
Remember me
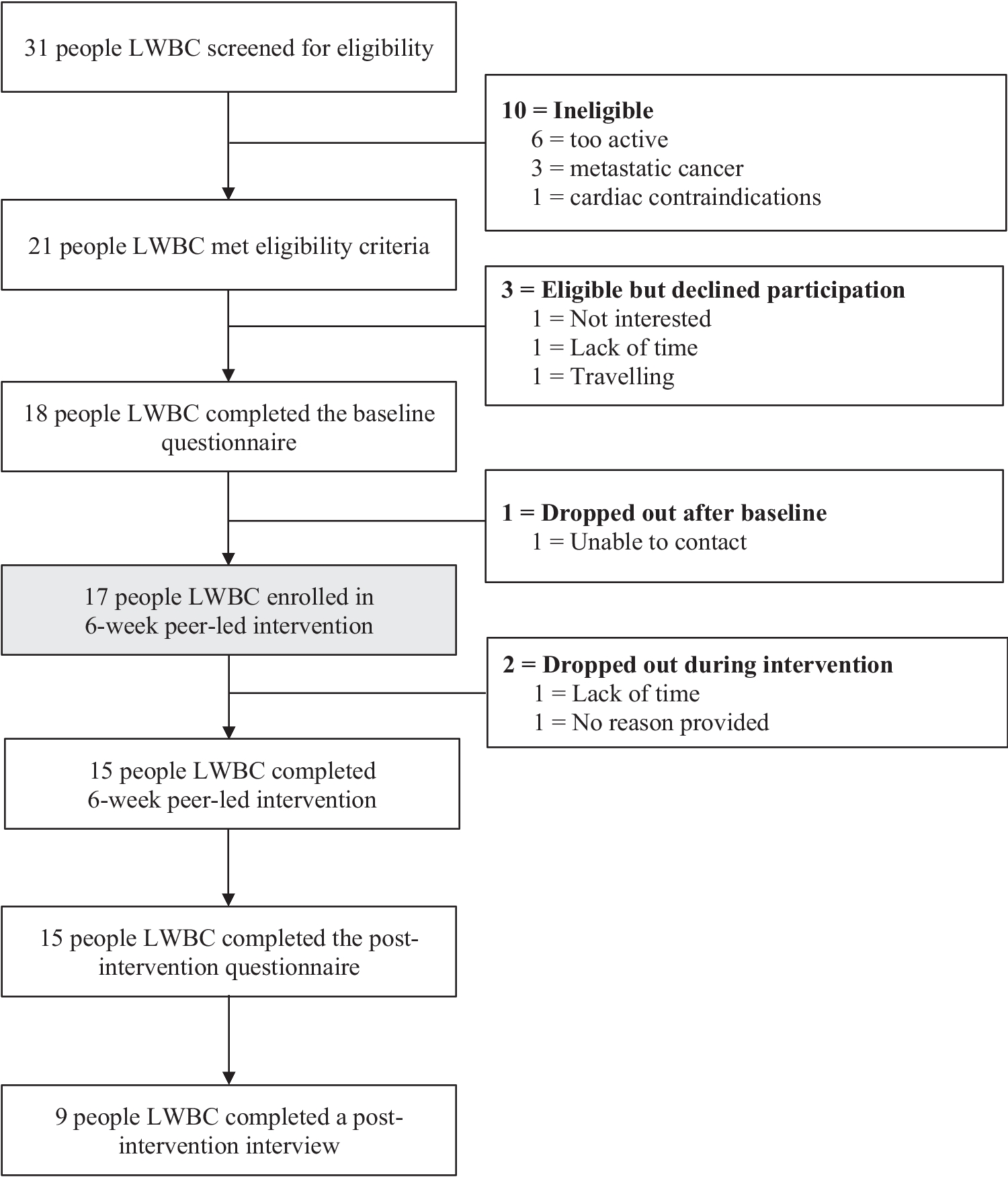
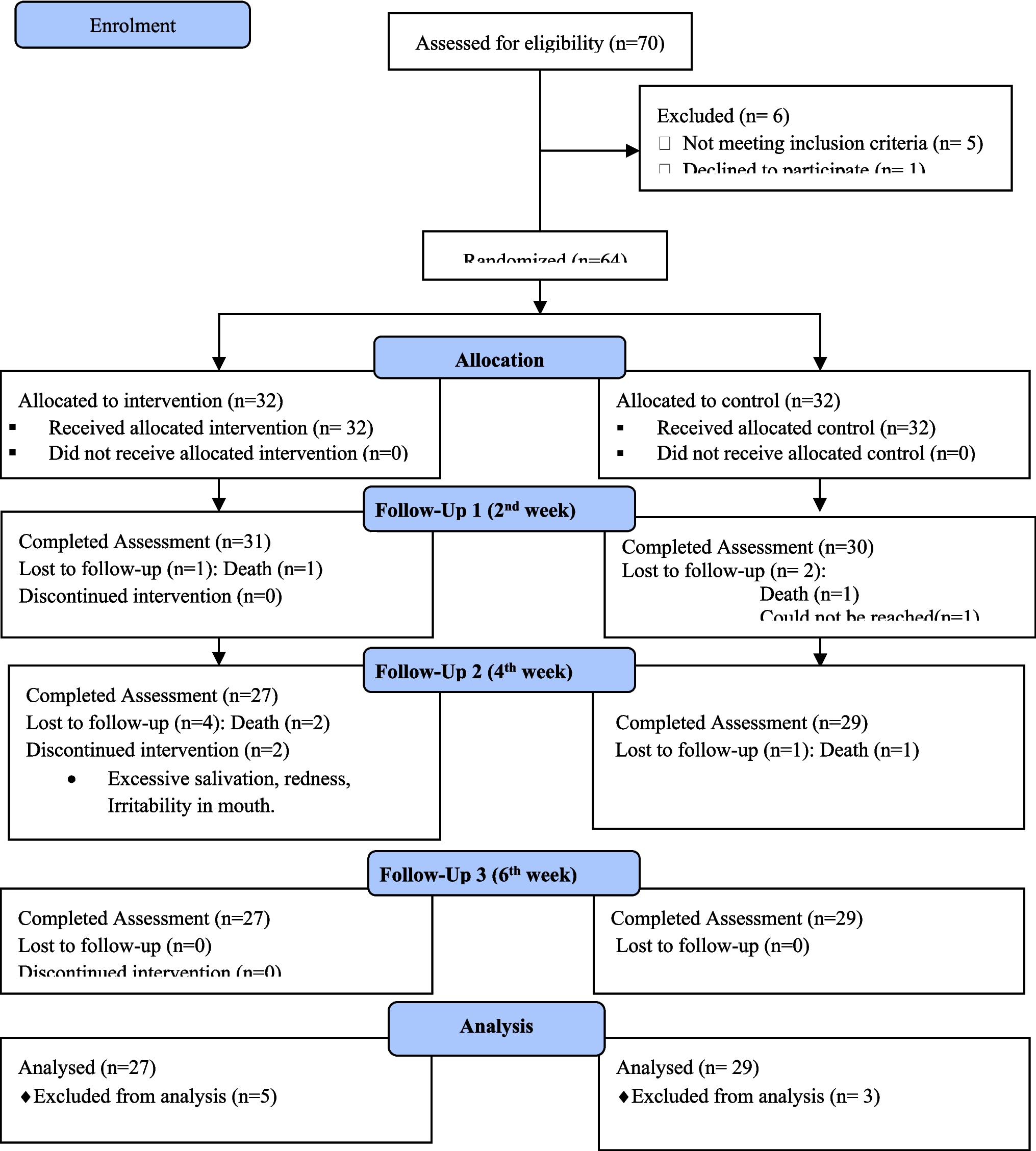

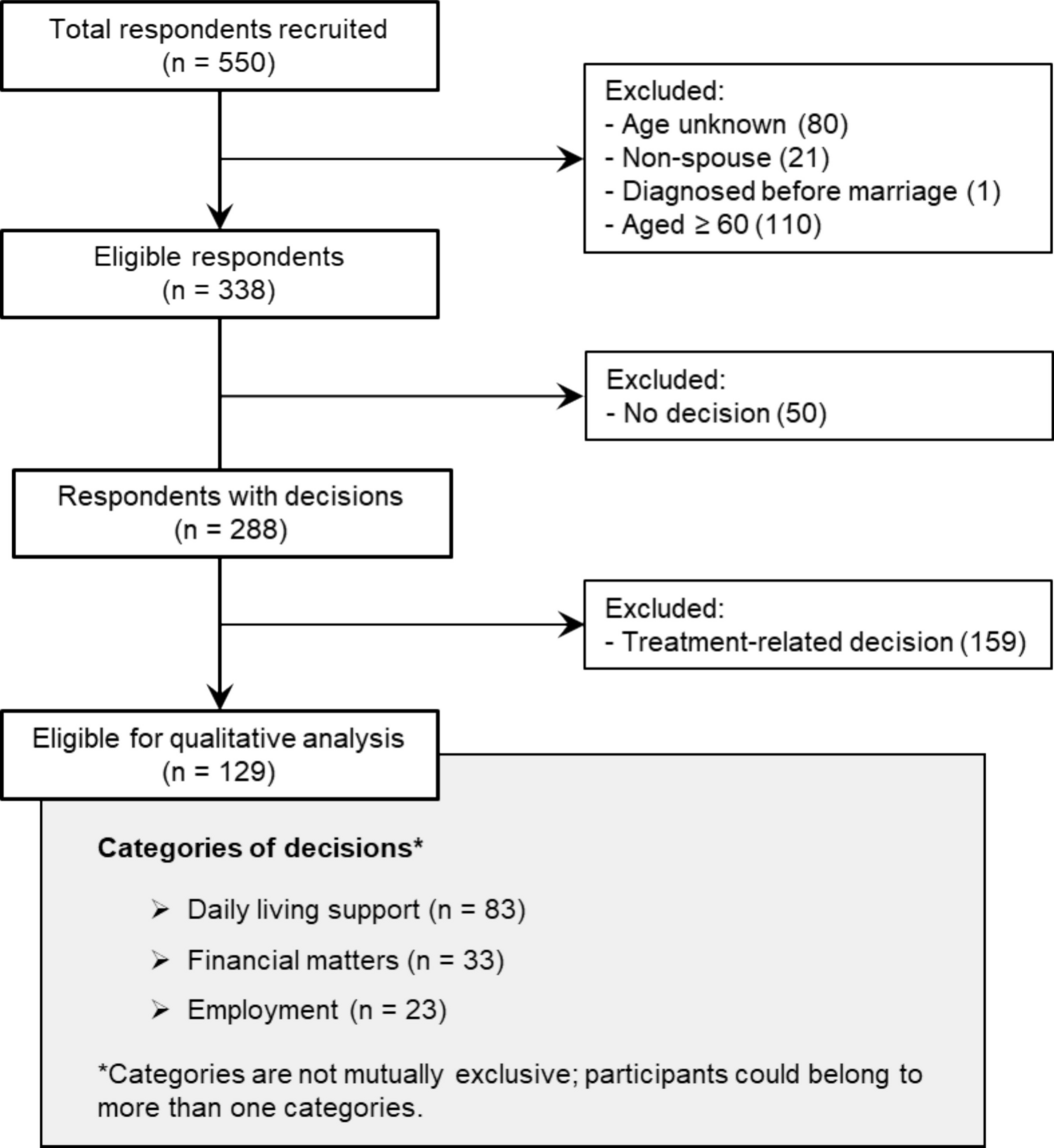
Literature from bibliographic databases resulted in 3481 records identified. Once duplicate records and conference abstracts were removed, 1950 records had titles and abstracts screened, excluding 1840 records and retaining 110 full-text reports for full-text screening. An additional 221 records were identified through supplementary sources, including trial registries, Google search, and targeted searches, and assessed for eligibility. One large trial [18], identified through Google Scholar notifications, that satisfied the inclusion criteria was published after our search cut-off date. Given its size and relevance to the topic, and in line with best practice guidelines for systematic reviews [19,20,21], we included it in the analysis for this review and have noted this deviation from the original protocol. In total, 18 records met the inclusion criteria and were incorporated into the final review: 10 guidelines; 4 completed trials; and 4 trial registrations. The PRISMA flowchart is presented in Fig. 1.
Fig. 1
PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Quality appraisalClinical guidelinesQuality assessment of guidelines is presented in Table 2. Most guidelines demonstrated strong performance in the domains of Scope and Purpose, and Clarity of Presentation, reflecting clearly defined objectives and well-structured recommendations. However, variability was noted in Stakeholder Involvement and Editorial Independence, with some guidelines lacking transparency regarding funding sources or the inclusion of consumer perspectives. The Rigour of Development domain was generally well addressed, particularly in guidelines that incorporated systematic evidence reviews and formal consensus processes. The mean quality score for the included guidelines was 4.4 (SD = 0.97), indicating moderate quality.
Table 2 Guideline characteristicsTrialsRisk of Bias (RoB) assessment for each trial is presented in Table 3. A mix of ‘low’ (n = 1) and ‘some concerns’ (n = 3) for risk of bias was evident across studies. Common strengths included clear reporting of outcomes and use of validated patient-reported outcome measures (PROMs) and experience measures (PREMs). Limitations included small sample sizes, lack of blinding, and incomplete reporting of allocation procedures.
Table 3 Trials and trials registry characteristicsIncluded document characteristicsGuidelinesCharacteristics of included guidelines are presented in Table 2. Of the 10 clinical guidelines included, 60% (n = 6) were Clinical Practice Guidelines, 20% (n = 2) Optimal Care Pathways, 10% (n = 1) Principles of Best Practice, and 10% (n = 1) were Practice Recommendations. Regarding location, 40% (n = 4) were developed for Australia, 20% (n = 2) United Kingdom, 10% (n = 1) Germany, 10% (n = 1) United States, and 20% (n = 2) multinational. Target populations of the guidelines ranged from 15 to 25 years. Recommendations from guidelines (Table 4) were mapped against three transition phases (preparing for transition, during care transition, after care transition), domains of care, allowing for comparative synthesis.
Table 4 Guideline recommendationsTrialsOf the four included published trials, all were single-arm trials, with 50% (n = 2) conducted in Canada, 25% (n = 1) in Switzerland, and 25% (n = 1) in the United States (Table 3). The sample sizes of the published trials ranged from 10 to 40 (mean = 23.8, SD = 15.0), with a total number of 95 participants across the trials. Seventy-five percent of the published trials (n = 3) reported the sexes/genders of their participants, with 51.8% (n = 44) of participants across these trials being female. Most of the published trials either reported the mean (25%, n = 1) or median (50%, n = 2) age of participants at the time of diagnosis and assessment. Median and mean age at diagnosis was 8 years and 10.75 years, respectively; whereby the range of ages of participants at diagnosis was 1.5 years to 32 years. Seventy-five percent (75%, n = 3) of the published trials reported the cancer types of their participants, with 25% (n = 1) of included trials focusing exclusively on brain tumours, 25% (n = 1), 25% on focusing exclusively on Leukemia, and 25% (n = 1) including multiple cancer types (primarily Leukemia/Lymphoma = 41% and central nervous system = 18%). Of the included trials, 75% (n = 3) reported lived-experience intervention in their design and delivery. Half of the trials (50%; n = 2) utilised a multimodal intervention (multi-pronged model of care), 25% (n = 1) workshop intervention (education and skill building), and 25% (n = 1) self-directed planning intervention (workbook). The primary outcome domains of assessment varied considerably across the trials. Across the four trials, primary outcome domains included transition readiness (25%, n = 1), perceived self-management ability (25%, n = 1), cancer worries (25%, n = 1), confidence and self-efficacy (50%, n = 2), knowledge (25%, n = 1), as well as indices related to evaluations of the transition intervention itself, including understandability and actionability (25%, n = 1), and overall impression of the intervention (25%, n = 1).
The four included registered current trials are presented in Table 3, of which 50% (n = 2) were randomised control trials, 25% (n = 1) were single-arm trials, and 25% (n = 1) were quasi-experimental (non-randomised) 3-arm trials. Twenty-five percent (n = 1) are being conducted in the United States of America, 25% (n = 1) in Germany, 25% (n = 1) in France, and 25% (n = 1) in Switzerland. The target sample sizes of the registered current trials ranged from 60 to 1600 (mean = 525.0, SD = 732.6), with a total number of 2100 target participants across the trials. None (0%, n = 0) of the registered current trials specified particular target sexes/genders, and 50% (n = 2) specified a target age range at diagnosis (0–19 months of age, and = <18 years, respectively). All trials specified their target age, which differed across each individual trial but ranged between 15 and 25 years (see Table 3). None of the registered current trials specified specific cancer types targeted nor lived-experience input in the development or conduct of the trial. Fifty percent (n = 2) of registered current trials are utilising a multimodal intervention (multi-pronged model of care), and 50% (n = 2) are utilising an educational intervention (knowledge and skill building). Like the published trials, the primary outcome domains of assessment varied considerably across the registered current trials, with 10 different outcomes being measured (see Table 3). The only endpoint being measured by more than one trial is self-management skills, being measured across two trials currently underway (50%). Aims and outcomes of the completed trials and the aims and efficacy outcomes to be assessed for the current trials are presented in Tables 5 and 6, respectively.
Table 5 Trial aims and outcomesTable 6 Trials registries aims and outcome measurementsNarrative synthesisFigure 2 presents key overarching commonalities across the guidelines, which are explored in greater depth in the sections below, alongside a discussion of notable differences.
Fig. 2
Key overarching commonalities across the guidelines. Note. This figure presents key overarching commonalities among a number of the guidelines. It is not exhaustive and does not represent the content of each guideline.
Guidelines Preparing for transitionPreparation for health service or care transition is universally recognised as a foundational phase in ensuring continuity and quality of care for young people moving from paediatric to adult health services [39, 40]. Across guidelines, early and proactive planning is emphasised as essential to mitigating risks and promoting engagement (see Table 4). Kerr et al. [28], Potter et al. [29] and the Clinical Oncology Society of Australia (COSA) [25] advocate for the development of individualised transition plans that are responsive to the young person’s developmental stage, psychosocial context, and future care needs. These plans are ideally initiated at diagnosis and refined over time. The Agency for Clinical Innovation [22] proposes a structured framework focusing on early preparation. Cancer Council [23, 24] and Tonorezos et al. [30] similarly stress the importance of education regarding long-term risks and the provision of communication tools to support navigation of adult services. Gebauer et al. [26] and Wams et al. [18] extend this approach by recommending the formation of multidisciplinary care teams and institutional policies to support health service and care transition planning. The consistent recommendation to appoint a care transition coordinator [18, 26, 29] reflects a growing consensus on the need for dedicated roles to facilitate continuity and advocacy. Several guidelines draw on lived experience and trauma-informed care principles [22, 29], while others are informed through multidisciplinary expert consensus and international frameworks.
During care transitionHealth service and care transition phases are characterised by a need to maintain continuity, foster autonomy, and ensure psychosocial safety. COSA [25], Cancer Council [23, 24] and Heitzer et al. [27] highlight the importance of sustained relationships and the provision of emotional and practical support. Effective communication between paediatric, AYA, and adult cancer services is a central theme in the guidelines by Potter et al. [29] and Tonorezos et al. [30], who also advocate for shared responsibility and joint working models. Kerr et al. [28] and Wams et al. [18] recommend joint consultations and flexible timing of transfer, tailored to individual readiness and stability; and Gebauer et al. [26] propose a structured model involving regular multidisciplinary meetings and risk stratification at the initial late effects consultation. Heitzer et al. [27] emphasise the integration of familial resources and community advocacy, particularly for survivors of paediatric brain tumours. These approaches reflect a shift toward holistic, person-centred care that is well supported by expert consensus.
Following care transitionPost-transition management is increasingly recognised as a long-term process requiring sustained engagement, surveillance, and evaluation. Kerr et al. [28], Tonorezos et al. [30], and Gebauer et al. [26] recommended ongoing psychosocial support, survivorship planning, and structured follow-up that includes ongoing surveillance for treatment-related complications, including cardiac toxicity, pulmonary dysfunction, endocrine disorders, neurocognitive impairment, infertility, and secondary malignancies, as well as the psychological wellbeing. Cancer Council [23, 24] and COSA [25] advocated for access to tailored survivorship care plans and support mechanisms to promote adherence and wellbeing. Heitzer et al. [27] extend this model by incorporating neuropsychological evaluation and vocational planning, with a focus on promoting functional independence. Wams et al. [18] and the Agency for Clinical Innovation [22] emphasise institutional-level evaluation of transition quality, incorporating survivor feedback and outcome data to inform continuous improvement.
Domains of careGuidelines span a wide array of care domains, underscoring the complexity and multidimensionality of care and health service transition planning, including but not limited to physical health and late effects, psychosocial and emotional wellbeing, familial and cultural considerations, educational, vocational, and financial support, and spiritual and developmental needs.
Trials and trial registriesIntervention design and deliveryDespite methodological variation, all interventions aimed to enhance autonomy, self-management, and long-term engagement. Digital and hybrid models featured prominently in both current and published trials (60%). For example, Devine et al. [35] are piloting a mobile-based self-management and peer mentoring programme for young adults, with an equity lens through Hispanic oversampling. Further, Entz-Werle et al. [36] are evaluating OnKO-TnT, a mobile app supporting AYA survivors’ therapeutic and educational navigation. Ryan et al. [34] developed a structured workbook (Life After the Janeway), while Carrier et al. [32] delivered psychoeducational workshops for paediatric brain tumour survivors (PBTS) and caregivers.
Structured care pathways were also commonly engaged. Jin et al. [33] implemented the GREAT Survivorship Clinic, combining medical review with AYA-specific counselling and primary care provider (PCP) liaison. Schmidt et al. [37] are trialling a multidisciplinary, guideline-concordant model with psychosocial counselling, while Scheinemann et al. [38] are assessing, and Buehlmann et al. [31] have assessed, longitudinal transition pathways across Swiss cancer centres. All interventions addressed multiple domains: medical, psychosocial, cognitive, vocational, and reproductive.
Key outcomesAcross studies, patient-reported outcomes were especially prevalent. Improvements were noted in transition readiness [32], self-efficacy [32], and cancer knowledge [31]. Jin et al. [33] reported enhanced confidence and PCP communication, while Ryan et al.’s workbook scored highly on usability (PEMAT-P: 94%) [34]. However, persistent gaps were identified with awareness of fertility and secondary malignancy risks remaining low [31], and systemic barriers such as insurance navigation and PCP linkage persist [33]. Regarding current trials, similar key outcome domains as the published trials are typically being used. For example, Entz-Werle et al. [36] are examining engagement and perceived benefit, and Schmidt et al. [37] are assessing self-efficacy.
Feasibility and acceptabilityAll studies that assessed health service and care transition intervention feasibility and acceptability demonstrated positive results. For example, retention was strong (e.g., 83% in Carrier et al. [32]), and satisfaction ratings were consistently high (e.g., 95% in Jin et al. [33]). Digital tools were well received but required attention to technical quality and interactivity. Recruitment challenges were common, particularly among underserved populations, highlighting the importance of equity-focused strategies.
Comments (0)