To the best of our knowledge, this is the first study reporting the prognostic significance of mEPE score in patients diagnosed with intermediate-risk prostate cancer treated with robotic ultrahypofractionated SBRT without ADT. Our findings suggest that a higher mEPE score is associated with lower BFS.
Multiple studies have demonstrated the feasibility and efficacy of ultrahypofractionated SBRT for localized low- and intermediate-risk prostate cancer, showing long-term BFS rates ranging from 85 to 100% [10, 19,20,21]. Hereby, treatment choices, including decisions on the delivered radiation dose and target volumes, are influenced by whether or not the disease is confined to the organ [2, 22]. Therefore, accurate pretherapeutic imaging is crucial, and mpMRI has been shown to have a significant impact on staging when performed additionally to conventional diagnostics [4, 23]. However, in a meta-analysis by de Rooij et al., MRI-based detection of the extraprostatic extension appears to have limited and heterogeneous sensitivity (SE: 0.61, 95% CI 0.54–0.67) [6]. This may impose a challenge, as SBRT for high-risk prostate cancer remains underinvestigated and is not routinely advised [15, 24]. Moreover, intensified systemic treatment in high-risk prostate cancer patients undergoing radiotherapy is part of the multimodal treatment concept [2].
For patients undergoing prostatectomy, the mEPE score is of relevance, as higher scores are associated with an increased risk of positive postoperative margins and biochemical recurrence [7, 8]. To improve the prediction of side-specific EPE, Soeterik et al. developed a comprehensive nomogram. This model incorporated digital rectal examination staging, the highest ipsilateral International Society of Urological Pathology biopsy grade, and PSA density, in addition to an MRI-based score, achieving a remarkable area under the curve of approximately 0.8 [25]. The additional diagnostic value of combining clinical nomograms with MRI-based models was validated by a systematic review conducted by Zhu et al., which analyzed multiple nomograms for predicting EPE. The combined nomograms may enhance decision-making protocols for prostate cancer patients in the pretreatment phase [26]. Nevertheless, there is no evidence for the impact of mEPE score on the outcome of patients diagnosed with intermediate-risk prostate cancer treated with ultrahypofractionated SBRT.
In this analysis, a higher mEPE score was correlated with lower BFS. A possible explanation is that among patients with higher mEPE scores, some may be understaged and present with EPE, as patients with higher mEPE scores are more likely to exhibit pathological EPE [5]. Consequently, some of these lesions could have belonged to the group of high-risk prostate cancer with T3 stage [17]. This aligns with the findings of Ma et al., who reported understaging of T3 prostate cancer in pretherapeutic MRI compared to pathological findings in 44% of patients undergoing radical prostatectomy [27]. Correspondingly, BFS in our cohort, with 92 and 75% after 3 years and 4 years, respectively, is considerably lower than then BFS stated in the PACE B trial [28]. Hereby, van As et al. reported a 5-year BFS of 95.8% for patients with localized prostate cancer treated with SBRT [28]. This BFS difference could be due to several factors: a total of 7.5% of the patients treated with SBRT in the PACE B trial were diagnosed with low-risk prostate cancer. Furthermore, no patients with Gleason 7b were included [28]. In contrast, low-risk prostate cancer patients were excluded from our analysis, and we included patients with Gleason 7b, accounting for 18.9% of our cohort. These factors have been associated with lower BFS, as stated in an analysis of 477 prostate cancer patients treated with SBRT by Katz et al. [29]. Hereby, BFS of patients with Gleason 7b was comparable to BFS in our cohort [29]. Moreover, 66.2% of our patients were treated with a total radiation dose of 35 Gy, which is lower than the 36.25 Gy total dose applied in the PACE B trial [28]. This may contribute to inferior BFS in our cohort, as dose escalation from 35 to 37.25 Gy in SBRT for low- and intermediate-risk prostate cancer was associated with improved BFS in a prospective trial by Moore et al. Failure rates at 8 years post-treatment were 15% for the 35 Gy dose and 3.4% for the 37.25 Gy dose [10]. Aligning with these findings, a significant BFS difference was observed in our cohort, favoring the total radiation dose of 36.35 Gy over 35 Gy (p = 0.04). Additionally, the BFS rates of our cohort patients with high mEPE scores are comparable to the BFS rates of high-risk prostate cancer patients treated with ultrahypofractionated SBRT only published by the SHARP consortium [15]. Therefore, considering the lower BFS and the risk of EPE, a higher mEPE score might be considered an additional risk factor in prostate cancer. Therefore, treatment intensification for this patient subgroup should be considered.
Several approaches for treatment intensification in localized prostate cancer focus on escalating the dose to the visible tumor identified on MRI, as local recurrences typically originate from these areas [30,31,32,33]. In the Focal Lesion Ablative Microboost in Prostate Cancer (FLAME) randomized phase III trial by Kerkmeijer et al., patients received up to 77 Gy to the prostate, with an experimental arm receiving an additional simultaneous integrated focal boost to the intraprostatic lesion visible on MRI with up to 95 Gy [31]. Results showed a BFS difference favoring the experimental arm (hazard ratio 0.45, 95% CI 0.28 to 0.71; p < 0.001), with no significant difference in acute or late genitourinary and gastrointestinal toxicity [31]. However, the 7% difference in BFS at 5‑year follow-up may also result from the higher rate of patients receiving long-term androgen deprivation therapy (ADT) in the experimental arm (experimental arm 34% vs. standard arm 29%) [34]. Furthermore, Hannan et al. investigated dose escalation in SBRT to the whole prostate with up to 45 to 50 Gy and showed excellent local control with increased severe late toxicities [35]. Accordingly, studies on dose escalation in conventional radiotherapy for intermediate-risk prostate cancer also suggest that dose escalation might have a beneficial impact on BFS and metastases-free survival, with equivalent or slightly elevated toxicities [4]. However, due to limited follow-up, an overall survival benefit through dose intensification remains investigational [4].
In accordance with the above, treatment intensification by adding short-term ADT to SBRT for intermediate-risk cancer patients also yields a BFS benefit but, for the subgroup of patients with unfavorable intermediate-risk prostate cancer, an overall survival (OS) benefit can be obtained [4, 33, 36].
Since none of the patients in this cohort received ADT, and a high mEPE score may indicate a risk of EPE in some cases, treating these patients exclusively with ultrahypofractionated SBRT could lead to undertreatment. It may be reasonable to consider escalating systemic treatment to long-term ADT, since EPE is a high-risk factor and large randomized prospective studies have reported superior OS with long-term ADT over short-term ADT in locally advanced prostate cancer patients [37, 38]. A randomized, prospective trial by Nabid et al. compared OS rates in high-risk prostate cancer patients receiving ADT for 18 months to those receiving ADT for 36 months, with no significant difference in OS found [39]. Therefore, at least 18 months of ADT could be a valid option for such patients.
Another approach could be to switch to a longer fractionation scheme in patients with a high mEPE score, as ultrahypofractionated SBRT for T3 stage prostate cancer is a topic of current debate [15]. Given the increased risk of seminal vesicle invasion in prostate cancer with T3a stage, compared to the T1 or T2 stages, the CTV may be expanded to include portions of the seminal vesicles for patients with a high mEPE score [40, 41]. This approach aligns with the recommendations outlined in the European Society for Radiotherapy and Oncology-Advisory Committee for Radiation Oncology Practice (ESTRO/ACROP) guidelines for the delineation of localized high-risk prostate cancer [40]. However, the proposed treatment intensifications for patients with a high mEPE score but who are classified as intermediate-risk prostate cancer could lead to overtreatment. Therefore, prospective studies are needed to validate these approaches.
According to our institutional policy, we discuss the benefit as well as possible side effects of short-term ADT with each patient. We particularly recommend additional systemic treatment for patients with unfavorable intermediate-risk prostate cancer undergoing ultrahypofractionated radiotherapy. Nevertheless, in cases where patients decline systemic treatment due to potential side effects, such as decreased libido and sexual dysfunction, hot flashes, and fatigue, ADT is omitted, as previously described in similar patient cohorts [28, 29, 42, 43]. However, given the lower BFS rates, we nowadays emphasize the importance of ADT according to established guidelines, especially for unfavorable intermediate-risk prostate cancer patients [2].
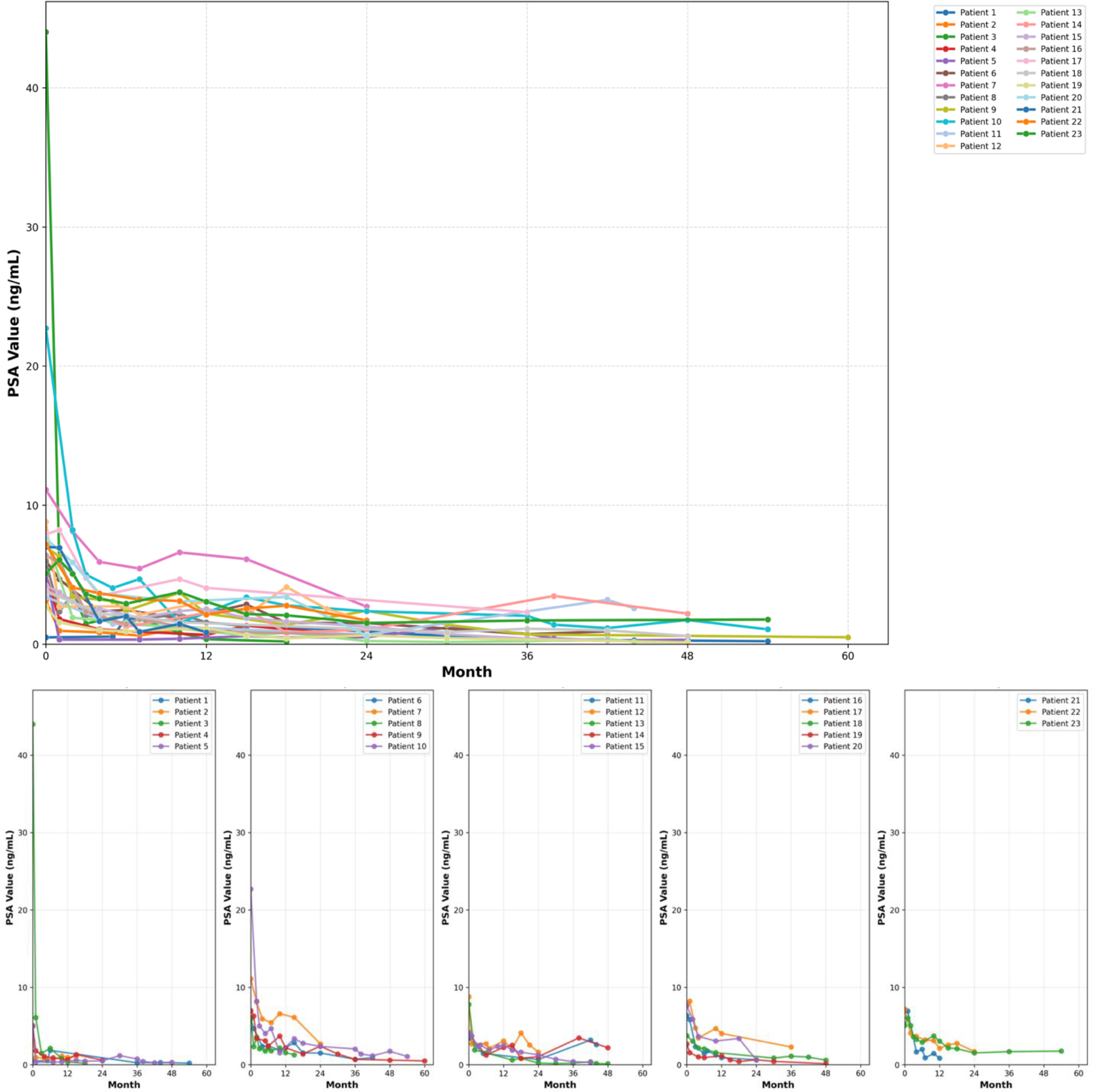
In our cohort, the PSA kinetics remain in alignment with the analysis of Jiang et al. [44]. A higher level of the PSA nadir was a significant predictor for biochemical failure in both studies [44]. However, the PSA nadir reported in our cohort is higher than in comparable cohorts [44]. A potential factor contributing to the elevated PSA nadir in our cohort may be the lower radiation dose, as a reduced radiation dose was associated with elevated PSA nadir levels [45]. Moreover, the multi-institutional analysis by Jiang et al. reported a median time to PSA nadir of 40 months. In contrast, our median follow-up was 30 months, suggesting that a significant proportion of patients may not have reached their PSA nadir during the observation period [44]. Moreover, a PSA bounce was noted in 20% of patients, which corresponds with previous literature on PSA bounce after SBRT, reported to range between 17 and 31% [29, 44, 46,47,48].
In contrast to other studies that reported a divergence between BFS and clinical failure-free survival, we observed a clinical manifestation for every biochemical failure [35, 49, 50]. This difference may be due to our use of PSMA-PET/CT for recurrence diagnosis, which yields superior detection rates for recurrences. Other studies did not report using PSMA-PET/CT [35, 49,50,51,52]. Although intraprostatic recurrences predominantly occur in the region of the primary tumor, we observed only two such lesions in that area, which may be attributed to the small number of intraprostatic recurrences [32].
Emerging techniques, such as radiomics models, hold the potential for identifying high-risk lesions within tumors as well as for detecting EPE in prostate cancer patients [53, 54]. In a recent systematic review by Ponsiglione et al., the pooled area under the curve for radiomics-based EPE diagnosis in prostate cancer patients was reported to be 0.8. However, the review highlighted significant heterogeneity among the studies (84.7%; p < 0.001) and addressed the lack of independent validation [53]. Moreover, radiomics techniques face multiple challenges, including the standardization of scanner parameters, post-processing algorithms, and applications across institutions. Due to the potential impact on the results, these challenges must be addressed before implementation in clinical practice [53, 54]. Additionally, unlike MRI diagnostics, radiomics models involve poorly explained parameters, while MRI provides the advantage of comparable applicability across institutions [53].
Nevertheless, there are limitations to our results, as the sample size is small, and the analysis is retrospective. Data were collected from one institution only, which may lead to sampling bias, and the follow-up only encompasses a median of 30 months. Additionally, it could be argued that prior biopsy and fiducial marker implantation introduced uncertainties into the MRI reading, as each intervention requires penetration of the capsule tissue. This may influence factors assessed in the mEPE score, such as the irregularity of capsule margins. Therefore, validation of our results in larger cohorts with longer follow-up periods is still needed.


Comments (0)