Current role of Cabergoline and surgical indications
Cabergoline (CAB) remains the gold standard for treating prolactin-producing pituitary adenomas (prolactinomas) due to its high efficacy in normalizing serum prolactin (PRL) levels and reducing tumor volume [1,2,3,4,5,6,7,8,9,10], even in the presence of visual impairment [10]. Compared with older dopamine agonists (DAs) such as bromocriptine and terguride, CAB offers milder and fewer side effects [1,2,3,4,5,6,7,8,9,10]. In 2010, Klibanski comprehensively outlined surgical indications for prolactinomas, including tumor progression despite optimal medical therapy, pituitary apoplexy, DA intolerance or resistance, fertility-seeking women with DA-resistant microadenomas or chiasmal compression, unresponsive cystic tumors, CSF leakage during DA use, and cases with psychiatric contraindications to DAs [2]. Subsequently, surgical indications for prolactinomas were reported from a neurosurgical perspective [10,11,12,13,14,15,16,17,18]. Among these, absolute indications have remained limited to CAB resistance, intolerance, and CSF leakage, while relative surgical indications include unresponsive cystic prolactinomas [10, 19,20,21] and cranial nerve palsy [22]. Other potential reasons for preferring surgery over medical therapy include avoidance of lifelong medication, cost-effectiveness [23, 24], early pregnancy planning, and improved fertility outcomes after surgery [25]. However, these factors remain inconclusive and do not establish surgery as superior. Surgical intervention should be considered only with clear indications and may be offered as a meaningful alternative to medical therapy when it can be performed safely and appropriately.
We retrospectively analyzed surgically treated prolactinoma cases between 1998 and 2008 and found that no recurrence occurred among women who conceived and delivered after achieving surgical remission. Based on this emerging finding, we propose a refined surgical indication for carefully selected pregnancy-seeking women—curative-intent surgery followed by pregnancy and childbirth after surgical remission—as an alternative to long-term dopamine agonist therapy. Since 2009, we have prospectively applied a standardized, magnetic resonance imaging (MRI)-driven candidacy strategy focused on enclosed tumors and minimal cavernous sinus invasion.
A noble surgical indication for childbearing women desiring pregnancy
Despite its potential clinical significance, neither the 2023 international consensus statement by the Pituitary Society [8] nor recent comprehensive review of prolactinoma treatments [9] addressed the relationship between pregnancy and delivery following surgical remission and recurrence. However, in our current study of 59 childbearing women who achieved remission following surgery between 1998 and 2022, none of the women who became pregnant and delivered experienced recurrence (0%, 0/29), whereas recurrence occurred in 20% (6/30) of those who did not conceive (P = 0.0237; Table 4). In our cohort, pregnancy and delivery after surgical remission were associated with an absence of recurrence. However, given the observational design, this association should be interpreted cautiously and may be influenced by selection factors related to surgical candidacy and postoperative biochemical status.
Although patients can become pregnant while on CAB therapy, continuation is usually required postpartum. Notably, the Pituitary Society guidelines recommend at least two-year period of PRL normalization without residual tumor on MRI before attempting withdrawal [26,27,28], and the likelihood of discontinuing CAB therapy after remission is not high. However, in our series, patients who became pregnant and delivered after surgical remission did not require CAB therapy postpartum and did not experience recurrence. These outcomes are consistent with the possibility of durable, treatment-free remission in carefully selected pregnancy-seeking women after confirmed complete resection. Rather than establishing superiority over CAB, our data suggest that surgery may represent a clinically meaningful option for selected patients when complete resection is anticipated and surgery can be performed safely. In this context, the potential benefit is durable remission without the need for postpartum CAB therapy.
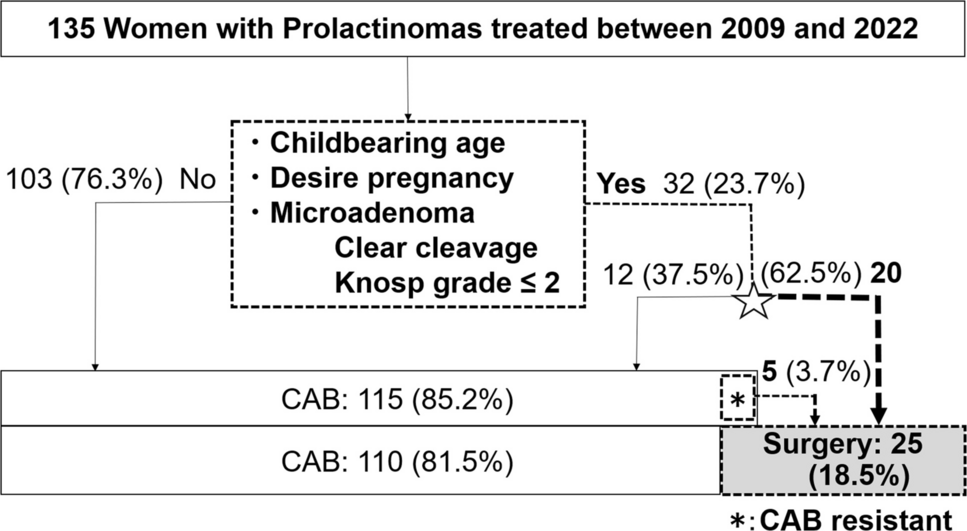
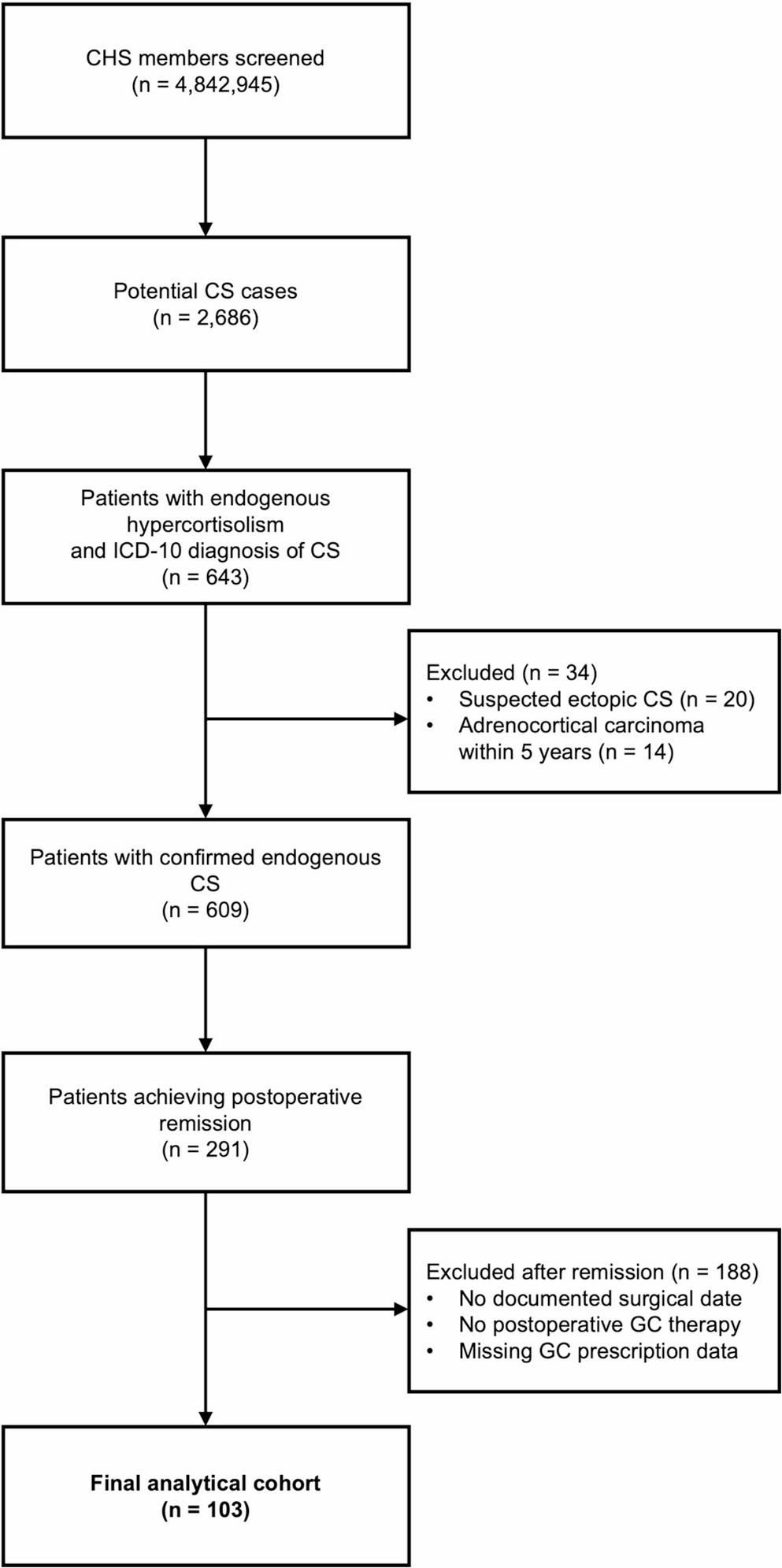
In addition to the advantage of enabling early pregnancy planning (as soon as one month after surgery) and breastfeeding after delivery, surgery offers the unique benefit of potentially achieving long-term remission. When postoperative normoprolactinemia is achieved without radiological evidence of residual tumor, patients may require only annual serum PRL monitoring. However, surgery necessitates hospitalization, carries risk of complications [29, 30], and may cause psychological distress, including anxiety about surgery. Patients must receive balanced, comprehensive counseling—on CAB therapy from endocrinologists and on surgical options from neurosurgeons. Shared decision-making is essential, as one-sided explanations may result in biased or incomplete understanding. Patients should be fully informed of both options and supported in choosing the most appropriate treatment for their individual circumstances. As a result, 20 of 32 childbearing women (62.5%) with enclosed-type prolactinomas who desired pregnancy elected surgery (Fig. 1 star).
Surgical strategy and patient selection
The number of surgically treated cases decreased over time (57 procedures in 1998–2008 vs 25 in 2009–2022). This likely reflects the broader adoption of CAB with improved tolerability compared with earlier dopamine agonist practice patterns. In addition, our approach to surgical candidacy evolved after 2009: “patient preference” was previously interpreted more broadly, sometimes including women expressing a non-specific future desire for pregnancy, and candidacy was occasionally determined predominantly within the neurosurgical service. Since 2009, we have applied more stringent, MRI-driven criteria for anticipated complete resection and a realistic near-term pregnancy plan, with multidisciplinary counseling that includes endocrinologists and final treatment selection based on informed patient decision-making.
The surgical goal in women desiring pregnancy is total tumor removal with normalization of PRL. Residual tumor necessitates postoperative CAB therapy, thereby defeating the purpose of surgery. Careful patient selection based on detailed preoperative MRI is therefore essential. Suitable candidates have enclosed tumors, a distinct cleavage plane from the normal gland, and minimal cavernous sinus invasion (Knosp grade ≤ 2) (Fig. 1). We selected Knosp grade ≤ 2 as an eligibility threshold because, in our practice, this range still allows reliable identification of an enclosed tumor with a discernible cleavage plane and a high likelihood of complete resection on preoperative MRI. We acknowledge the ongoing discussion regarding whether stricter criteria (e.g., Knosp ≤ 1) should be used to further maximize the probability of gross-total resection, and that the optimal cutoff may depend on imaging interpretation and surgical expertise. Remission rates for enclosed-type tumors improved from 52.4% (1998–July 2003) to 95.2% (August 2003–2008) (P = 0.0036, Table 1) due to technical advances in transsphenoidal surgery (TSS). However, even a 95.2% remission rate was insufficient; for women desiring pregnancy, only 100% remission is acceptable. In our series, MRI-based selection with Knosp ≤ 2 achieved 100% remission in pregnancy-seeking women without new deficits, supporting the practicality of this criterion in experienced hands. Nonetheless, these results should be interpreted cautiously and require external validation across centers with varying surgical volumes and expertise.
To achieve this, we refined endoscopic techniques, improved TSS instruments [31,32,33,34], and adopted high-definition endoscopy [35]. Furthermore, we aim to avoid over-resection to preserve pituitary function [36], which is essential for conception. PRL levels during postoperative days 1–10 (POD1–10) predicted recurrence: patients with PRL < 3 ng/mL had significantly lower recurrence than those with 3–15 ng/mL (4.3% vs. 50.0%, P = 0.0098; Table 1). Although postoperative PRL level < 3 ng/mL is ideal for minimizing recurrence, levels of 3–15 ng/mL were considered acceptable if conception was anticipated, prioritizing function preservation. In our cohort, no new postoperative hypopituitarism was identified on dynamic endocrine testing: the growth hormone, hypothalamic–pituitary–adrenal, gonadal, and posterior pituitary axes were all preserved. Accordingly, no patient required new long-term hormone replacement therapy after surgery. To reconcile these competing goals, we emphasize pseudocapsule resection [36], meticulous identification and preservation of the normal pituitary gland [35], and prevention of complications such as CSF leakage [29, 30, 32]. These procedures require an experienced pituitary neurosurgeon [13, 17]. However, even with expert surgical skill, dynamic MRI is critical for identifying the cleavage plane between the tumor and the gland. Furthermore, when the tumor extensively invades the cavernous sinus (Knosp grade > 3) [22, 37] and complete resection cannot be guaranteed, surgery should not be offered to women desiring pregnancy, even in cases of strong patient preference. Importantly, the clinical decision-making framework for surgical candidacy was not standardized in the earlier period. Before 2009, “patient preference” was interpreted more broadly and documentation of near-term pregnancy intent and MRI-based predictors of complete resection was not uniformly incorporated into the surgical indication process. Since 2009, we have implemented a standardized, MRI-driven selection strategy focused on anticipated complete resection and a realistic near-term pregnancy plan, supported by multidisciplinary counseling and informed patient decision-making. This evolution in candidacy assessment likely contributed to the reduced number of surgical cases over time and to the more consistent outcomes observed in the later cohort. Since 2009, a 100% remission rate has been achieved in childbearing women who met the surgical criteria without new hormonal deficits or complications, as a result of meticulous preoperative MRI-based case selection and advances in transsphenoidal surgical instruments and techniques. Although the difference was not statistically significant, the recurrence rate was lower in 2009–2022 than in 1998–2008 (1/10 [10%] vs. 5/20 [20%], P = 0.633). This trend may reflect refined patient selection and the higher proportion of women who conceived and delivered (44.4% [16/36] vs 56.5% [13/23], P = 0.430; Table 4). This increase may, in part, be related to strategic refinements intended to minimize ascertainment bias when assessing a woman’s intent to pursue pregnancy. If childbearing women are simply asked whether they wish to have a baby, most will naturally respond affirmatively; however, not all will be able to conceive after surgical remission due to various personal or social circumstances. Therefore, to better identify candidates for surgery with curative intent, additional factors—such as marital status, the presence of a partner, and concrete plans for conception—should be assessed preoperatively. In light of recent societal trends such as delayed marriage and childbearing and shifting attitudes toward marriage and child-rearing, we implemented a strategy that included confirming marital status or the presence of a fiancé/stable partner and requiring a commitment to conceive within two years of surgery. This 2-year benchmark was chosen based on our observation that recurrence, when it occurred, did not present earlier than two years postoperatively. In 2009–2022, recurrence occurred in only one woman who did not conceive, at 2.8 years after surgery. The proportion of women who did not become pregnant and deliver decreased from 55.6% (20/36) to 43.5% (10/23), although this difference did not reach statistical significance (P = 0.430; Table 4). This decrease may be related to the implementation of stricter selection criteria.


Comments (0)