
Remember me
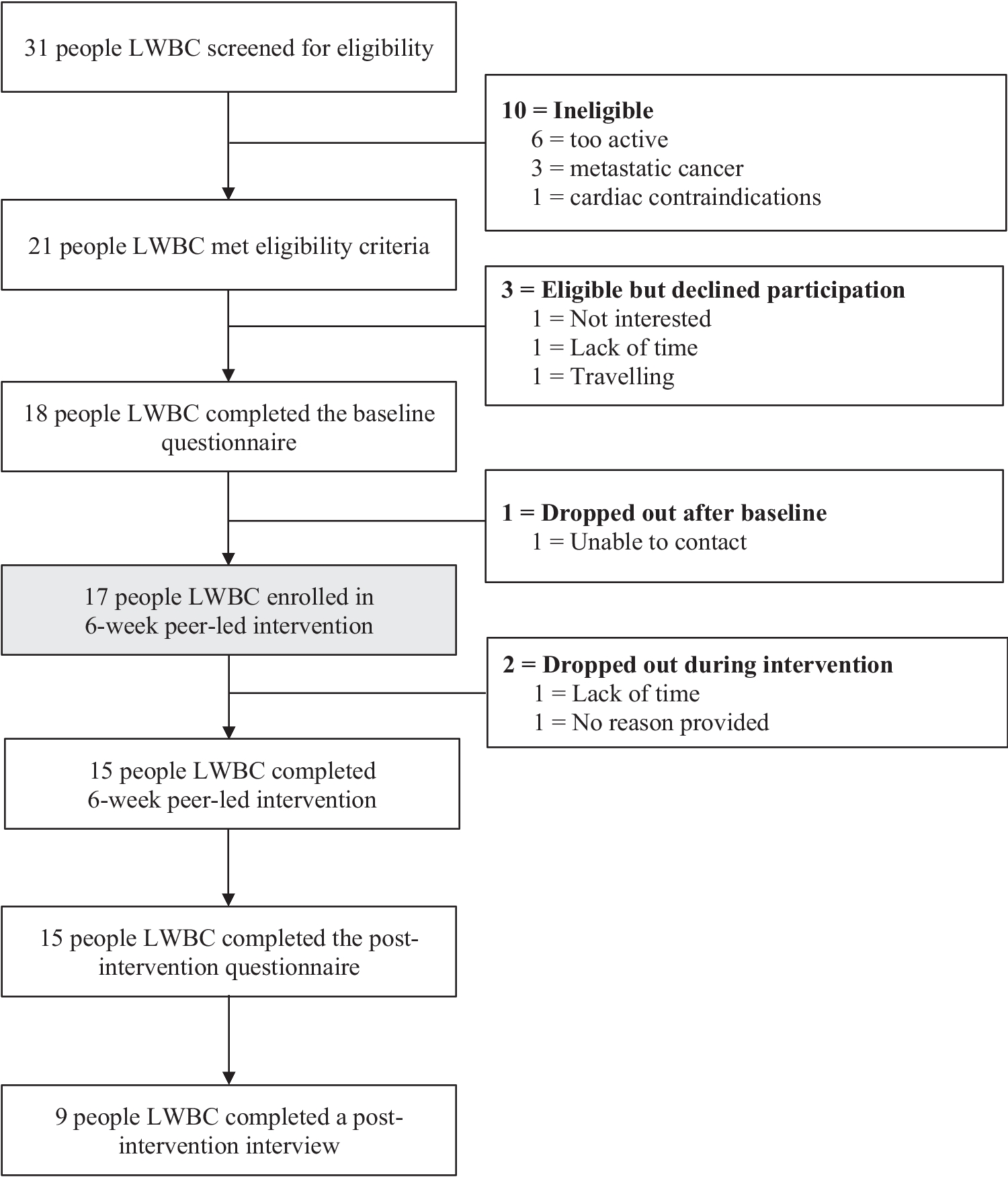
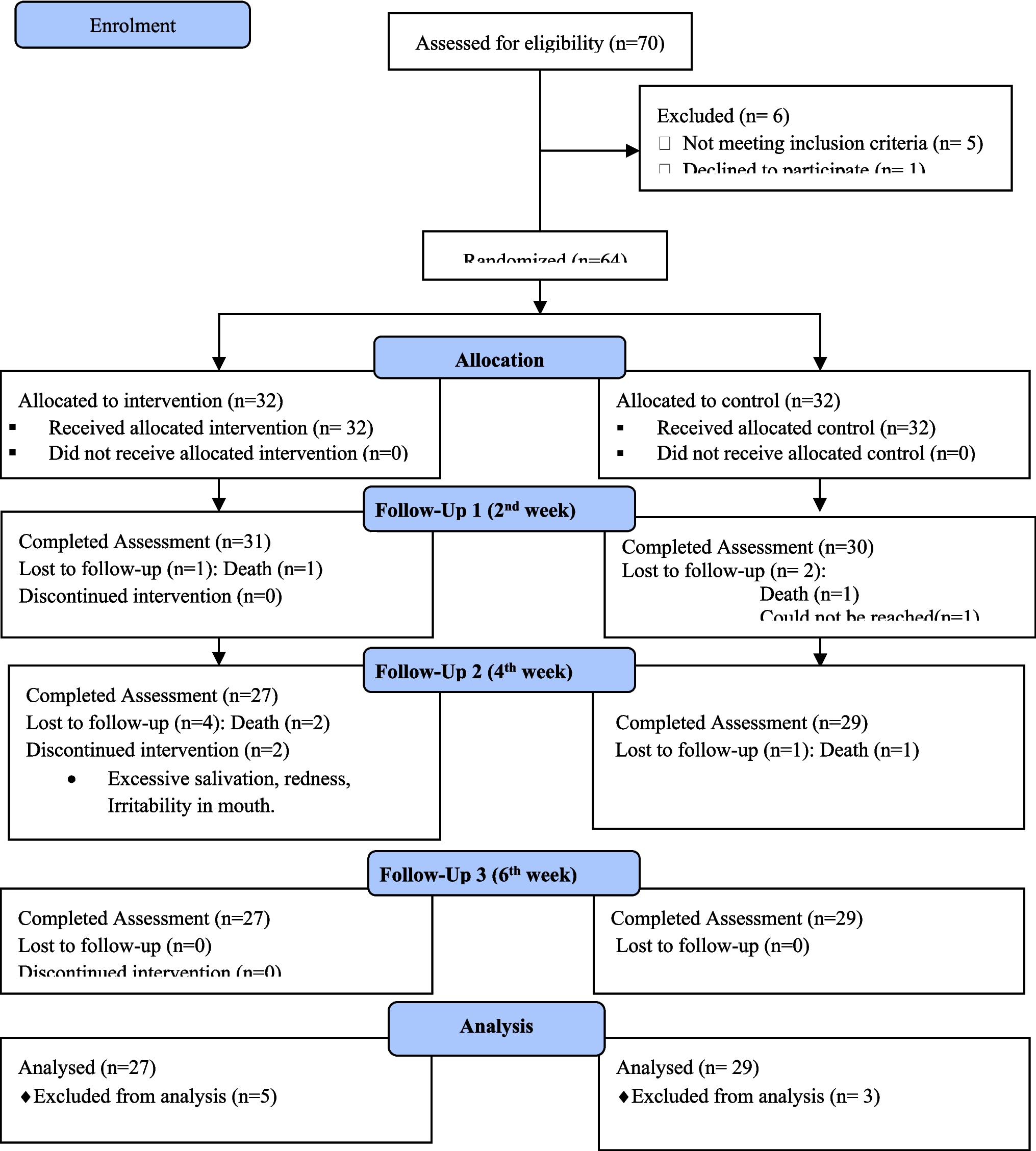

A qualitative approach was taken using positive deviance theory [17], with analyses informed by a framework method [18]. The methodological approach is presented visually in Fig. 1.
Fig. 1 Setting
SettingThis study took place within a Queensland cancer care service at a quaternary referral hospital located within the largest public health service in Australia.
ParticipantsA purposive sampling approach was used to recruit participants with direct experience in cancer care delivery. Sampling was stratified by professional role to ensure representation from oncology nurses and specialist health professionals, reflecting their distinct functions within the care pathway.
Recruitment continued until no new findings were identified.
Guiding theoretical frameworkPositive Deviance Theory was used as the theoretical framework for this study [17, 19, 20]. Positive deviance is a strengths-based approach that draws on existing knowledge, behaviors, and successful strategies already present within local healthcare teams. It assumes that healthcare workers may not always recognize the factors that contribute to their own successful practices and that these practices may not yet be formally articulated or embedded in routine care. There are four core stages: (i) define the problem and current practices influencing symptom management; (ii) determine existing strategies; (iii) discover examples of high-quality symptom management; and (iv) develop solutions based on these insights. In this study, Positive Deviance Theory informed the development of the interview and focus group guides by shaping the questions used to elicit examples of effective practices and local solutions. The final “Develop” stage will be reported separately as part of the subsequent co-design process. Although the theoretical framework informed data collection, the analysis itself was conducted inductively using Gale et al.’s framework method [18], allowing key symptom management strategies to emerge from the findings without imposing a priori categories.
Study proceduresIn summary, two datasets were collected. Separate datasets were established for methodological reasons, as the functional nature of the roles in each participant group is distinct. Patients may interact with multiple oncology nurses throughout their cancer journey within a unit that typically operates as a coordinated team. In contrast, specialist health professionals (such as oncologists, allied health clinicians, senior nurse specialists) generally interact with patients and often work independently. To align with these differing practice structures, focus groups were conducted exclusively with oncology nurses, while individual interviews were conducted exclusively with specialist health professionals. There was no overlap between the two participant groups.
Questions for data collection in both datasets included the following:
1.Do you think we have pathways in place for managing symptoms?
2.What formal pathways do we have?
3.What informal pathways are there?
4.What do you think influences the quality of symptom management?
5.What role does each healthcare worker group have?
6.What do you think healthcare workers are doing to ensure the quality of symptom management?
7.What strategies do they use?
8.How do you know that symptom management is of a high quality?
9.How is this achieved?
Dataset 1: Oncology nurse focus groupsThe focus groups were approximately 45 minutes in length questions in the guide. A semi-structured approach was taken. Each focus group was recorded and transcribed verbatim in a de-identified format.
Dataset 2: Interviews with specialist health professionals.Structured interviews, approximately 30 minutes in length. A structured interview template was used and responses were written down. Participants were given the opportunity to consider and review the written responses and provide further details as required.
Data analysesA female clinical research nurse (FB) with experience in qualitative research support roles conducted the focus groups and interviews, supported by an external facilitator clinician researcher with a PhD and 20 years of qualitative research experience (NR). Both were known to healthcare teams. Memos were collected during all meetings for reflexive monitoring and for rigor during reporting by FB and NR. The process for analysis was inductive in nature [21, 22] and informed by the steps outlined in the framework method [18]. Transcripts from dataset 1 were initially coded after two focus groups by both FB and NR independently. An analytical framework was then developed during a meeting with FB and NR and then applied to the first two transcripts again by FB. FB and NR met again and then determined after discussion that it could be applied to the remaining transcripts, with at least two researchers working independently on each transcript.
Data from dataset 2 were initially coded independently by FB and NR from the first two interviews to develop an analytical framework, which was then applied to the remaining interviews. A research assistant (KC) with 2 years qualitative experience and NR conducted an independent application of the analytical framework on all transcripts.
When researchers came together at each step to discuss their findings, disagreements were addressed until consensus was reached. Reflexive memos by FB and NR were discussed with all team members at the step of charting the data into the framework matrix. Dataset 1 and dataset 2 were analyzed separately until stage 6 of the framework method approach (interpreting the findings). These findings were then explored together to interpret the data, drawing upon memos/diarized notes and documented impressions. Similarities and differences were noted; connections were mapped into tables [23].
ReportingReporting of qualitative work used the COnsolidated criteria for REporting Qualitative research (COREQ) [24].
Ethical considerationsThis study received low-risk ethical approval (LNR/2019/QRBW/60332) by the Royal Brisbane and Women’s Hospital Human Research Ethics Committee (EC00172). The research was performed in accordance with the Declaration of Helsinki. One-page information sheets explaining the nature of the project, voluntary participation, and data management were distributed to all staff by email and presented on noticeboards across staff areas. Hard copy information sheets were also provided to healthcare teams and consumer representatives prior to arranging a suitable time for participation in qualitative data collection. The information sheet was re-presented at each data collection so consent could be confirmed. All data were de-identified and stored on password-protected servers in a non-identifiable format. A standard operating procedure for withdrawal from study participation was in place, if required.
Comments (0)