Questionnaires
Three questionnaires were used in this study: one questionnaire (KI-21) concerning patients’ perception of safety and concerns towards the upcoming discharge was developed in the prestudy and two questionnaires were compiled with items from the European Organization for Research and Treatment of Cancer (EORTC) database [20]. In addition, data on the type of cancer, treatment, and secondary diagnoses were collected from the patient file.
Prestudy
In preparation for the prestudy in summer 2021 (ethics application D537/21), as a first step, a literature search was conducted (PubMed; “home visits”, “radiotherapy”, “radiooncology” “discharge”). Issue lists were developed. The questionnaire items were developed using an inductive, expert-based approach. Semi-structured interviews with open-ended questions were conducted with two radiation oncologists, one psychologist, and one social worker. A medical doctoral candidate and a psychologist conducted the interviews. Key points from the interviews were documented in written format and used to develop a first draft of the questionnaire items.
Subsequently, the preliminary questionnaire was sent to all experts for feedback and suggestions for revisions. This feedback was then incorporated into the final version of the questionnaire (final version of this questionnaire in the supplement). The development process followed established recommendations for inductive item generation and expert review in questionnaire development [21]. First, patients were asked whether they would like to participate in the prestudy and answer the questionnaire. After giving their consent, they were given the questionnaire and, if necessary, it was read aloud to them. Three areas were mentioned as possible causes for concern among patients: practical everyday tasks (e.g., cooking, cleaning, and making appointments with their practitioner), the absence or presence of a contact person, and physical complaints (e.g., pain, nausea/vomiting, weakness), persistence of complaints, or worsening of symptoms. As a next step, questions asking inpatients about possible fears and concerns regarding their discharge were formulated. Furthermore, respondents were asked about the availability of private and professional support options. Patients were also given the opportunity to add their own comments and concerns. In addition, willingness to participate in a home visit by students was queried.
During the 4‑week prestudy period, all patients were interviewed prior to their upcoming discharge.
KI-21
The KI-21 questionnaire was developed from the prestudy questionnaire and adapted based on feedback from participating patients. For the final version of the questionnaire, feedback was again sought from the expert group that developed the prestudy questionnaire. The final KI-21 (full questionnaire in the supplement) contained questions about sociodemographic data (gender, age, last profession) and living situation (living alone or with a partner/family, assisted living, or other). Patients were also asked whether they had to climb stairs in their home environment and what medical services were available to support them. Three questions addressed the patients’ perception of safety on a numeric rating scale from 10 = very safe to 0 = very unsafe with regard to discharge, care, and medical help in the home environment and further treatment planning. The last item asked whether the patient had any further concerns about discharge and if so, what they were. There were nine different options to choose from, several of which could be ticked, and a field where the patients could express individual worries.
EORTC IL-174 and IL-175
In the EORTC IL-174, medical doctors were rated in four areas: human qualities (e.g., empathy, willingness to listen, politeness, respect, and friendliness), time, thoroughness of physical examinations, and provision of information. In six items the organization of care was evaluated (e.g., information on planned examination dates, and support offers). One last item concerned the overall care in this clinic. For all items, a 5-point scale was provided (1 = poor, 2 = fair, 3 = good, 4 = very good, 5 = excellent). The second EORTC questionnaire (IL-175) contained questions about the patients’ current health. On a numeric rating scale from 1 = not at all to 4 = very much, the patients rated symptoms and problems of pain, weakness, tension, helplessness, and frustration. On the same scale, they also indicated how much their physical condition or medical treatment affected their socializing or activities with other people. In two final questions, patients were asked to rate their state of health and quality of life on a numeric rating scale from 1 = very poor to 7 = excellent.
Study design and process
Based on the inclusion and exclusion criteria (Table 1) and the temporal feasibility of home visits, suitable patients were addressed: due to scheduling reasons, patients could only be included in the study by the students at selected times. The study included 60 participants, evenly divided between the two groups: with home visit and without home visit. Two to five days before discharge, patients were introduced to the project. After giving informed consent, patients were randomly assigned to a group. At each time point, the patients completed the same set of questionnaires: the KI-21, IL-174, and IL-175.
Table 1 Inclusion and exclusion criteria of potential study participants on the radiotherapy ward for possible inclusion in the pilot study with home visits by medical studentsIn the home visit group, patients had their first appointment with the students before discharge and completed the first set of questionnaires (A1). The medical students were prepared for the home visit through special and individualized training. During preparatory seminars, students learned about the support system for palliative patients in Germany. They also learned about the side effects of radiation therapy and how they are treated. Before the students met their assigned patients, a radiotherapy specialist explained the underlying oncological disease as well as relevant comorbidities and the treatment plan in advance. The typical course of disease and symptoms after discharge were discussed, which were to be monitored during the home visit. After discharge, the patients were visited by the students at home. The timing of the home visit was agreed upon jointly by the patient and the students (the specified period was 2–5 days after discharge). During the home visit, the patients were asked about their general condition based on a checklist and basic vital parameters were measured (see checklist in supplemental information). The patients completed the second set of questionnaires (A2) and could address any concerns or unanswered questions. For follow-up, the students met with one of the senior physicians, discussed the patients, and clarified questions. The home visits had no set duration. On average, a visit lasted about an hour. There were also no restrictions on whether or which relatives were allowed to attend the home visit. The students did not take on any organizational tasks, as patient follow-up care had already been arranged in advance.
The other group, without a home visit, completed the first set of questionnaires (B1) after giving consent and before being discharged. Two to five days after discharge, patients were contacted by telephone and completed the second set of questionnaires (B2).
Both groups completed the questionnaires by having the questions read aloud to them. They also had access to the questionnaires and were able to read the questions for themselves. The control group answered the second set of questionnaires by telephone.
Targeted advertising in specific social media groups and flyers distributed during lectures to the target group drew attention to the extracurricular teaching project. Interested students from the 5th year onwards were able to register and take part in an introductory information event. Inclusion criteria were successful completion of the first state medical examination and willingness to participate in the project.
Sample size calculation
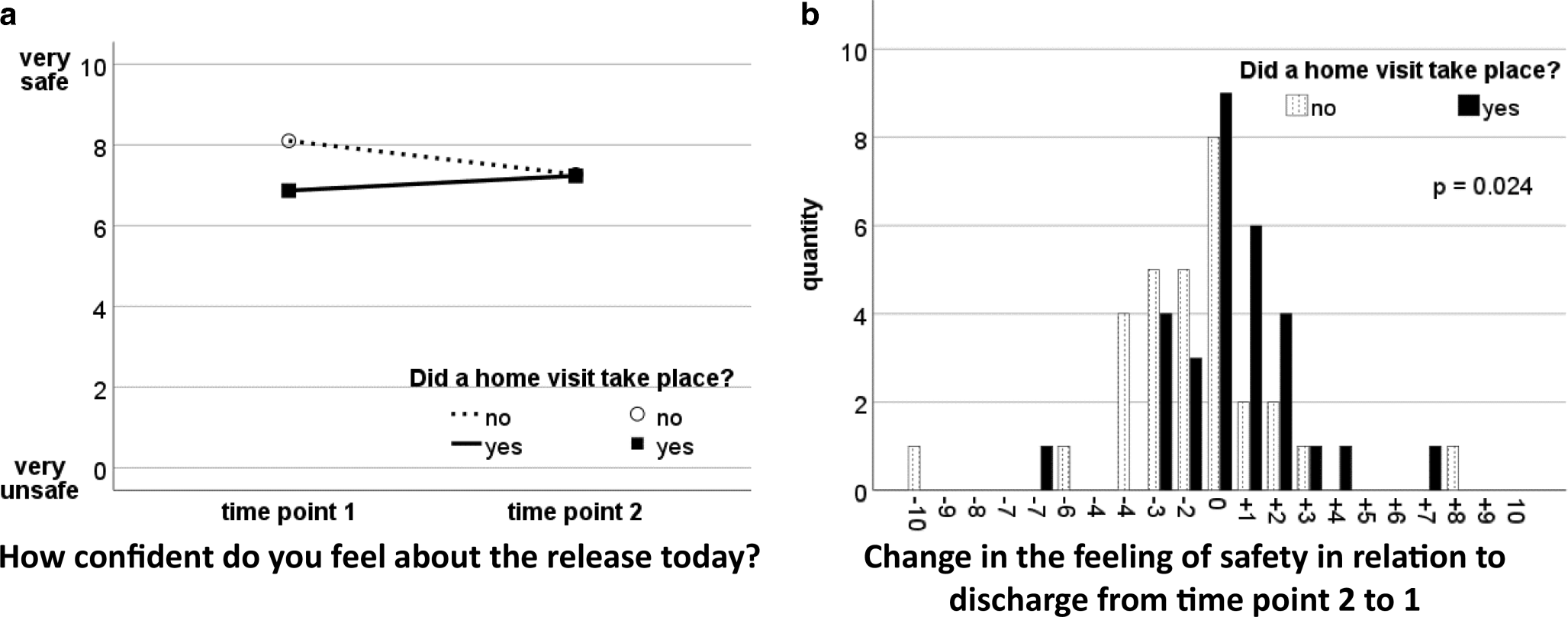
This study was a pilot study (ethics application D435/22). Therefore, the sample size calculation was geared towards a large effect. The primary outcome measure was the difference in inpatients’ perception of safety regarding the upcoming discharge between time points 1 and 2. Perception of safety was measured on an ordinal scale between 0 and 10 in the questionnaire. A nonparametric Wilcoxon rank sum test was used to compare the groups with and without a home visit. A large effect can be represented by Cohen’s d of 0.8, which corresponds to a Mann–Whitney estimator P(X < Y) of 0.7142 for the Wilcoxon rank sum test. For a significance level of 0.05 and a power of 0.80, this resulted in case numbers of n = 29 for the groups with and without home visits. The number of cases was calculated using the software program Bias for Windows, version 11.12 (https://www.bias-online.de).
Based on inclusion and exclusion criteria (Table 1), patients were recruited from April 2022 to February 2024.
Statistical analysis
First, the differences between time point 1 and 2 were calculated:
A::
Home visit group
B::
Control group
1::
time point 1 (before discharge)
2::
time point 2 (after discharge)
Subsequently, the two groups were compared based on their differences (X1 and X2) using the Mann–Whitney U test for independent samples with a significance level of 5%. Moreover, 95% confidence levels were computed. This test was applied to all items and merged item groups in the questionnaires.
Fisher’s exact test was used to analyze any differences between categorical variables in the cohorts at time point 1.
Statistics were calculated with the program IBM SPSS Statistics version 29.0.0 (Armonk, NY, USA).


Comments (0)