical benefits across diverse patient groups and practice settings.
Our findings suggest that sequential afatinib-to-osimertinib therapy represents a durable, effective, and economically viable treatment strategy for patients with EGFR-mutated advanced NSCLC, achieving survival outcomes that appear competitive with contemporary combination strategies. For healthcare systems and patients where upfront combination strategies pose financial, toxicity, or access barriers, sequential TKI therapy offers a rational alternative supported by robust real-world evidence. However, prospective randomized trials directly comparing sequential monotherapy strategies to upfront combination strategies are needed to definitively establish optimal treatment paradigms. Future studies should incorporate comprehensive quality-of-life assessments, cost-effectiveness analyses, and patient-reported outcomes to guide personalized treatment selection beyond survival endpoints alone.

Comments (0)