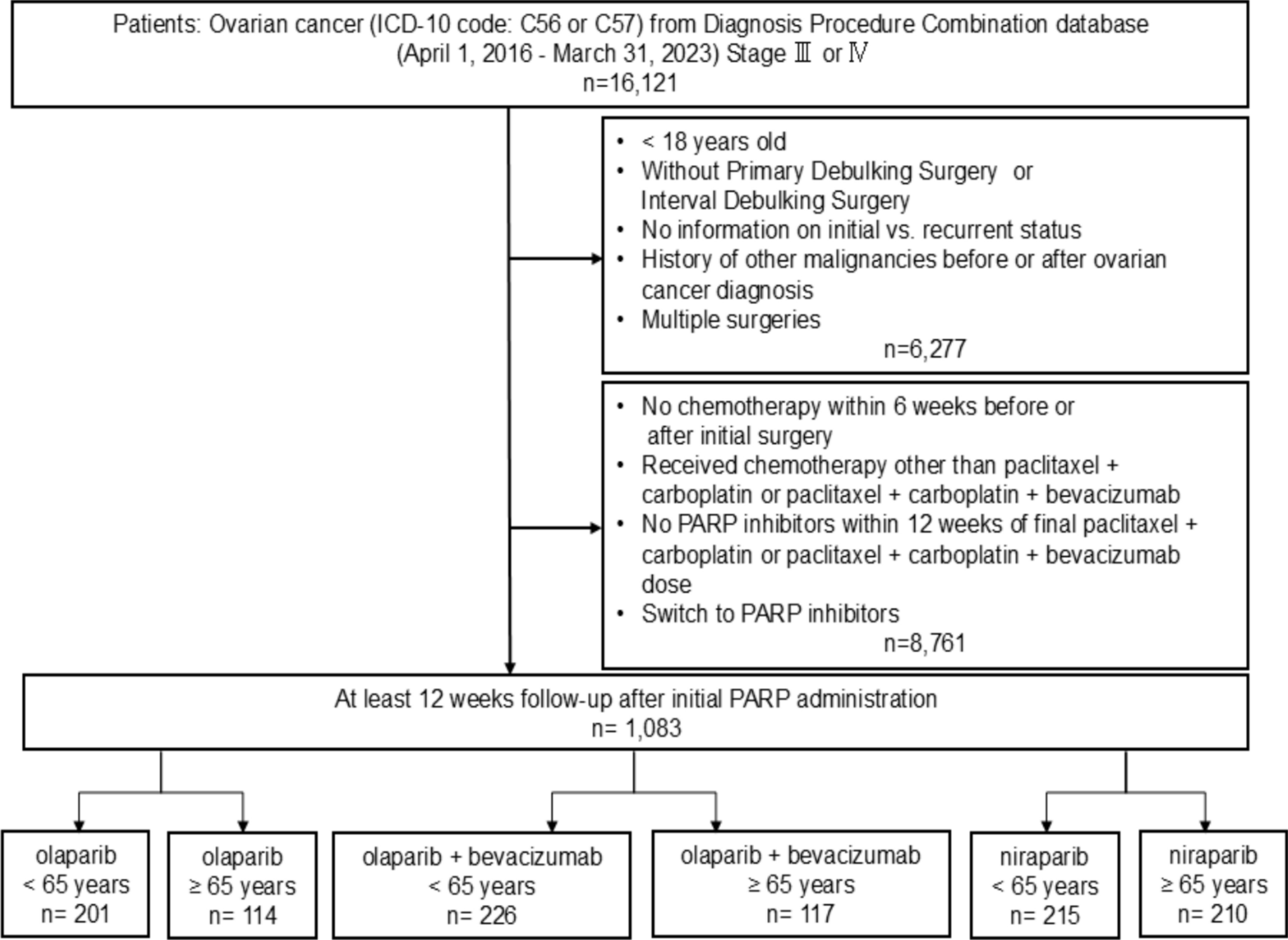
In this study, we evaluated the incidence of clinically significant SAEs by age in 1083 patients with advanced ovarian cancer receiving PARP inhibitor maintenance therapy between 2016 and 2023. The incidence of severe anemia and thrombocytopenia was comparable between the two age groups for all regimens. Although severe neutropenia appeared more frequently in patients aged ≥ 65 years receiving olaparib monotherapy (incidence rate ratio = 7.47, 95% CI 2.37–23.5), this magnitude was unexpectedly high compared with those in prior reports. This pattern was not observed in the other treatment groups (olaparib plus bevacizumab or niraparib), thus it is unlikely to be explained solely by the effect of age. Residual confounding from unmeasured factors—such as baseline hematologic parameters, renal function, HRD/BRCA status, Eastern Cooperative Oncology Group (ECOG) performance status or frailty, cumulative chemotherapy dose intensity, prior chemotherapy exposure, bone marrow reserve, or drug‑specific susceptibility—remains possible. Therefore, this finding should be interpreted as hypothesis generating rather than as definitive evidence of age‑related toxicity.
Our findings are broadly consistent with previous clinical trials evaluating PARP inhibitors in advanced ovarian cancer. Specifically, severe anemia and thrombocytopenia did not differ significantly by age across any treatment regimen, aligning with the PAOLA-1 trial (olaparib plus bevacizumab: anemia ≥ 70 vs. < 70 years, 21.2% vs. 16.5%; thrombocytopenia: 1.9% vs. 1.6%) and the PRIMA trial (niraparib: anemia ≥ 65 vs. < 65 years, 27.4% vs. 33.3%; thrombocytopenia: 26.1% vs. 18.0%) [14, 15]. The substantially increased risk of severe neutropenia in older patients receiving olaparib monotherapy was not observed in the olaparib plus bevacizumab or niraparib groups. In the PAOLA-1 trial, grade ≥ 3 neutropenia occurred in 5.1% and 9.6% patients aged < 70 and ≥ 70 years (olaparib plus bevacizumab), respectively, while in the PRIMA study, it occurred in 13.0% and 16.0% patients aged < 65 and ≥ 65 years (niraparib), respectively [14, 15]. Although the substantially increased risk of severe neutropenia in older patients receiving olaparib in this study is noteworthy, the cause of this age-related increase remains unclear. Variations in prior chemotherapy cannot fully explain this finding, as all patients received a similar paclitaxel–carboplatin regimen. Moreover, the number of chemotherapy cycles was included as a covariate in the inverse probability weighting-adjusted analysis, suggesting that differences in cycle number do not account for the observed effect. Detailed data on cumulative chemotherapy exposure, including dose intensity, were not available, and unmeasured factors—such as frailty, HRD/BRCA status, renal function, ECOG performance status, and bone marrow reserve—may have influenced toxicity. Therefore, we cannot completely exclude the possibility that these factors may have contributed to higher neutropenia risk in older patients. The lack of histologic subtype information is another limitation, particularly in Japan where clear cell carcinoma is more prevalent and may influence treatment sensitivity. These unmeasured factors may have acted in combination to produce the observed increase in neutropenia risk among older patients receiving olaparib monotherapy. Despite this uncertainty, careful monitoring is necessary in older adults receiving olaparib, given the short neutrophil lifespan (approximately 5 days) and potential for early-onset myelosuppression. Further studies accounting for potential residual confounding and detailed treatment-related information are warranted to clarify these findings.
In the present study, the rates of severe nausea and vomiting were similar across age groups, while interstitial lung disease was rare, observed only in patients younger than 65 years. Additionally, we observed no significant age-related differences in treatment interruption or discontinuation, consistent with prior reports [14, 15]. Myelosuppression generally occurred within the first few months, and older patients tended to experience earlier anemia and neutropenia onset, emphasizing close monitoring. The small number of events within subgroups likely limited the power of the time‑to‑event analyses, thereby warranting cautious interpretation of the non‑significant findings. Moreover, the hospitalization rate was similar between patients aged ≥ 65 years and those younger than 65 years in the olaparib and olaparib plus bevacizumab groups. In contrast, in the niraparib group, patients aged ≥ 65 years had fewer hospitalizations owing to myelosuppression and nausea/vomiting than the younger patients. Although this pattern may partly reflect more proactive dose management among older adults, it is also likely influenced by residual confounding or selection bias. Importantly, the median follow‑up duration and median niraparib exposure time were shorter for the older patients, suggesting that the lower hospitalization rate may reflect reduced treatment exposure rather than a true difference in toxicity risk. Older patients were more likely to initiate therapy at reduced starting doses and require additional dose reductions within 12 weeks, particularly with niraparib. These observations highlight the importance of individualized dose adjustment; however, the potential influence of unmeasured confounding must be acknowledged.
This study has several strengths, including the use of one of the largest medical databases in Japan, which covers a wide variety of institutions and reflects real-world clinical practice. Additionally, the study provided a detailed analysis of the actual use of PARP inhibitors and patterns of clinically significant SAEs in patients with advanced ovarian cancer, clarifying safety profiles by age group in a large cohort of 1083 patients treated between 2016 and 2023.
Nevertheless, this study has certain limitations. First, the database only included participating institutions, potentially limiting the generalizability of our findings. Second, treatments and adverse events that occurred at other institutions were not captured, potentially leading to incomplete data. Third, the clinically significant SAEs evaluated in this study were inferred from medical records and medication information, and therefore it did not necessarily correspond to laboratory‑confirmed CTCAE grade ≥ 3 events. These operational definitions should be interpreted as proxy measures, and the true incidence of severe toxicities may be underestimated. Although this approach is widely used in pharmaco‑epidemiologic studies using the Diagnosis Procedure Combination database, the absence of laboratory data prevented full CTCAE alignment [19, 24, 25]. Fourth, key determinants of toxicity—such as baseline blood counts, renal function, HRD/BRCA status, performance status or frailty, and cumulative chemotherapy dose intensity—were not available in this database. Consequently, estimates of age‑related differences in adverse events are subject to residual confounding, and the observed differences between the younger and older patients may reflect unmeasured patient characteristics rather than age itself. Additionally, information on histologic subtype was not available. Histologic subtype may influence chemotherapy sensitivity and susceptibility to PARP inhibitor–related toxicities; therefore, the absence of histologic information may have contributed to residual confounding in the observed age‑ and regimen‑related differences. Finally, although treatment interruptions or discontinuations were defined based on delays or cessation following adverse events, they may have occurred due to other reasons. Despite these limitations, this extensive real-world investigation provides hypothesis-generating evidence regarding age-related differences in the safety profiles of PARP inhibitor maintenance therapy, which can inform future prospective studies.
Although the evidence is hypothesis generating, our findings have several clinical implications. First, older patients receiving olaparib monotherapy may be at increased risk of severe neutropenia, particularly within the first few months of therapy, underscoring the importance of proactive monitoring and timely dose adjustments. Second, real-world hospitalization data suggest that age-appropriate and carefully monitored dose management may help reduce the risk of adverse events in older adults. Third, the earlier onset of bone marrow toxicities in patients aged ≥ 65 years emphasizes the necessity of vigilant monitoring, particularly during the initial months of therapy. Collectively, these results suggest that proactive management and individualized treatment strategies may enhance the safety of older patients, but further prospective validation is warranted. Future research should validate these strategies using prospective studies and explore predictive markers for hematologic toxicity to optimize PARP inhibitor therapy in older populations.

Comments (0)