Our study provided a comprehensive description of the epidemiology of severe pulmonary infections in children in central China. The six years of data in this study, including three years of the COVID-19 pandemic, showed that the age of onset and the distribution of pathogens in severe pulmonary infections vary from year to year. Our study provides a reference for rapid diagnosis of pathogens and early targeted anti-infection treatments. In addition, this study may provide a reference for pathogen changes during similar subsequent public health events.
Unlike other epidemiological studies, our study used BALF culture results for data analysis [2, 5, 6]. BALF is collected directly from lung lesions via bronchoscopy, and the detection rate of pathogens is higher in BALF than in sputum or blood [14]. Therefore, BALF culture is regarded as the gold standard for diagnosing pathogens in severe pulmonary infections and has been widely used for an extended period [15,16,17,18]. These findings indicate that BALF cultures can provide a reliable diagnostic basis in clinical practice.
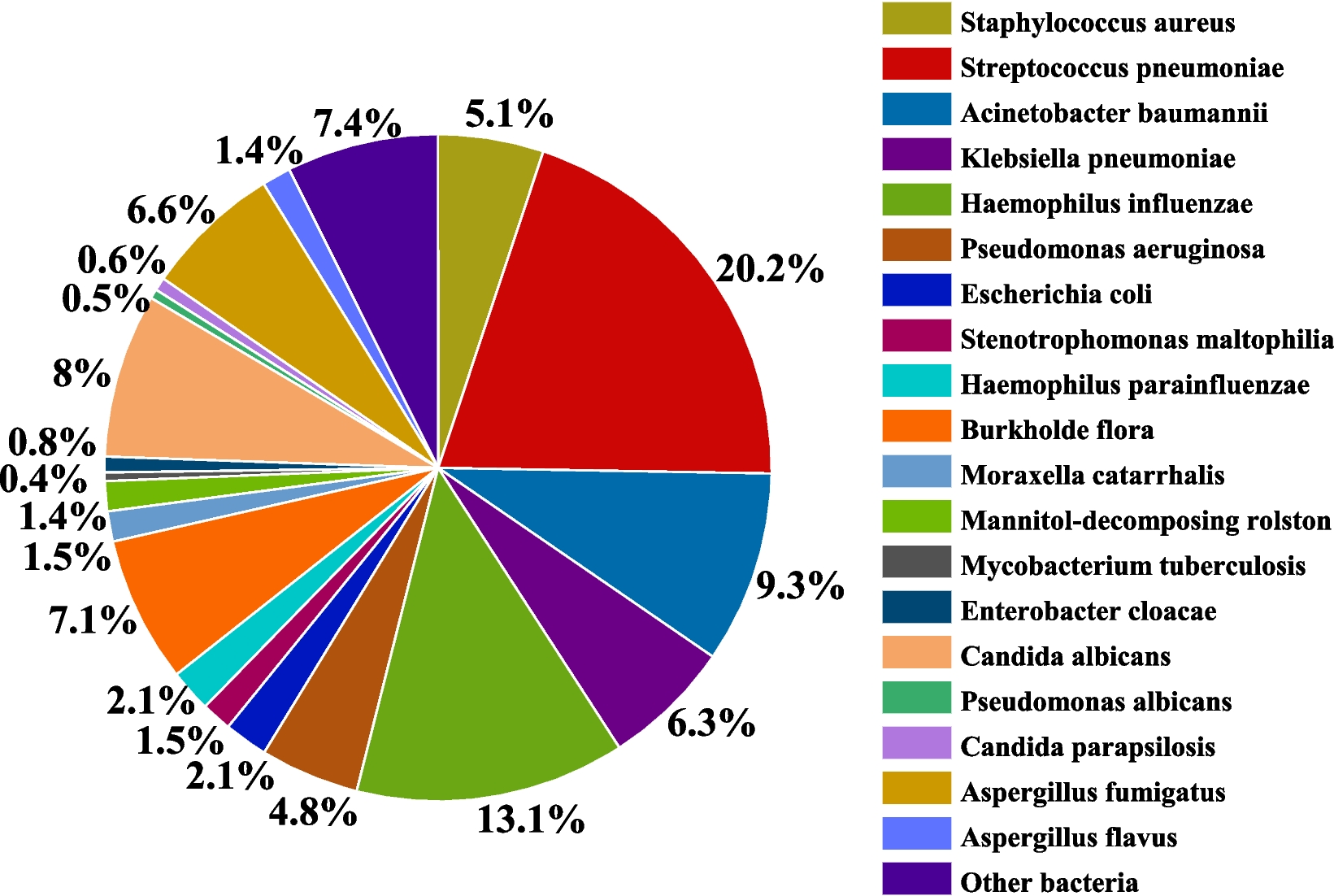
Our study indicated that the positive rate of BALF culture in children with severe pulmonary infections at our hospital was notably high, with gram-negative bacteria identified as the predominant pathogens. This was similar to the results of a previous study conducted in China [18]. The principal gram-negative bacteria identified were Haemophilus influenzae and Acinetobacter baumannii. The main gram-positive cocci included Streptococcus pneumoniae and Staphylococcus aureus. The primary fungi detected in this study were Candida albicans and Aspergillus fumigatus. However, in a study in the USA, children with community-acquired pneumonia who required hospitalization were more likely to be infected with the virus or mycoplasma [19]. This may be due to the widespread use of conjugate vaccines against Streptococcus pneumoniae and Haemophilus influenzae type b [20, 21]. Antibiotics are widely used in China; however, the coverage rate of conjugate vaccines remains low [22]. Studies have suggested that increasing the coverage rate of conjugate vaccines can lead to a reduction in the colonization rate of pathogens in the upper respiratory tract and decrease in antibiotic resistance rates, which have good health benefits [22, 23]. Vaccination against bacterial pathogens, such as Streptococcus pneumoniae and Haemophilus influenzae type b, represents an effective strategy to reduce both morbidity and mortality associated with severe pulmonary infections in children [24].
Our study revealed that the proportion of children with severe pulmonary infections was higher in males than in females. In addition, there has been an annual increase in the age of children with severe pulmonary infections. Notably, the incidence of positive BALF cultures in infants aged 0 to 12 months showed a decreasing trend over the years, whereas the incidence in children aged > 3 years showed an increasing trend. In infants aged 0 to 12 months, gram-negative bacilli were the predominant pathogens associated with severe pulmonary infections. Conversely, in children over 1 year of age, the infection rates of gram-positive cocci, Aspergillus fumigatus, and Candida albicans were relatively high. The results may be related to the impact of the COVID-19 pandemic on pathogens since 2020 [25]. For example, in Li’ s study, the number and positivity rate of pathogens in the blood of neonates decreased during COVID-19, and the distribution of pathogens also changed [26]. This suggests that clinicians should fully consider the age and epidemic trends of children when empirically using antibiotics.
In our study, the incidence of drug-resistant bacteria gradually decreased, with the highest proportion of 29.2% in 2017 and the lowest of 11.7% in 2022, representing a significant reduction (p < 0.001). Except for CRE and MRSA, the infection rates of the MDR, ESBL, CRABA, and CRPAE strains exhibited a consistent downward trend annually (p < 0.001). This is similar to the results reported by the Infectious Disease Surveillance of Pediatrics program on bacterial epidemiology and antimicrobial resistance in children in China between 2016 and 2020 [27]. Drug-resistant bacteria are associated with an increased risk of treatment failure and relapse. Thus, they are important drivers of increased morbidity and mortality rates [28]. We inferred that this downward trend is attributable to the standardized use of broad-spectrum antibiotics in recent years and the COVID-19 pandemic [27, 29]. Bacterial adaptability and resistance can be minimized by standardizing and optimizing the use of antimicrobials, thereby reducing the emergence and spread of drug-resistant bacteria [29]. Improving the quality of antibiotic use is a primary objective of the World Health Organization's global action plan to combat antimicrobial resistance. Notably, there is substantial variation in the use of access, watch, and reserve antibiotics among neonates and children [30]. A report from the United Kingdom indicated that antibiotic use during primary health care significantly exceeded established guidelines, leading to excessive prescription [31]. Conversely, another report from Europe revealed that one-third of antibiotic prescriptions for children with fever were deemed unreasonable or uncertain, suggesting that antibiotic management should be implemented to limit usage until pathogenic bacteria are accurately identified [32]. Therefore, it is particularly important to analyze the distribution of drug resistance in severe pulmonary infections. This can guide clinicians in making empirical drug choices before determining the cause of the infection, thereby reducing inappropriate antibiotic use.
However, the COVID-19 pandemic has significantly increased the public awareness of infection prevention and hand hygiene. Parents paid more attention to their children's hygiene problems, such as washing hands and wearing masks. Restrictions on outdoor activities reduced the frequency of personal contact. These public health measures help to reduce the spread of pathogens and the risk of infection by drug-resistant bacteria [33]. Additionally, medical institutions have stepped up infection control measures, including hand hygiene, environmental cleaning, and equipment disinfection, which diminishes the likelihood of nosocomial transmission and cross-infection by drug-resistant bacteria [34].
The difference in pathogen distribution among hospitalized children with severe pulmonary infection was mainly reflected in the neonatal intensive care unit (NICU) and pediatric intensive care unit (PICU). Compared to the statistical results from the China Antimicrobial Resistance Surveillance System regarding the detection rates of pathogens in intensive care units across all age groups, notable differences were observed among Klebsiella pneumoniae, Pseudomonas aeruginosa, Acinetobacter baumannii, and Streptococcus pneumoniae [35]. The detection rate of drug-resistant bacteria, such as ESBLs and CREs, in children was higher than that in adult care units, which aligns with the infection characteristics observed in pediatric populations [36]. Therefore, it is essential to develop a nosocomial infection control strategy that specifically targets pathogenic bacteria associated with pediatric infections.
Our study had limitations. First, the data were obtained from a single tertiary hospital, which potentially limits the generalizability of our results to lower-level medical centers. Second, our study lacked a joint analysis of multi-center data, which may influence the scope and applicability of our findings. Finally, we did not analyze the specific antibiotic resistance of drug-resistant bacteria, hindering our ability to assess the appropriateness of antibiotic selection.




Comments (0)