
Remember me



The questionnaire was filled out by 553 pediatricians from 17 out of 20 Italian Regions: 35,3% from North Italy, 38.9% from Central Italy and 25,8% from South Italy and Islands.
72% of pediatricians had more than 20 years of practice as primary care pediatricians and only 5.4% of participants had less than 5 years of work experience. 53% of participants reported to see about 5–10 children per year with delayed mild-moderate MPE over the course of antibiotic (mainly BL) treatment. Moreover, in the last 5 years, 21% of pediatricians managed about 11–20 children with such a type of reaction and 14.8% of participants evaluated more than 20 patients. In case of suspected MPEs occurring during antibiotic treatment, pediatricians followed different approaches to manage patients: only 25% of general practitioners were used to take a picture of the skin lesions; 47% of them used to assess the extension and the presence of itching; 66% used to ask about the time latency and 48.5% used to follow up patients with acute MPE by performing an “in person” visit after 24 h. In case of MPEs occurrence during fever and concomitant antibiotic treatment: 58,2% of primary care pediatricians interrupted the antibiotic treatment and 41.8% continued to treat the patient with the same antibiotic, shortly re-evaluating the patient. Among those who interrupted the drug: 52% prescribed antihistamines and 32.8% prescribed both antihistamines and corticosteroids. Of those who continued the antibiotic treatment, 61.7% added antihistamines.
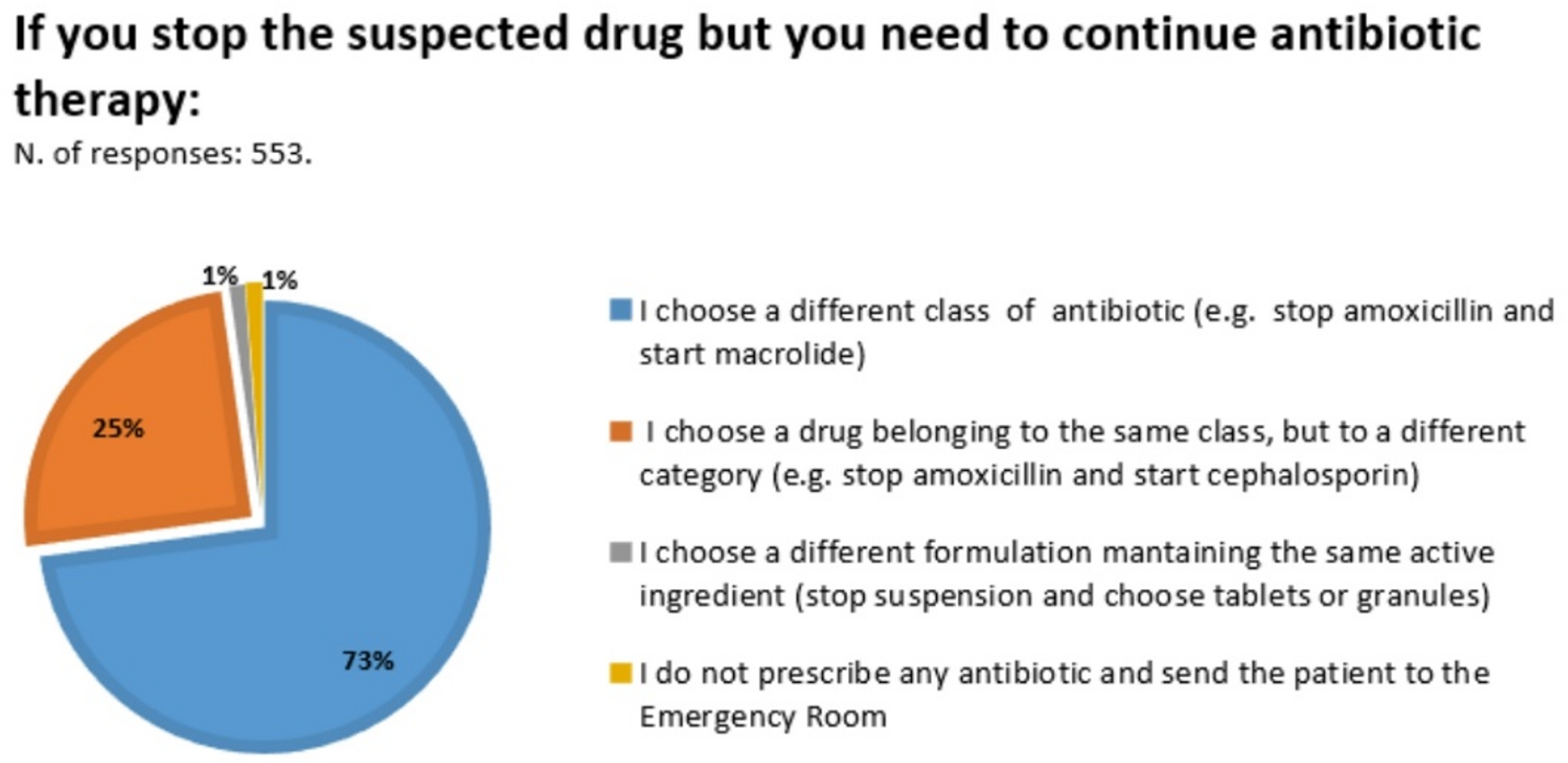
When the antibiotic was stopped and it was necessary to treat the disease with an alternative drug, 72.9% of participants switched to a different antibiotic class (i.e., macrolides); 24.9% of participants chose an antibiotic belonging to the same class (i.e. a third-generation cephalosporin was most commonly prescribed when a MPE occurred during amoxicillin/clavulanic acid treatment and vice versa) (Fig. 1).
Fig. 1
In case of future necessity of the same BL antibiotic that provoked a mild-moderate MPE: 50.4% of participants prescribed a different class of antibiotic (i.e. macrolides); 28% choose a different antibiotic of the same class (for example a cephalosporin instead of amoxicillin); 21.2% of pediatricians prescribe again the same molecule (11.2% at home, 4.9% by administering the first dose in an out-patient setting, 5.1% combining the antibiotic with anti-histamine).
The 131 primary care pediatricians who have prescribed the same molecule, for example a BL that provoked a mild MPE, stated that 26,7% of patients always tolerate the same antibiotic, 67,9% of patients often tolerate the same antibiotic and 5.3% of patients rarely tolerate the same antibiotic.
In case of delayed mild-moderate MPE during BL treatment, more than half of participants (57%) referred patients to the allergist only in case of recurrent reactions with the same molecule or with a different one. Patients were always referred to the allergist by 17.2% of participants, by 8.9% only in case of family history of drug allergy, by 7.1% only in case of switch to a different molecule. It is noteworthy that 9.9% of participants never referred those patients to the allergist (Fig. 2).
Fig. 2
Regarding the timing for referral, 42.8% of participants think that the allergy work-up should be performed within 3–6 months from the reaction; 28% within a month, 10.3% within 12 months and 19% think that the timing for allergy evaluation should be adapted to the age of patient.
When a complete allergy work-up including a negative drug provocation test showed that the suspected drug was tolerated, 81% of participants feel confident in prescribing again the same antibiotic while 16.6% of participants would not prescribe again the drug in question and 1.3% of participants leave the decision to the family.
Comments (0)