Tyrosine Kinase Inhibitors
The remarkable success of imatinib has catalyzed the development of next-generation TKIs designed to overcome mechanisms of resistance and to target the diverse array of other oncogenic kinase fusions found in HES and related neoplasms. This research has led to a growing collection of potent agents that offer new hope for patients with molecularly defined diseases who do not benefit from standard therapies.
A key area of development has been addressing imatinib resistance in PDGFRA-rearranged disease. While the T674I gatekeeper mutation is a known mechanism of resistance, mutations in the activation loop, such as D842V, also confer complete resistance to imatinib and other conventional TKIs [29]. Avapritinib is a highly potent, type I kinase inhibitor specifically designed to target and inhibit KIT and PDGFRA activation loop mutants [29]. Its efficacy was demonstrated in the pivotal NAVIGATOR trial in patients with gastrointestinal stromal tumors (GIST) harboring the PDGFRA D842V mutation, where it induced durable responses in the majority of patients, leading to its approval by the Food and Drug Administration (FDA) for this indication [30]. Although these mutations are rare in the context of myeloid neoplasms, studies have demonstrated the successful use of avapritinib in patients with PDGFRA-mutant systemic mastocytosis with eosinophilia and other myeloid neoplasms, establishing a mechanistic and clinical rationale for its use in select patients with imatinib-resistant PDGFRA-mutant neoplasms, recognizing that evidence in hypereosinophilic neoplasms remains limited [35].
For the notoriously aggressive and chemo-refractory FGFR1-rearranged neoplasms, several TKIs have been investigated. Ponatinib, a potent multi-targeted TKI with activity against ABL, PDGFR, FGFR, and VEGFR, was an early agent of interest [32]. Preclinical studies provided a strong rationale, demonstrating that ponatinib could effectively suppress the growth of cell lines driven by various FGFR1 fusion proteins and prolong survival in mouse models [36]. However, clinical experience has been mixed. While ponatinib can induce hematologic responses, and in some cases, complete remissions in patients with FGFR1-rearranged disease, these responses are often transient, and the drug carries a significant risk of serious vascular adverse events [37]. Its role is therefore limited, often serving as a potential bridge to HSCT in select patients [26, 37].
The challenges with ponatinib have highlighted the need for more specific and potent FGFR inhibitors. Pemigatinib is a selective inhibitor of FGFR1, 2, and 3 that was granted an FDA approval for treating cholangiocarcinoma with FGFR2 fusions [38]. Its activity against FGFR1 fusions has been demonstrated in myeloid/lymphoid neoplasms, most notably in the phase 2 FIGHT-203 study, where it induced high rates of complete response, leading to its recent approval for this specific indication [39]. In this pivotal trial, pemigatinib produced complete hematologic responses in nearly 80% of patients with chronic-phase disease and durable cytogenetic remissions, which directly supported its FDA approval in 2022 for myeloid/lymphoid neoplasms with FGFR1 rearrangement [39]. Long-term follow-up has demonstrated sustained efficacy, with many patients successfully bridged to HSCT [40]. This represents a major therapeutic advance, providing the first specifically approved targeted therapy for this high-risk patient population. Other investigational agents targeting the FGFR pathway, such as futibatinib and infigratinib, are also in various stages of clinical development, reflecting an active and promising area of research aimed at improving outcomes for these diseases [32]. Importantly, despite the marked activity of pemigatinib in FGFR1-rearranged neoplasms, allogeneic hematopoietic stem cell transplantation remains essential for durable disease control in patients presenting with accelerated-phase or blast-phase disease. In these settings, selective FGFR inhibition should be viewed primarily as a cytoreductive and disease-stabilizing strategy to achieve remission and optimize patients for timely transplantation, rather than as definitive therapy [22, 26, 40].
JAK Inhibitors
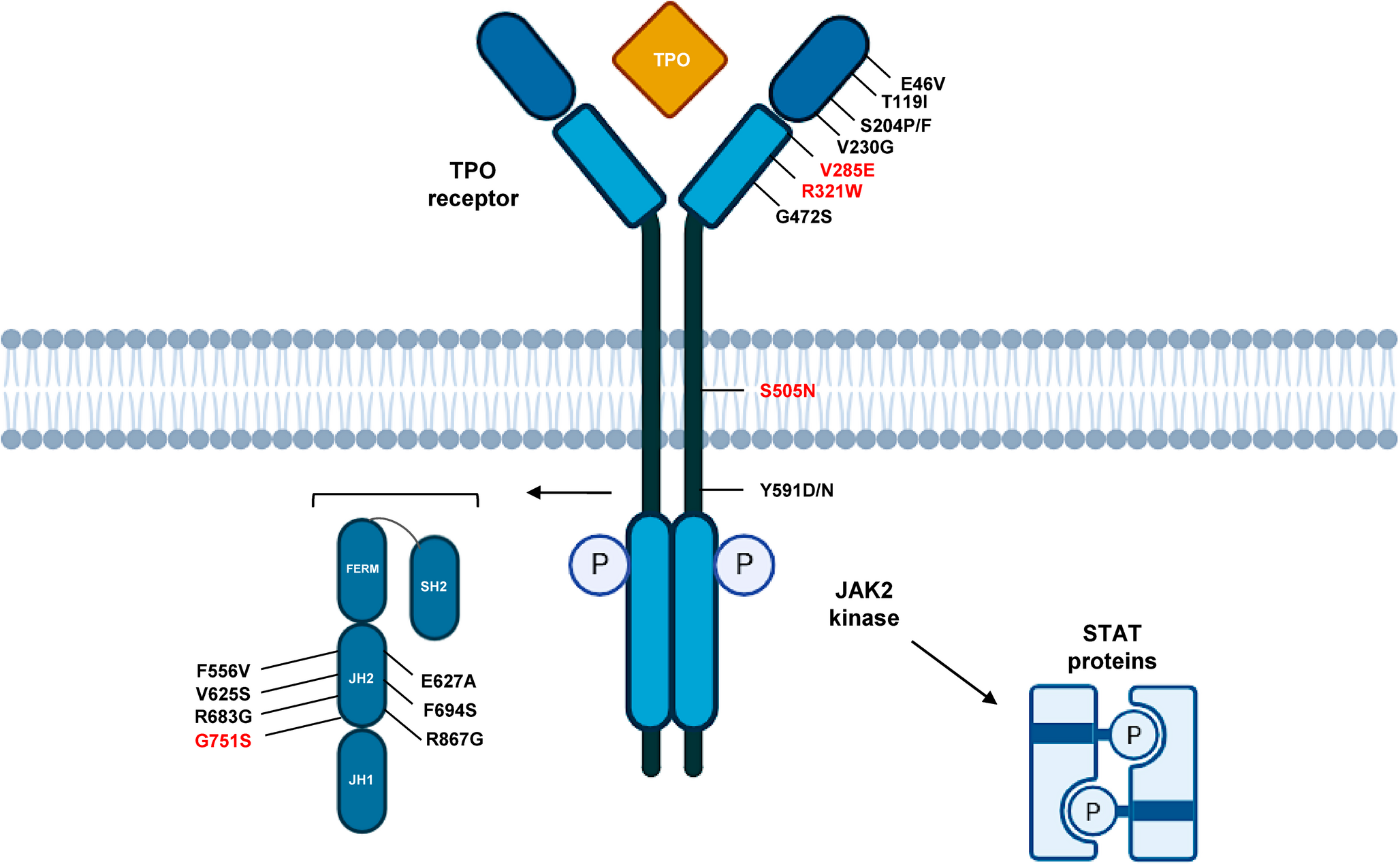
The Janus kinase (JAK)-signal transducer and activator of transcription (STAT) pathway is a critical signaling cascade for a multitude of cytokines and growth factors essential for hematopoiesis and immune regulation. Its aberrant activation is a central pathogenic mechanism in classical MPNs like myelofibrosis and polycythemia vera, making it a prime therapeutic target. This rationale extends logically to the subset of HES and related overlap neoplasms where dysregulation of this pathway is the primary oncogenic driver [12].
Ruxolitinib, a potent inhibitor of JAK1 and JAK2, has become a cornerstone of therapy for myelofibrosis and polycythemia vera, demonstrating significant efficacy in reducing splenomegaly and improving constitutional symptoms [41]. Its role in eosinophilic disorders is being actively explored, particularly in cases driven by specific JAK2 abnormalities. This includes the small subset of HES patients who harbor the canonical JAK2 V617F mutation, as well as those with the provisional WHO entity defined by JAK2 rearrangements, most commonly PCM1-JAK2 [8]. In these molecularly defined populations, ruxolitinib represents a direct targeted therapy. Available reports, primarily limited to small series and case-based studies, demonstrate that ruxolitinib can reduce eosinophil counts, alleviate disease-related symptoms such as pruritus and night sweats, and decrease spleen size in select patients with JAK2-mutated HES or PCM1-JAK2-positive neoplasms [42, 43]. These early signals of activity warrant further investigation in prospective clinical trials to better define its efficacy and safety in this specific patient population.
The therapeutic landscape of JAK inhibition has expanded beyond ruxolitinib with the approval of second-generation agents. Fedratinib, a selective JAK2 inhibitor, and momelotinib, an inhibitor of JAK1, JAK2, and ACVR1, are now established treatments for myelofibrosis, offering new options for patients who are intolerant to or have lost response to ruxolitinib [44, 45]. While clinical data for these newer agents specifically in HES are currently scarce, their proven efficacy in controlling the myeloproliferation and cytokine-driven symptoms of MPNs suggests they may have a future role in managing eosinophilic overlap syndromes, pending further investigation.
Monoclonal Antibodies and Immune Modulators
While TKIs target the intrinsic cellular drivers of myeloproliferation, a parallel and highly effective therapeutic strategy involves targeting the extrinsic factors that promote eosinophil survival and activation. Among them, the IL-5 signaling pathway is the most critical, acting as the master regulator of eosinophil differentiation, trafficking, and persistence. The development of monoclonal antibodies that disrupt this pathway has influenced the treatment of severe eosinophilic asthma and has now been successfully translated to the management of HES.
Mepolizumab, a humanized monoclonal antibody that binds to and neutralizes circulating IL-5, was the first biologic agent to be extensively studied in this setting. A pivotal randomized, double-blind, placebo-controlled trial demonstrated that mepolizumab significantly reduced the rate of disease flares and allowed for a substantial reduction in corticosteroid dosage in patients with FIP1L1-PDGFRA-negative HES [17]. These findings led to its approval by the FDA for this specific indication, providing the first approved targeted therapy for the non-clonal HES population. Although its primary indication is for non-myeloproliferative HES, mepolizumab is increasingly used off-label to manage severe, refractory eosinophilia in patients with myeloproliferative variants [13]. In this context, it can serve as a potent steroid-sparing agent or as a bridge to more definitive therapy, such as HSCT, by controlling the end-organ damage mediated by eosinophils [13].
Another highly effective agent is benralizumab, a monoclonal antibody that targets the IL-5 receptor alpha chain (IL-5Rα) expressed on the surface of eosinophils and basophils. Unlike mepolizumab, which sequesters IL-5, benralizumab induces direct, rapid, and near-complete depletion of eosinophils through antibody-dependent cell-mediated cytotoxicity. Studies, including a randomized phase 2 trial and real-world series, suggest that benralizumab can induce rapid, deep, and sustained eosinophil depletion in steroid-refractory HES [46], although evidence in clonal myeloid neoplasms remains limited and such agents do not directly eradicate the malignant clone. More recently, results from the phase 3 NATRON study demonstrated that benralizumab significantly delayed time to disease worsening or flare and improved clinical outcomes in patients with HES, with a favorable safety profile [47]. Its use in HES remains off-label (approved for asthma and eosinophilic granulomatosis with polyangiitis), although its potent cytolytic activity has made it an attractive option. Although case-based evidence includes patients treated after mepolizumab failure and occasional reports with clonal/myeloid features, data in overt myeloid neoplasms are limited and management should be individualized [13, 46].
Other immune pathways are also being explored. Dupilumab is a monoclonal antibody that blocks the alpha subunit of the IL-4 receptor, thereby inhibiting both IL-4 and IL-13 signaling. These cytokines are central to type 2 inflammation and contribute to eosinophil recruitment and activation. While its role in HES is less established than the anti-IL-5 agents, studies have shown its efficacy in controlling eosinophilia and clinical symptoms, suggesting it may be a viable option for select patients [48].
The role of checkpoint inhibitors, such as anti-PD-1 or anti-CTLA-4 antibodies, is purely investigational and must be approached with extreme caution. A well-recognized spectrum of immune-related adverse events is associated with these agents, including the development of significant eosinophilia [49]. Consequently, there is a strong theoretical concern that their use in a patient with an underlying eosinophilic neoplasm could trigger a dangerous “eosinophil flare,” potentially exacerbating the disease. Their use would only be contemplated in highly specific and rare clinical scenarios, such as transformation to a lymphoid blast phase where such therapies might be indicated, and only with careful risk-benefit analysis.
Epigenetic and Targeted Agents
Beyond targeting kinases and cytokine pathways, research is actively exploring other critical vulnerabilities in myeloid cancer cells, including epigenetic dysregulation and dependencies on specific metabolic and survival pathways. These approaches are particularly relevant for overlap MDS/MPN syndromes like aCML, which often lack a single, dominant kinase driver and are instead characterized by a more complex mutational landscape [16, 33].
Hypomethylating agents (HMAs), such as azacitidine and decitabine, are the cornerstone of therapy for higher-risk myelodysplastic syndromes (MDS). These drugs work by incorporating into DNA and inhibiting DNA methyltransferases, leading to global hypomethylation and the re-expression of silenced tumor suppressor genes. Given the significant clinical and molecular overlap between MDS and aCML, HMAs represent an important therapeutic option for these patients. While currently considered off-label and not standard of care for aCML, HMAs can provide transitory responses. They may serve a critical role as a bridge to HSCT for eligible patients requiring cytoreduction, or as an alternative therapy for transplant-ineligible patients who cannot tolerate standard agents like hydroxyurea [50].
The principle of precision medicine, focused on targeting a specific mutation with a tailored inhibitor, extends to this patient population. Although rare in HES and aCML, mutations in the isocitrate dehydrogenase genes, IDH1 and IDH2, can occur. Potent, specific inhibitors—ivosidenib (for IDH1) and enasidenib (for IDH2)—are approved for treating patients with IDH-mutant acute myeloid leukemia (AML) and have shown efficacy in other IDH-mutant myeloid neoplasms [51, 52]. For the rare HES or aCML patient found to harbor one of these mutations, these targeted agents represent a clear and compelling therapeutic option.
Furthermore, a strong biological rationale exists for targeting other crucial cell survival pathways. The anti-apoptotic protein BCL2 is frequently overexpressed in myeloid malignancies, conferring a survival advantage to leukemic cells. Venetoclax, a BCL2 inhibitor, has significantly impacted the treatment of older or unfit patients with AML, especially when used in combination with HMAs [53]. This highly effective combination is now being actively investigated in high-risk MDS and chronic myelomonocytic leukemia (CMML), with promising results [54]. This provides a strong rationale for exploring venetoclax-based combinations in refractory aCML, particularly in patients already being treated with an HMA. Similarly, preclinical evidence suggests that the Hedgehog signaling pathway, which is critical for leukemic stem cell maintenance, may be a viable target. Glasdegib, a Hedgehog pathway inhibitor, is approved in combination with low-dose cytarabine for newly diagnosed AML in older adults, and its role in other myeloid neoplasms remains an area of active investigation [55].

Comments (0)