This study investigated the interplay between nocturnal CBT, HR, and sleep architecture by statistically comparing two cohorts of healthy adult males of differing ages: a younger group (mean age 26.5 years; study 1) and a middle-aged group (mean age 46.2 years; study 2). Our findings confirm and extend previous research, highlighting distinct age-related patterns in nocturnal CBT and sleep stage distribution.
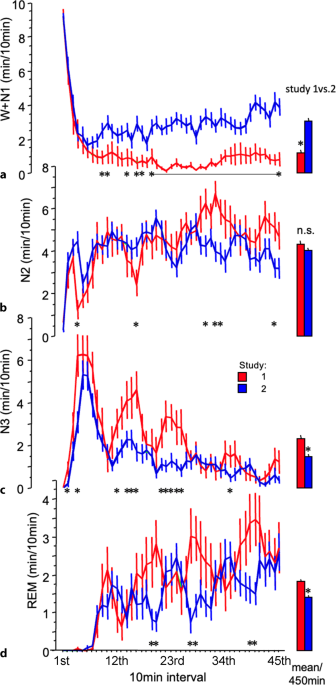
The primary observation was a significant difference in sleep consolidation and nocturnal CBT profiles between the two age groups. Study 1 exhibited objectively more sleep (increased sleep efficiency), characterized by TST, a higher proportion of slow-wave (N3) and REM sleep, and shorter sleep onset latency (SOL) and wake after sleep onset (WASO) compared to study 2. Sleep stage 2 (N2) did not differ between the groups. This aligns with established literature indicating a general decline in sleep consolidation and alterations in sleep architecture with advancing age, particularly a reduction in N3 sleep [13, 17, 18].
The nocturnal CBT trajectories also differed markedly. In study 1, CBT showed a sustained decline for approximately 5 h after sleep onset, remaining low thereafter. Conversely, in study 2, CBT was lower at sleep onset and declined over the initial 2 h, but it then began a gradual ascent for the remainder of the night. This pattern in the middle-aged group—an earlier nadir and a subsequent rise—is consistent with reports of age-related changes in circadian rhythmicity, including a tendency towards phase advancement and a potential reduction in the amplitude of the CBT rhythm [13, 15]. It has been specifically noted that while baseline CBT might not differ significantly in healthy aging, the dynamics of its nocturnal fall and rise can be altered [15]. Already nearly 100 years ago, Kleitman and Doctorsky (1933) stated that going to bed at night when the muscle tonus is low leads to a further decrease in tonus, as indicated by the low CBT [19]. It is therefore quite possible that the decline in CBT after lying down and falling asleep [20] differs between the two age groups, likely due to the well-documented aging process of the cardiovascular system [21].
The early upswing in CBT and HR after the initial drop after lights out in older adults may reflect age-related changes in the autonomic, vascular, and thermoregulatory systems that reduce the efficiency of the physiological “shutdown” that aids sleep consolidation. In younger adults, parasympathetic activation lowers HR and CBT after lights out, while in older adults, sympathetic dominance and weaker parasympathetic activation prevent a persistent drop, limiting the cardiovascular shift needed for restful sleep. Additionally, the decline in CBT is hindered by less efficient heat transfer from the core to the environment due to impaired blood flow redistribution.
Interplay between age, core body temperature, heart rate, and sleep stage distribution
A central question arising from these observations concerns the nature of the relationship between CBT, HR, and sleep stage distribution, particularly in the context of aging. Is the observed difference in sleep primarily a consequence of age-related changes in the circadian pacemaker, or does CBT itself directly modulate sleep structure—independently of or in addition to circadian influences? Our comparative study cannot provide conclusive evidence in this regard; however, it can at least highlight plausible associations in line with the existing literature that could be examined in prospective studies. Historically, research has pointed towards a change in the circadian pacemaker system with age, including a diminished circadian amplitude, e.g., as measured by CBT rhythm [17]. This could inherently lead to a shallower nocturnal CBT dip and poorer sleep consolidation. However, it is also noted that older individuals typically exhibit an earlier-timed circadian phase [13]. Thus, simply attributing the observed sleep differences solely to age as a global factor affecting circadian output is an oversimplification. Our findings, when viewed alongside evidence from temperature intervention studies [3,4,5, 7, 8], suggest a more direct role of CBT in modulating sleep. The original studies from which our current data are derived demonstrated that using a high-heat-capacity mattress to enhance conductive heat loss and lower CBT led to significant increases in N3 sleep and a reduction in HR in both young and middle-aged men [3, 5]. Quantitative sleep measures (Table 1) further support this, showing higher percentages of N3 on the cooling mattress in both study 1 and study 2 [3, 5] and demonstrating a higher percentage of the night spent in deep sleep (N3%). This suggests that actively lowering CBT can improve deep sleep irrespective of the baseline age-related circadian characteristics. This aligns with work proposing that a failure of CBT downregulation at sleep onset could lead to SWS deficiency in insomnia [1, 12] and with studies discussing hyperarousal and elevated CBT [2, 11] and HR [22] in insomnia. The capacity of a cooling mattress to facilitate a more pronounced drop in CBT, as seen in the original intervention studies, appears to directly translate into enhanced N3 sleep—a stage crucial for restorative processes [3,4,5]. Therefore, while age-related changes in circadian timing and amplitude undoubtedly contribute to the differing sleep and CBT profiles observed in our cohorts, the direct physiological link between a lower CBT and improved N3 sleep and calmer HR seems to be an independent and significant factor. The mechanisms likely involve the intricate connections between thermoregulatory centres in the hypothalamus and sleep-regulating nuclei, where a cooler core temperature may facilitate the neuronal processes underlying N3 sleep generation and reduce sympathetic tone [6, 23,24,25].
Limitations
This study combines data from two independent cohorts, which, while matched for health status, inherently introduces variability. The age groups are distinct, but a continuous age spectrum was not assessed. Our analysis and focus on the age of the two groups is rather observational and limited to hypothesis generation; we cannot prove that age is the sole responsible variable, even though prior literature supports the idea. Studies were conducted in two different university sleep laboratories (Turin, Italy, and Berlin, Germany). Although identical protocols and lab conditions were used—including standardized temperature measurements—regional factors may still have introduced variability. These could include environmental or climatic differences or variations in inter-rater reliability of sleep scoring. The interpretation of causality between CBT and sleep, while supported by intervention literature, remains complex in an observational comparison between age groups where multiple physiological systems are changing concurrently. Various physiological changes associated with the onset of sleep appear to complement one another. For instance, simply lying down—even without falling asleep—can lead to decreases in CBT and HR, effects similar to those observed during the transition into sleep following lights out [20, 26]. However, to conclusively disentangle and clarify these effects—particularly in relation to the aging process—longitudinal intra-individual studies are required. Additionally, the relationship between sleep latency and thermoregulatory changes cannot be conclusively examined across the studies, as the necessary values prior to lights out are not available. In the present study, only men were examined (whereas a third study included only women [4]). To make well-founded and generalizable statements, studies involving mixed-gender groups with different ages are needed.
Implications and future directions
An interesting observation was the difference in non-REM (NREM) and REM sleep cycles. In our samples, younger men showed distinct REM and NREM sleep cycles, while middle-aged men also had less defined peaks. This difference, while purely observational in the current comparative analysis, might hint at subtle age-related alterations in the timing mechanisms governing NREM–REM cycling and its interaction with the circadian rhythm, which could be an avenue for more focused investigation in the future. Within this context, a previous study has shown that so-called quality sleep—comprising N3 and REM sleep—is most strongly associated with the age-related increase in overnight metabolic rate [27], which aligns well with our results.
The confirmation of distinct nocturnal CBT and HR profiles associated with differing sleep stage distribution across age groups reinforces the importance of thermoregulation in sleep health. However, unlike in smaller animals such as mice [6, 24], there is no clear temporal association between the NREM–REM sleep cycle and CBT in humans [16]. Our findings instead support the speculation that younger men, compared to their middle-aged counterparts, experience an enhanced nocturnal N3 sleep stage, potentially through increased sleep cycle amplitude. This appears to be accompanied—if not partly caused—by slower but more pronounced nocturnal declines in HR and CBT, as observed in study 1. Notably, evidence that direct modulation of CBT, e.g., via cooling mattresses, can enhance N3 sleep and lower HR is particularly relevant. This was demonstrated in our studies using a cooling high-heat-capacity mattress [3,4,5] and is further supported by findings from other investigations using different cooling methods [7, 8]. The potential effect of cooling mattresses on blood pressure is currently under investigation.
Implications of climate for sleep consolidation
A brief but pertinent consideration is the context of global climate change. Rising ambient temperatures and more frequent heatwaves are increasingly recognized as being detrimental to sleep [28]. Understanding the physiological impact of thermal stress on sleep and the potential for interventions that promote nocturnal heat loss, such as cooling mattresses or other environmental modifications, is becoming increasingly crucial. Future research could explore the efficacy of such interventions in mitigating the negative effects of heat exposure on sleep, especially in vulnerable populations such as the elderly. Further research should also continue to disentangle the direct effects of CBT on sleep from the broader age-related changes in circadian regulation. Longitudinal studies tracking individuals over decades would be invaluable in this regard. Additionally, exploring the nuanced differences in NREM–REM sleep periodicity and their physiological underpinnings could offer new insights into age-related sleep changes. Future studies must also show that not only the ambient air temperature is important, but also the dissipation of body heat via conduction, e.g., into the mattress.


Comments (0)