In this large, long-term cohort of patients with NF-PitNETs, we analysed the natural history of tumours managed with active surveillance and the outcomes of those undergoing TSS and multimodal treatment. The results highlight the marked biological and clinical heterogeneity of NF-PitNETs and reveal some prognostic determinants which may guide individualized management strategies.
Among the 90 patients managed with active surveillance, radiological progression occurred in 27.8%, consistent with historical series reporting growth in approximately 25–50% of untreated NF-PitNETs over 4–6 years of follow-up [9, 28, 34, 35]. The cumulative probability of progression steadily increased over time, reaching 37.2% at 5 years and 64.1% at 10 years, consistent with the concept that NF-PitNETs exhibit slow but continuous growth in a substantial subset of patients.
A clinically significant difference in growth risk was observed between macroadenomas and microadenomas (47.1% vs. 22.5% at 60 months), similar to that reported by Karavitaki and colleagues [34], with faster growth in larger tumours. Baseline tumour volume was a significant predictor of progression in univariate Cox analysis, confirming the predictive role of initial size reported in previous observational cohorts [36]. Age and sex had no impact on natural history, consistent with previous reports showing that demographic variables are not strong predictors of progression risk [34, 36]. Similarly, baseline pituitary hormone deficits were not associated with a higher risk pf tumour growth in our cohort, suggesting that endocrine dysfunction at diagnosis likely reflects the mass effect of larger tumours rather than intrinsic tumour aggressiveness.
Visual impairment at baseline also correlated with progression risk in univariate analysis. Although this association lost significance in multivariable modelling, its presence suggests that tumours large enough or positioned such that they compress the optic chiasm may possess features associated with increased biological activity, as suggested by Fountas et al. [9], who demonstrated similar associations in conservatively managed NF-PitNETs. This observation is consistent with our findings since lesions that abut or compress the optic chiasm, were also those with the highest probability of growth.
Conversely, cavernous sinus invasion assessed by Knosp grade, was not associated with tumour progression in our cohort. In contrast, the combined anatomical invasiveness score correlated with growth. These findings suggest that vertical extension into the suprasellar cistern may be more strongly associated with the risk of tumour growth than parasellar invasion alone.
An important functional outcome was the development of new pituitary hormone deficits, which occurred significantly more frequently in patients whose tumours grew during follow-up (20% vs. 4.6%). This relation emphasizes the importance of an increasing mass effect in the genesis of pituitary dysfunction, in line with prior studies where progressive growth proved a major risk factor for new endocrinopathies [9, 37]. Conversely, the worsening of pituitary function is rarely observed for stable lesions. These data confirm the necessity for routine endocrine evaluation in patients with documented radiological progression while suggesting that in stable lesions, hormonal monitoring can be tailored to clinical context.
Most of the 85 patients submitted to TSS were operated within the first year of diagnosis. For these patients, postoperative outcomes were strongly influenced by the presence of residual tumour. Complete resection resulted in excellent long-term disease control, with only one documented recurrence; this confirms results of previous studies indicating postoperative residue as the most powerful predictor of future treatment needs [18, 38]. Patients with incomplete resections had a significantly lower event-free survival, with even a trend suggesting that higher residual volume may predict an earlier progression.
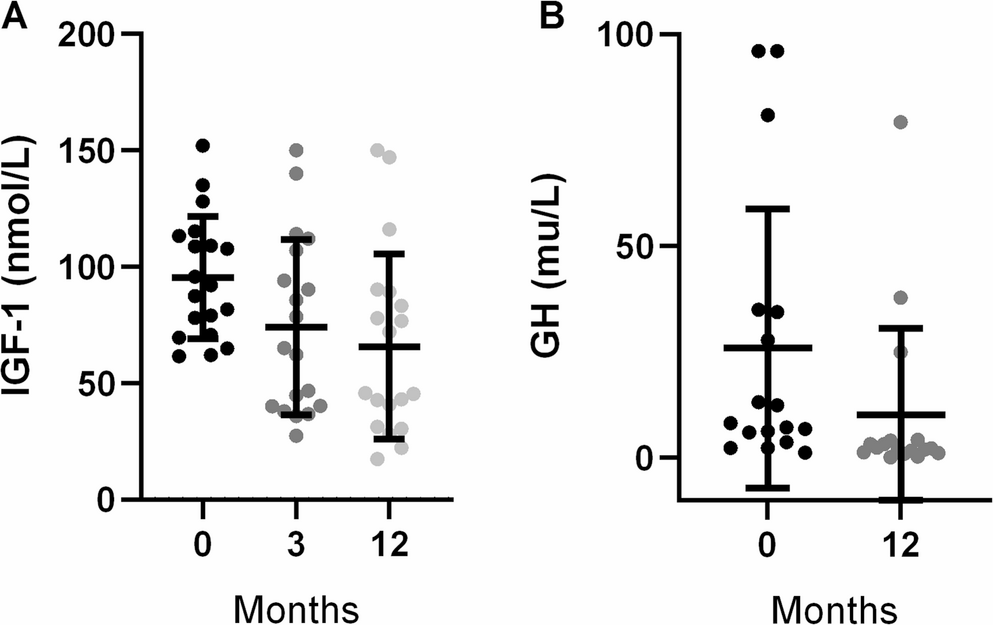
The early postoperative period was associated with a very high incidence of new hormone deficits (65.9 events per 100 person-years during the first six months), thereafter, rates markedly declined reflecting a major contribution of surgical manipulation rather than tumour progression on pituitary disfunction. The incidence of new postoperative deficits in our cohort was higher compared to that reported by Fountas et al. [9] but similar to that described by Zhang et al. [39]. The absence of postoperative residue did not protect against new deficits, further reinforcing that hypopituitarism largely reflects immediate surgical impact. There was no evidence of any tumour growth among those receiving GH replacement, consistent with the lack of impact on recurrence risk demonstrated by van Varsseveld et al. in NF-PitNETs [40], confirming the safety of this therapy.
Improvement in visual fields at 6–12 months was observed in approximately half of patients who had baseline deficits, and a reduction in tumour volume of more than 40% was significantly associated with recovery. These findings suggest that substantial decompression, rather than complete resection, is a key determinant of functional improvement. Similar results were reported by Dekkers et al. [41], who reported progressive visual recovery during the first postoperative year independently of complete tumour removal.
Our findings highlight the impact of anatomical complexity on surgical outcomes. As expected, cavernous sinus invasion, reflected by higher Knosp grades, limited the extent of tumour debulking, reinforcing the well-recognized challenge of achieving complete resection in these cases. Interestingly, chiasmal compression and the combined anatomical score showed only a weaker association with reduced debulking and postoperative residue; among patients with residual tumour, chiasmal proximity appeared to predict subsequent growth or the need for additional intervention. This suggests that suprasellar extension may capture aspects of biological aggressiveness not fully reflected by parasellar invasion alone, emphasizing the value of accurate anatomical assessment in risk stratification and surgical planning.
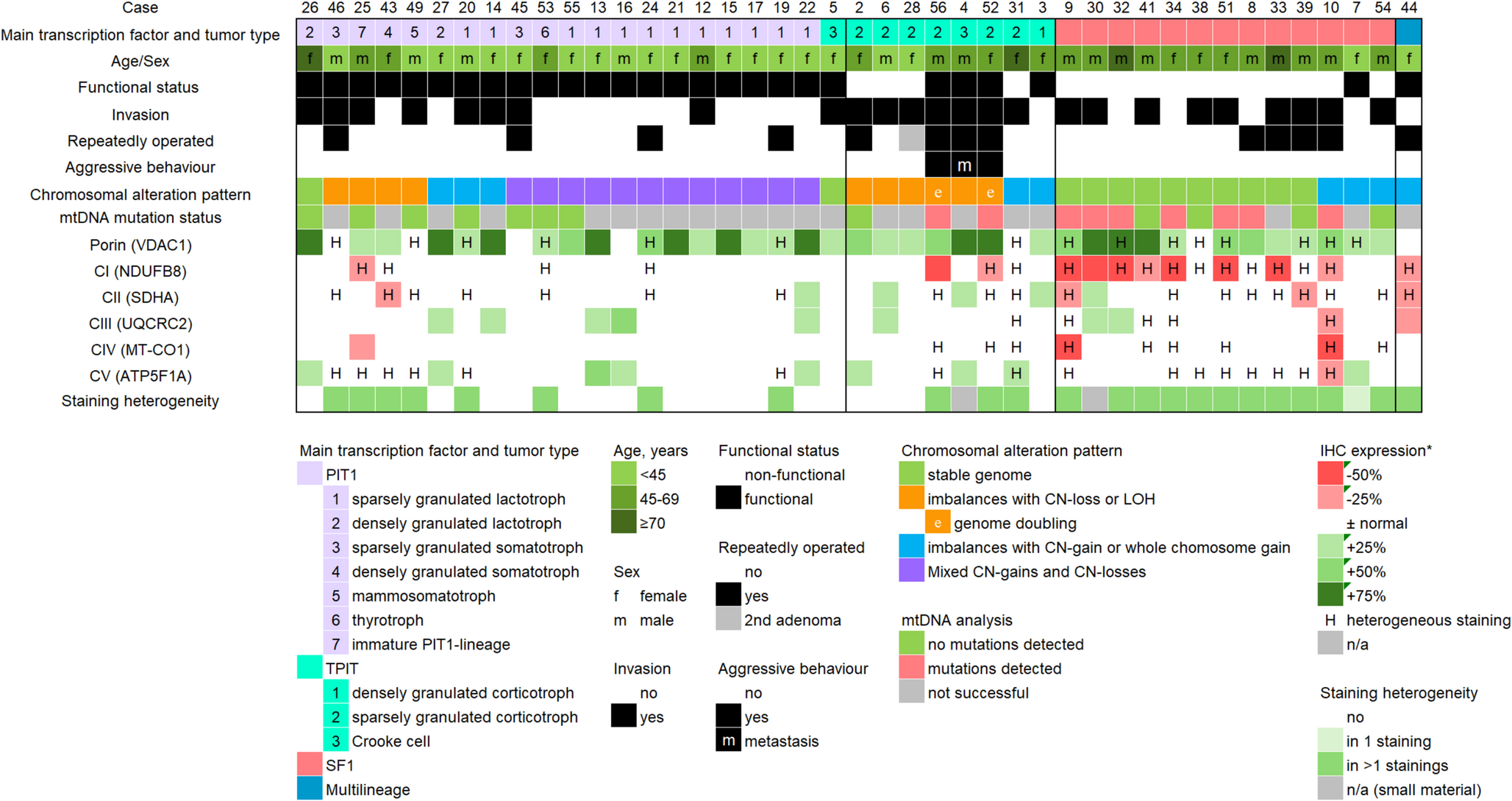
Immunohistochemical analysis confirmed silent gonadotroph tumours as the predominant NF-PitNET subtype, consistent with large surgical series and supporting the dominance of the SF1-lineage in these lesions [42, 43].
No significant association emerged between the Trouillas clinicopathological classification and tumour progression or the need for additional treatment in our cohort. Previous studies have suggested that the invasive and proliferative components of this classification may identify pituitary neuroendocrine tumours with a higher risk of recurrence or progression [44,45,46]. The lack of association observed in our series may be related to the relatively limited number of patients with available Trouillas grading, particularly within the proliferative subgroups, which may have reduced the statistical power to detect potential differences.
Second TSS showed the practical challenges posed by remnants in anatomically restricted areas. Smaller reductions after second surgeries likely reflect both more complex tumour geometry and possibly more aggressive tumour biology. Adjuvant stereotactic radiosurgery provided disease stability in the majority of patients, consistent with reported 5–10-year control rates of 85–95% [47]. Only one SRS-treated patient progressed, and new endocrinopathies were infrequent. Temozolomide (TMZ) with minimal new endocrinopathies. Temozolomide, used selectively in refractory or aggressive tumours, stabilized disease in two of three cases, echoing the reported response rate of approximately 40% [48] and reinforcing its role as a therapeutic option in highly resistant pituitary tumours [49].
Gender-related differences were evident in tumour presentation and outcomes. Male patients presented with larger tumours and consequently higher rates of visual and endocrine dysfunction, supporting prior observations that men often present with more pronounced mass-effect symptoms due to later detection [8]. In contrast, women in the active surveillance group were younger and had smaller tumours, likely reflecting earlier or incidental detection during the reproductive years, often prompted by menstrual irregularities or mild hyperprolactinemia.
Among the surgical cohort, females achieved complete resection more frequently and experienced fewer postoperative hormonal deficits and lower rates of visual impairment. These differences likely stem from males harbouring larger tumours closer to the optic chiasm-factors known to complicate surgical removal and increase the risk of pituitary injury [39]. Nevertheless, consistent with previous reports, TSS provided meaningful visual improvement in both sexes, particularly in patients with severe preoperative chiasmal compression [41].
Overall implications
Taken together, these findings highlight several important points. Firstly, NF-PitNETs require a personalized risk assessment that incorporates not only tumour size and clinical presentation but also anatomical features, such as suprasellar extension and optic chiasm abutment, which in our cohort were stronger predictors of growth than cavernous sinus invasion. These radiological markers, combined with early postoperative imaging, provide a more detailed and nuanced approach to understanding tumour behaviour. Secondly, despite the limited prognostic value of proliferative markers and the Trouillas classification in our cohort, anatomical and volumetric features remained key determinants for clinical surveillance and surgical planning. Multimodal therapy, which may include radiosurgery and TMZ, should be considered for not fully resectable tumours with features of biologically aggressiveness.
Finally, gender-related differences appear driven primarily by tumour size at diagnosis rather than intrinsic biological variation, underscoring the importance of timely detection to reduce visual and endocrine morbidity. Upcoming efforts should be devoted to establishing integrated predictive models that combine clinical, radiological and molecular features, in order to facilitate long-term risk stratification and personalize management strategies.


Comments (0)