
Remember me
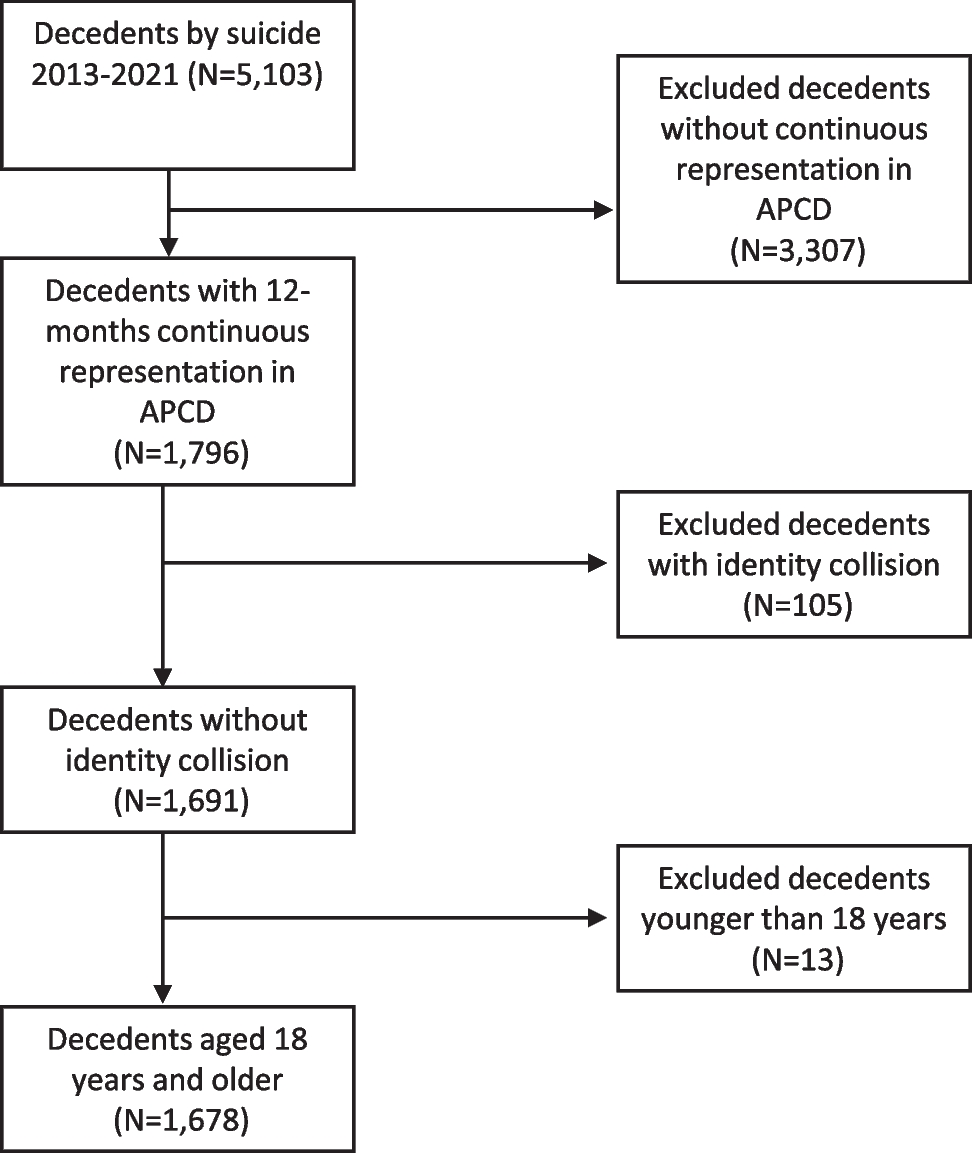
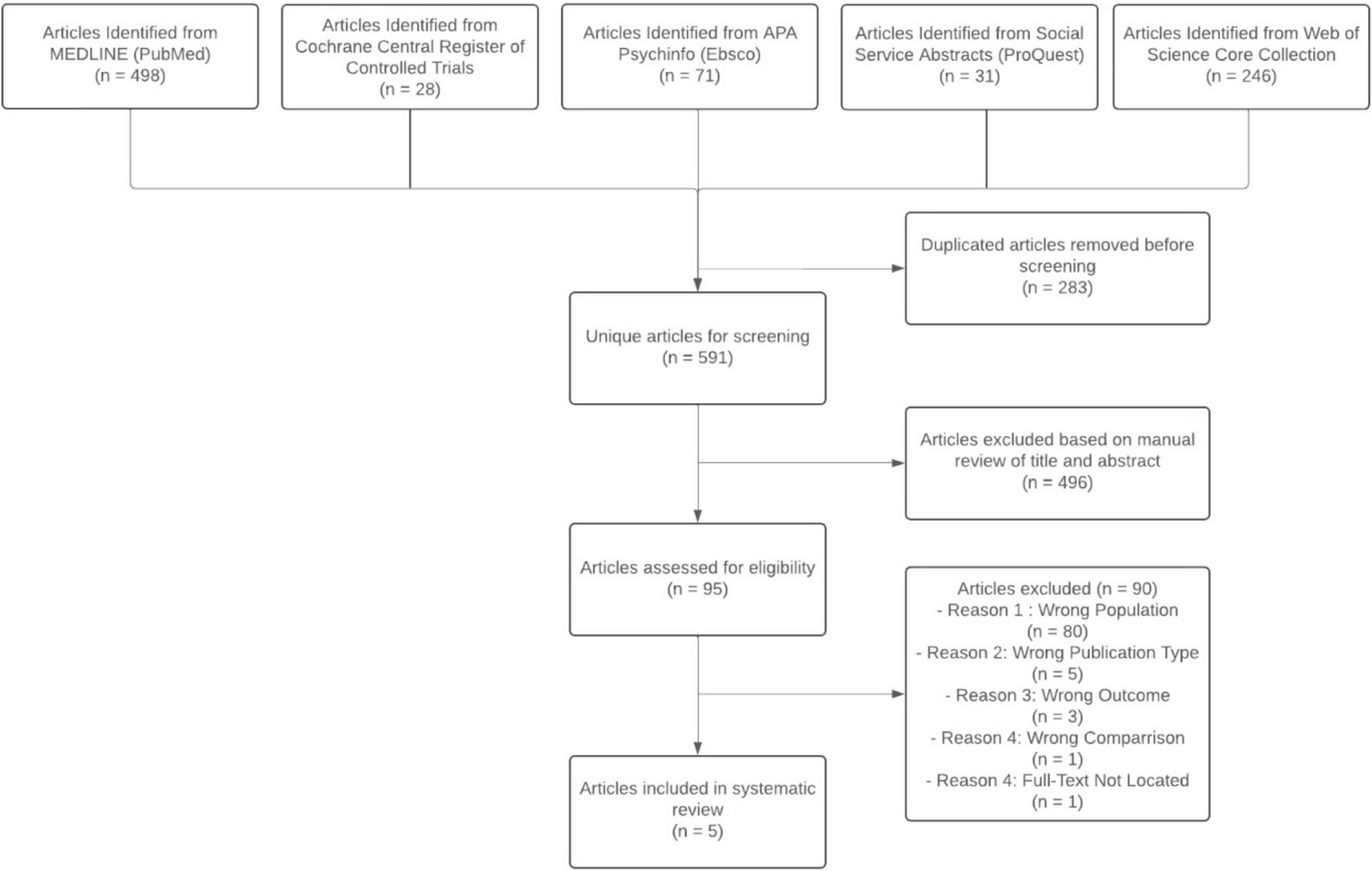

The literature search resulted in 498 articles from MEDLINE, 28 articles from Cochrane Central Register of Controlled Trials, 71 articles from APA PsycINFO, 31 articles from ProQuest, and 264 articles from Web of Science Core Collection. Then, 283 articles were duplicates, resulting in 591 unique articles for screening titles and abstracts. After screening titles and abstracts, 496 articles were excluded, leaving 95 articles for full-text review. Then, 80 of the 95 articles were excluded for studying the wrong population, five were excluded for being the wrong publication type, three were excluded for looking at the wrong outcome, one article was excluded for having the wrong comparison group, and one article’s full text could not be obtained (Fig. 1).
Figure 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.After the full-text review, five articles met the eligibility criteria. Three articles examined the impact on youth in foster care of a transition from FFS to MMC on behavioral healthcare utilization. One of these three articles also explored behavioral healthcare cost. The two remaining articles explored the utilization of well-child services.
Several articles displayed high to moderate risks in various domains like confounding, selection of participants, and missing data (Table 1). Differences in billing practices across states (e.g., use of UB-04 vs. 1500 forms for residential treatment services) may affect the comparability of utilization measures across studies. The included articles lack certain specifics, such as information about how Federal Qualified Health Center (FQHC) visits or T1015 claims were counted within the behavioral healthcare articles. Another example is that age inclusion criteria varied slightly across studies. While most focused on youth aged 0–18, some included individuals up to age 21, reflecting differences in state Medicaid eligibility for foster youth. These variations are noted in the data extraction table (Table 2).
Table 1 Risk of bias (ROBINS-I)Table 2 Summary of findingsMoreover, while Medicaid claims and encounter data, along with specific procedure and diagnosis codes, are commonly used for service definitions and counting, the comparability of utilization and cost outcomes across multiple states is not consistently addressed or fully supported by the sources. For instance, Bright, Kleinman, Vogel, et al. (2018) attempt a multistate comparison but note limitations, while the other studies are single-state focused and highlight state-specific policy and billing practice variations that could hinder direct cross-state comparisons.
Table 2 summarizes findings on healthcare utilization and costs. This table displays that managed care (MC) reduced inpatient services and improved access to primary care, while fee-for-service (FFS) had higher inpatient and residential treatment center utilization. The certainty of evidence varies, with behavioral healthcare findings rated low due to high bias, and well-child care utilization rated moderate (Table 2).
Behavioral healthcareThree included articles examined behavioral healthcare outcomes. These articles all drew from the same dataset originating from the Colorado Capitation Pilot Program.10,11,12 To prevent redundancy, a general overview of the Colorado Capitation Pilot Program is provided, followed by a breakdown of the methodologies and findings presented in each related article. The results were then synthesized into utilization outcomes and cost outcomes. All of the articles contain data on behavioral healthcare utilization,10,11,12 and one reported cost savings data.11
The Colorado Medicaid Capitation Pilot Program, initiated in 1995, aimed to reform mental health care delivery by transitioning from FFS to an MMC model. This involved implementing a capitated managed care system in previously FFS mental health treatment facilities. The state partnered with six not-for-profit community health centers to serve as the managed care organization (MCO), each responsible for a specific geographic area. The state also contracted with three joint ventures between a for-profit managed care company and several community mental health centers designated as "”for-profits.” Additionally, three mental health centers operating under the existing FFS system also participated in the pilot program by serving as the comparison group.
This pilot program aimed to assess the impact of the capitated system on behavioral healthcare utilization compared to facilities operating under the traditional FFS model, not limited to the child welfare population. Previous articles on this pilot program demonstrated that both capitated MMC models increased outpatient utilization, which includes individual and group therapy, crisis and evaluative services, case management, and day treatment programs, measured per service.10,11,12 Conversely, the cost of inpatient care, which is defined by days in a psychiatric hospital stay or acute, general hospital days identified with a mental health diagnosis, decreased among adults with serious mental illness, compared to FFS.13 Similar cost savings were observed for youth under the age of 18. However, findings regarding utilization were mixed, with more youth accessing services from for-profit MMC sites than non-profit MMC sites or FFS sites.14 Following these initial articles, researchers analyzed outcomes specific to Colorado’s child welfare population, including the three articles that met the inclusion criteria for this systematic review.
Cuellar, Libby, and Snowden (2001)10 conducted a study to examine mental health service utilization rates specific to Colorado youth involved in the juvenile justice or child welfare systems. This review includes only findings from the article pertaining to the child welfare sample. The study utilized a quasi-experimental, pre–post design with nonequivalent comparison groups, employing a two-part model to analyze service patterns. Dependent variables included the probability of service use and the number of services used (days or visits), with demographic variables and provider types as explanatory variables. Cuellar, Libby, and Snowden’s article (2001) was rated as having a high risk of bias due to confounding variables such as non-random assignment and local variability. Additionally, outcome measurement issues with user sample denominators and the exclusion of services typically covered by managed care lead to potential underestimation of costs and incomplete utilization results. Additionally, managed care plan enrollment was not randomly assigned.
Data from 1994 to 1997 was analyzed across a pre-program implementation phase and two post-implementation phases. The data was gathered from two experimental MC sites (one not-for-profit and one for-profit) and one comparison FFS site. The data was obtained through Medicaid claims, a “shadow billing” system for MCOs, and child welfare encounter data.
The child welfare sample was comprised of 9010 Colorado Child-Welfare involved youth under 18 years old, including those with in-home or out-of-home placements.10 Among the 9,010 young people, 59% were male in the pre-period, 58% in postperiod 1, and 60% in postperiod 2.10
The authors observed a decrease in the probability of inpatient service utilization, measured by days, in both not-for-profit (17%, 10%, and 10%) and for-profit managed care sites (22%, 15%, 15%) across the pre- and postimplementation periods.10 At the FFS comparison site, the probability of inpatient service use increased from 14% during the pre-period to 21% during postperiod 1 and 19% during postperiod 2.10 The number of inpatient days remained relatively stable across sites.10
The probability of utilizing outpatient services decreased in both not-for-profits and for-profit managed care sites across different study periods.10 Specifically, at not-for-profits, the probabilities were 90%, 80%, and 85% during the preperiod, postperiod 1, and postperiod 2, respectively, while for-profit sites showed probabilities of 91%, 87%, and 90% during the same periods.10 At the FFS comparison site, the probability of using outpatient services decreased from the pre-period to post-period 1 (81% to 78%) but returned to the pre-period rate by post-period 2.10
The number of individual outpatient services during a course of treatment increased significantly across all sites.10 Notably, not-for-profit managed care sites delivered an average of 16.5 services per user during the preperiod, 24 during postperiod 1, and 31.6 during postperiod 2.10 For-profits provided an average of 13.3 services per user during the preperiod, then 19.4 and 25.6 during the respective postperiods.10 The FFS site delivered an average of 13.3 services, then 19.3 and 25.4, respectively.10
Conversely, the likelihood of using RTCs (residential treatment centers) increased in both nonprofit and for-profit sites over the study periods.10 In nonprofits, the likelihood rose from 11% to 30% to 33%, while in for-profits, it increased from 12% to 21% to 24%.10 Comparatively, at FFS sites, the probability of use increased from 11% to 17% to 22%.10 Only the FFS site exhibited statistically significant changes in average days in treatment (62.6, 51.6, and 74.0, pre- and post-periods, respectively).10
Libby, Cuellar, Snowden, et al. (2002)11 examined shifts in service expenditures during the Colorado Capitation Pilot Program. Data was collected from a pre-program implementation phase and two post-implementation phases. The information was sourced through Medicaid claims, a “shadow billing” system used by managed care organizations, and data related to encounters within the child welfare system. Libby, Cuellar, Snowden, et al.’s article (2002) was also rated as having a high risk of bias, particularly in participant selection and intervention deviations, with contracts awarded based on proposals rather than random assignment. The article also highlighted cost-saving behavior due to the shift to child-welfare-covered services instead of focusing strictly on MMC services (Table 1).
The total sample consisted of 48,403 youths under the age of 19, with Medicaid claims data from October 1994 to June 1997.11 There were 3,931 child welfare–involved youth in the preperiod, 3532 in postperiod 1, and 4030 in postperiod 2.11 Service utilization and cost changes were analyzed by service type: inpatient, outpatient, and therapeutic residential treatment. Findings are represented by a regression coefficient of service use and service expenditures using a “difference in differences” methodology.
Findings regarding service utilization for the child welfare sample reveal a significant increase in inpatient and residential treatment use (81% and 42%, respectively), and outpatient use fell by 47% compared to the FFS control group.11 Findings regarding expenditures exclusively related to the child welfare sample reveal that, compared to the FFS control group, inpatient and residential treatment costs decreased significantly (23% and 65%, respectively), and outpatient costs increased (9%).11
The article’s broader conclusions, extending beyond just child welfare cases, reveal a significant trend: expenses are increasingly being redirected to services funded by child welfare budgets, rather than those covered by health insurance plans.11 Total expenditures decreased by 16%, while residential costs increased by 13%.11 These findings suggest expenditure patterns indicative of cost substitutions for services not covered by MMC.11
Snowden, Cuellar, and Libby (2003)12 examined if there are varying effects of transitioning youth in foster care to MMC by race. The study used a quasi-experimental, pre-post design involving a "difference-in-difference" analysis with nonequivalent comparison groups. It explored the shift of public mental health providers from a FFS to a capitated MMC system. The study period was divided into three time periods, reflecting one pre-implementation period and two post-periods. Snowden, Cuellar, and Libby12 examined both “access,” referring to the probability of being referred to services and “utilization,” pertaining to the amount of care received once referred. Snowden, Cuellar, and Libby (2003) was rated as having a moderate risk of bias due to lower risk in participant selection compared to other Colorado Pilot program articles, but still containing the potential confounding factors of nonrandom assignment and local variability, and possible missing data from underreporting in shadow billing datasets.
The sample of 60,324 youth was based on all state child welfare Medicaid claims data from September 1994 to June 1997.12 The three subsamples analyzed were White/non-Hispanic youth (n = 36,360), Black youth (n = 8032), and Hispanic youth of any race (n = 17,932). Then, 52% of the study population was male, and the largest age group was 5 years old (38%).12
The analysis revealed that MMC did not have a statistically significant effect by the second post-period on access for White youth in comparison to FFS.12 Black youth initially experienced increased access to care in the first post-period (23%), but this increase became statistically insignificant by the end of the second post-period.12 Hispanic youth did not experience a significant change in access during the first post-period; however, by the end of the second post-period, they exhibited a 22% increase in the probability of receiving services.12
Subsequently, changes in service utilization by service type were measured. Service types were defined as days in inpatient care, number of outpatient visits, and days in residential treatment. By the end of the study period, Black and White youth were observed to have fewer days in inpatient care under MMC than FFS, and there was no difference in days for Hispanic youth.12 The number of outpatient visits remained comparable between MMC and FSS.12 By the end of the study period, White youth were receiving an average of 3.6 visits under FFS and 3.9 under MMC, Black youth were receiving 3.2 visits under FFS and 3.4 under MMC, and Hispanic youth received slightly fewer with FFS (2.1 visits) than with MMC (2.8 visits).12
All youth received fewer days in residential treatment under MMC than FFS, with the predicted average days in residential treatment for white youth being 9.5 under FFS sites and 7.4 under MMC.12 For Black youth, the predicted average was 5.9 days and 4.9 days, FFS and MMC, respectively.12 For Hispanic youth in care, the predicted average was 5.9 days and 4.6 days.12
Using the GRADE approach, the literature regarding behavioral healthcare utilization is rated with low certainty of evidence. This low rating is attributed to the high risk of bias in the articles and their indirectness. There are concerns about the reliability and applicability of the findings related to how managed care affects the use of behavioral healthcare services, including inpatient, residential treatment, and outpatient care. The certainty of evidence for behavioral healthcare costs is also rated as low for displaying a high risk of bias and indirectness. This indicates that there is limited confidence in the accuracy of the reported cost changes associated with managed care.
Well-child visitsBright, Kleinman, Vogel, et al. (2018)15 investigated the variations in primary care, preventive care, and emergency department (ED) usage among foster youth in Texas (n = 38,569) who switched to the specialty managed care plan, STAR Health, from FFS, compared to foster youth in Florida (n = 24,611) who remained on FFS from 2006 to 2010.15 It is notable that STAR Health contains features that encourage coordinated care and provider acceptance, such as a 24-h nurse hotline. The article focused on foster youth aged 0 to 18 actively involved in cases with Title IV-E eligibility and enrolled in either Texas or Florida Medicaid during the study period. Only data on primary care and preventive care are included in this review. Bright, Kleinman, Vogel, et al.’s article (2018) was rated as having a high risk of bias due to biased participant selection, excluding youth with shorter stays in care, and unaddressed confounding variables from concurrent interventions.
Well-child visits encompass both primary and preventive care, serving the dual purpose of addressing both the immediate health needs of the child and preventing potential health issues through regular check-ups, screenings, and vaccinations. Access to primary and preventive care was assessed using age-stratified groups with continuous enrollment. For primary care, individuals needed at least one visit with a primary care provider (PCP) during the measurement year (or the previous year, depending on age). For preventive care, age-stratified groups were evaluated for well-child visits indicated by procedure or diagnosis codes with a PCP or obstetrician/gynecologist during the calendar year.
Over the study period, access to primary and preventative care improved for youth in foster care covered by MMC, unlike youth in the FFS control group.15 For foster youth aged 12 to 24 months, there was no significant change in access to primary care after transitioning to MMC.15 For youth aged 2 to 6 years, transitioning to MMC improved access to primary care by 12.18%, 13.01% for youth aged 7 to 11 years, and 8.68% for youth aged 12 to 18 years after adjusting for covariates.15 Similarly, preventive care access improved by 13.81% and 10.47% for youth aged 3 to 6 years and 12 to 18 years, respectively.15
Day, Curtis, Paul, et al. (2018)16 examined the timeliness of well-child visits for older foster care youth, 10 to 20 years old. Data was captured from November 1, 2009, to September 1, 2012, during which the state of Michigan transitioned its youth in care from FFS to Health Maintenance Organization (HMO) plans, a type of MMC. A retrospective analysis was conducted for 1,657 youth using child welfare administrative data in addition to Medicaid claims and encounter data.16 The timeliness of well-child visits was determined by analyzing the initial well-child visit recorded following entry into foster care, serving as the reference point. The duration between foster care entry and the first well-child visit was calculated, and visits occurring within 30 days of entry were considered timely. This study coincides with the introduction of policies designed to encourage timely Medicaid enrollment and well-child visits for youth newly entering care, with confounding factors addressed in the analysis. Day, Curtis, Paul, et al.'s article (2016) was rated as having a low risk of bias.
The percentage of timely visits increased during the managed care period, from 27.6% during the FFS period to 52.2% during the MC period.16 Additionally, the percentage of youth meeting the requirement to begin Medicaid within 14 days of foster care entry rose from 85.1% to 96.8% during the FFS and MMC (HMO) periods, respectively.16 The reported odds ratio for receiving timely well-child visits reveals that youth who entered care during the MMC (HMO) period were 2.46 times as likely as those who entered care during the FFS period.16
Notably, this analysis revealed that non-Hispanic black foster care youth and those with multiple housing arrangements had lower odds (0.65) of timely visits.16 Similarly, four (0.78) or more (0.62) housing placements and those not enrolled in Medicaid within 14 days of foster care entry (0.46) had lower odds of timely visits.16 Regarding the time taken for the first well-child visit, youth entering foster care during the managed care period experienced significantly fewer days to their first visit compared to those in the FFS or transition periods. Overall, the analysis indicated that the transition to managed care was associated with improved timeliness of well-child visits among foster care youth, with notable disparities observed based on demographic and enrollment factors.
Well-child visit utilization is rated with a low certainty of evidence, primarily due to the limited number of eligible articles, only two, and concerns about risk of bias. One study was found to have a high risk of bias across several domains, while the other was assessed with a low risk of bias. The small evidence base and methodological limitations together weaken the overall confidence in the findings.
Dental and vision careNo included articles assessed the impact of MMC on dental or vision care utilization or cost for foster youth.
Comments (0)