
Remember me
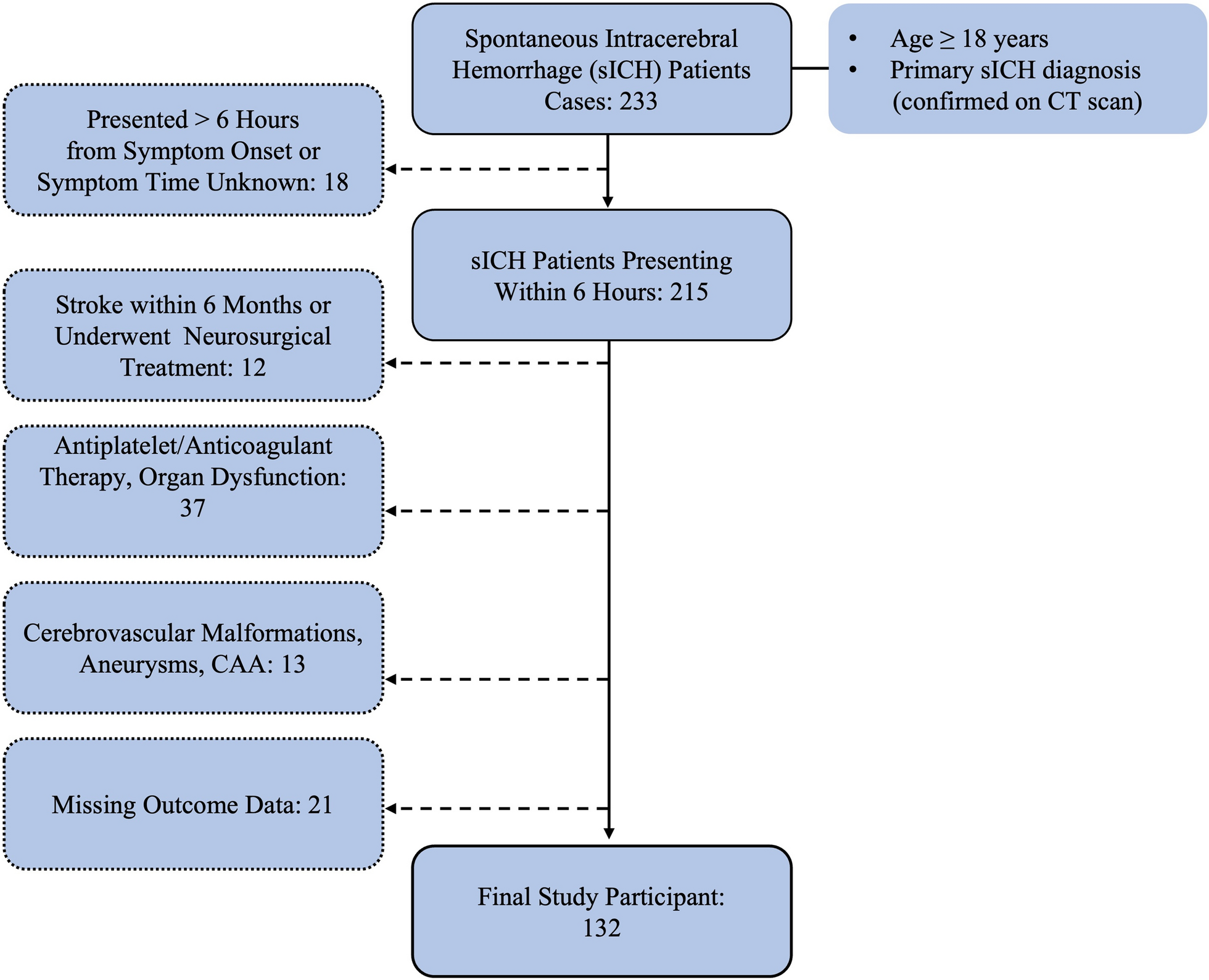
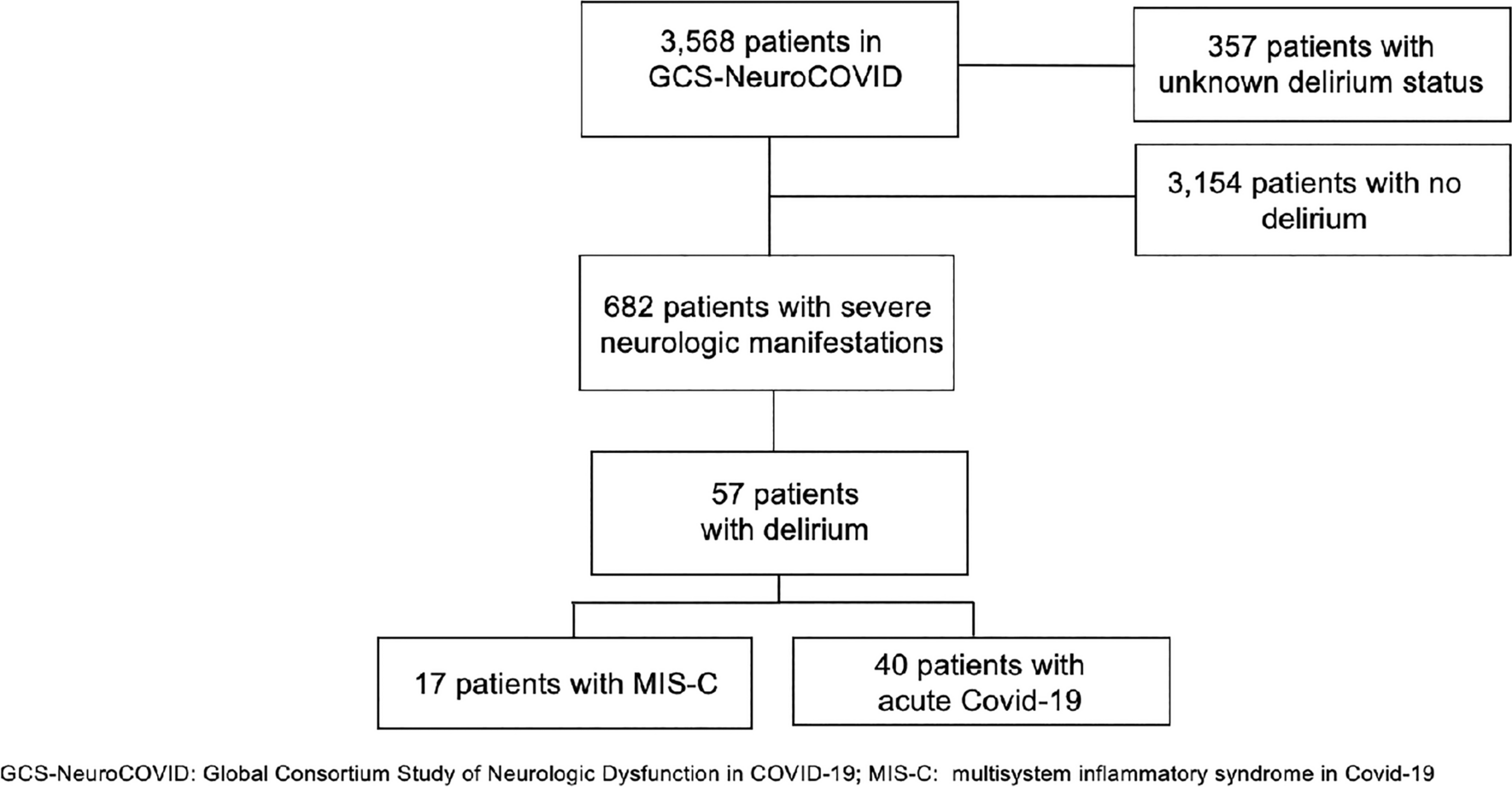
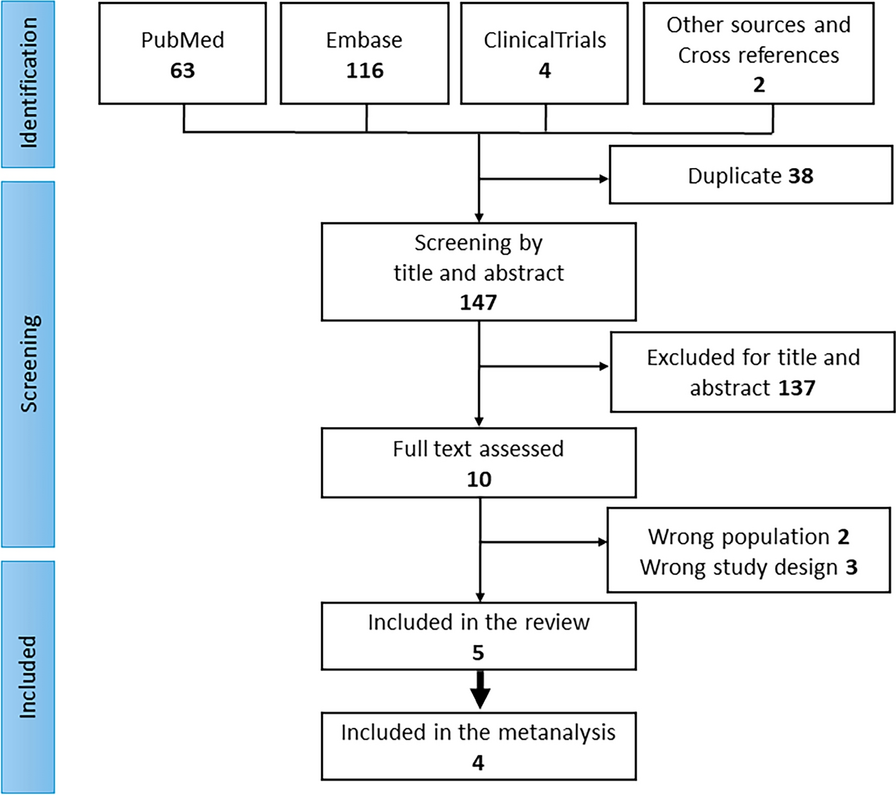
Applying the prespecified search term, 103 patients were identified. Two cases were excluded for poor image quality. After subtracting four duplicates and one patient who did not meet the TOBS definition, 96 patients were finally included in the study (Fig. 1).
Fig. 1
Study flowchart describing the data procurement and stepwise patient selection process intended for retrospective analysis. Further search terms were (translated from German): distal basilar artery thrombosis, distal basilar artery syndrome, thrombus of the distal basilar artery, thrombus in the distal basilar artery, distal basilar thrombus, and distal basilar thrombosis
Clinical Findings at AdmissionThe mean age was 70.32 years, and 41.67% of the patients were female. Seventy-two percent of the patients presented with a decreased level of consciousness, along with bulbar symptoms (dysphagia in 61%, dysarthria in 80%), hemiparesis (54%), pupillomotor deficits (46%), and oculomotor deficits (50%). The Babinski sign was positive on at least one side in 34% of the cases. The median NIHSS score at admission was 19, whereas the median prior mRS score was 1. In total, 33 patients (31%) presented with prior antiplatelet monotherapy (32 patients with aspirin, 1 with clopidogrel) and 5 patients (5%) presented with dual antiplatelet therapy, all of them due to recent cardiac interventions (coronary stents). Seventeen patients (18%) presented with prior oral anticoagulation, of whom 12 patients received the vitamin K antagonist phenprocoumon and 5 patients received direct oral anticoagulants. For more baseline characteristics, see Table 2.
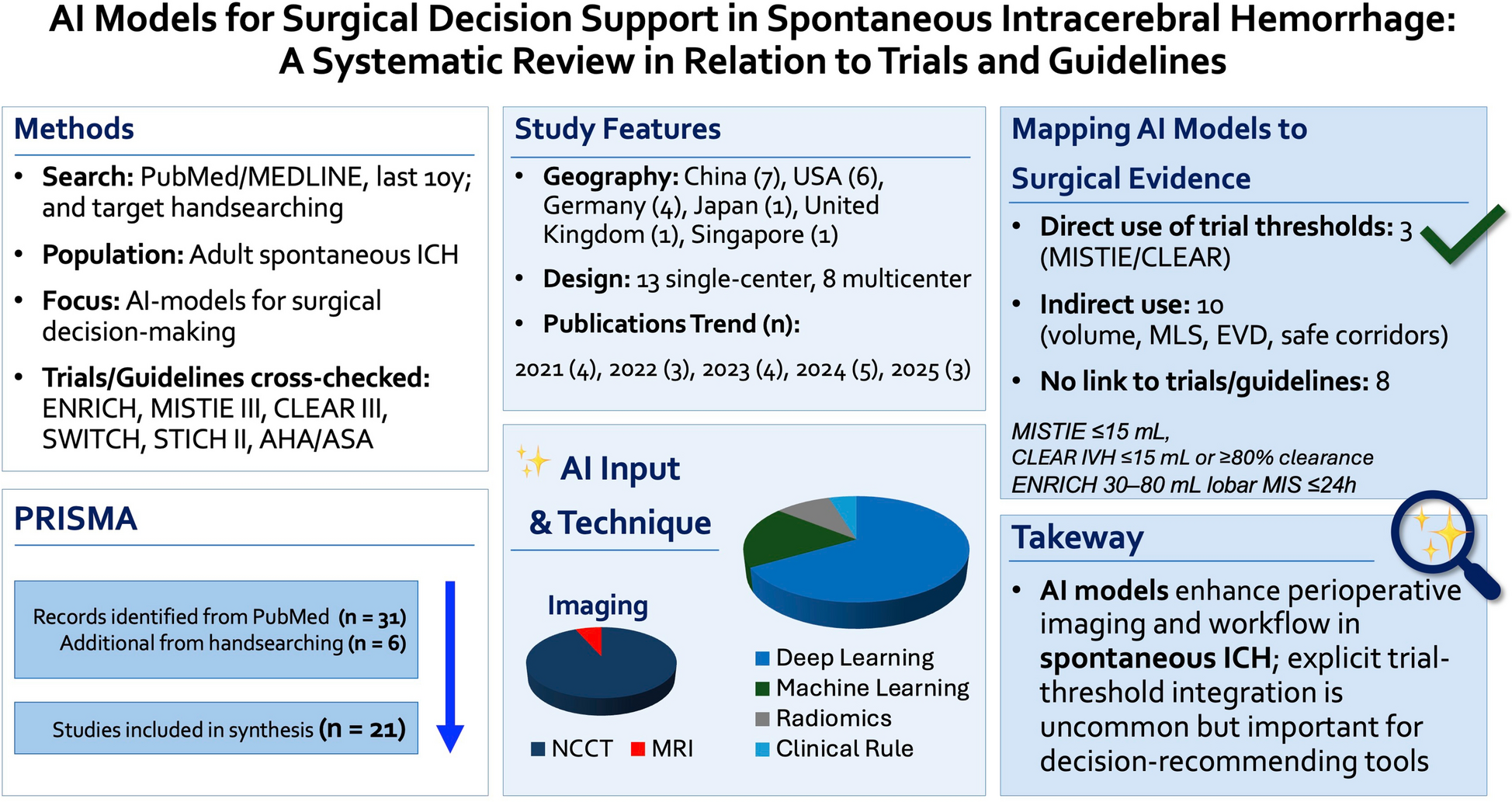
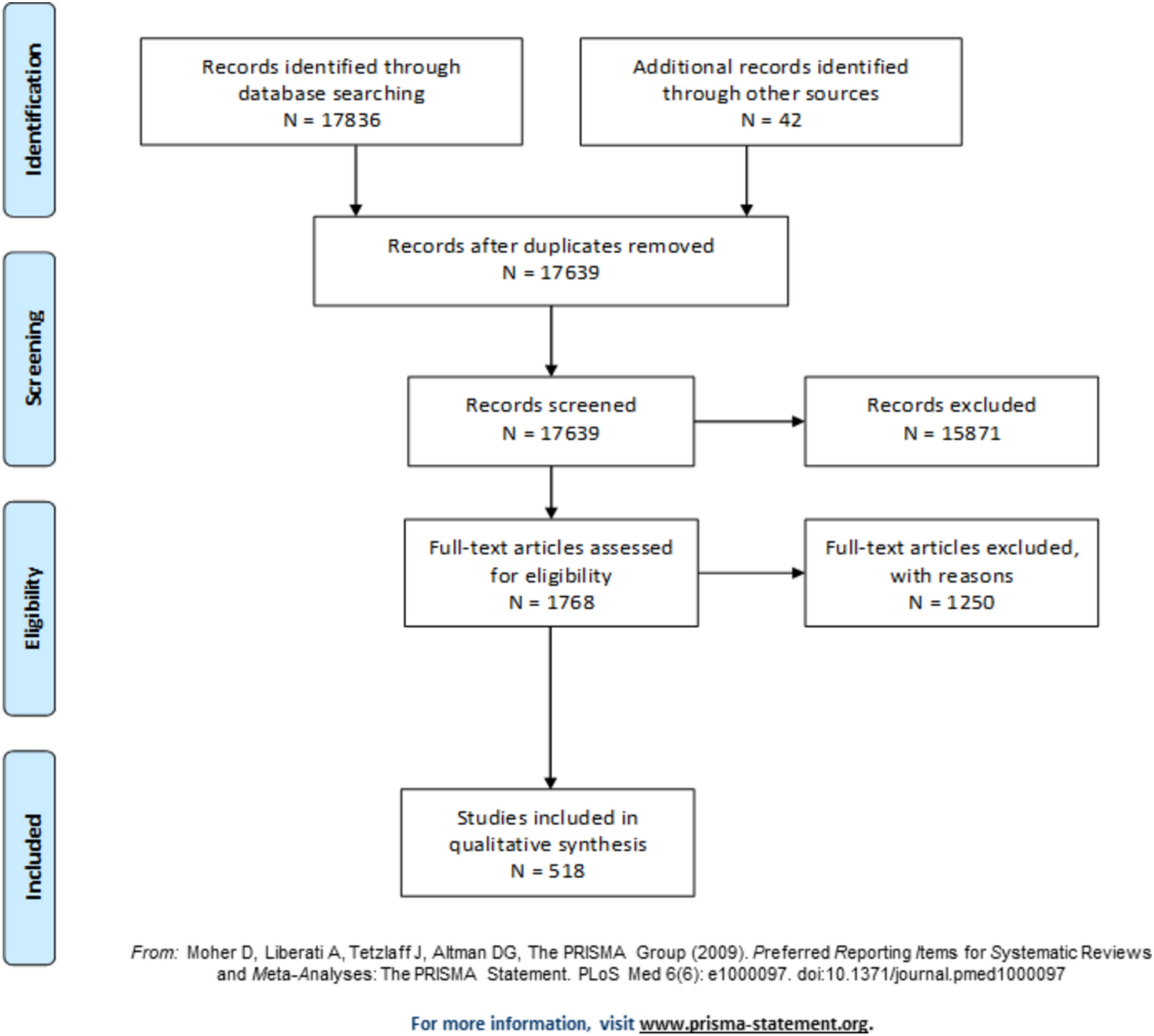
Table 2 Patient baseline characteristicsRadiological Findings at AdmissionThe mean length of the thrombi was 9.6 mm (± 6.5 mm) and most frequently included an additional occlusion of the P1 segments with slightly more frequent involvement of the left side (Supplemental Table S1). Overall, 46 patients (49%) did not show any infarcts in the initial imaging. Infarction of the thalamus was found unilaterally in 13 (13.7%) and bilaterally in 7 cases (7.4%). In addition, 13 patients (13.7%) had unilateral occipital infarcts, and 2 (2.1%) had bioccipital infarcts. Overall, 22 patients (23.2%) showed infarcts of the mesencephalon, 17 (17.9%) showed infarcts of the pons, 19 (20%) had unilateral cerebellar infarct, and 11 (11.6%) had bilateral cerebellar infarcts. MRI provided superior infarct delineation compared to CT, with significantly lower pcASPECTS scores (median 7 [IQR 5–8] for MRI vs. 10 [IQR 9–10] for CT, p < 0.0001; Fig. 2a).
Fig. 2
a, Frequency distribution of the pcASPECTS in the initial imaging (CT group n = 60 vs. MRI group n = 36; p < 0.0001). b, Sankey diagram of treatments. Made with SankeyMATIC.com. CT computed tomography, IVT intravenous thrombolysis, MRI magnetic resonance imaging, MT mechanical thrombectomy, pcASPECTS posterior circulation Alberta Stroke Program Early CT Score
One patient was identified in whom a partial thrombosis of an unruptured giant basilar artery aneurysm caused TOBS (representing Castaigne syndrome). After a thorough workup, we assumed that a carryover of thrombotic material from the aneurysm into both P1 segments and both SUCAs caused an extended infarction (bioccipital, bimesencephalic, bicerebellar, left pontine, and left thalamic).
Treatment DecisionsIn our cohort, 11 patients (11%) received IVT only, 45 patients additionally received MT (IVT + MT 47%), 30 patients received MT without thrombolysis (32%), and 10 patients received no acute recanalizing therapy in the form of MT or thrombolysis (10%; Fig. 2b). Time windows from symptom onset to arrival at our comprehensive stroke center were not statistically significantly different between the treatment groups (Kruskal–Wallis test p = 0.5877; Supplemental Table S2). IVT initiation was often precluded by preexisting infarct demarcation (in 52.2% of the cases), prior anticoagulation, time window limitations, or bleeding risks (for details, see Supplemental Table S3). Anticoagulation or antiplatelet therapy was adjusted based on individual risk profiles, including atrial fibrillation detection and stent placement. Detailed information on the secondary prevention strategies can be found in the supplementary material.
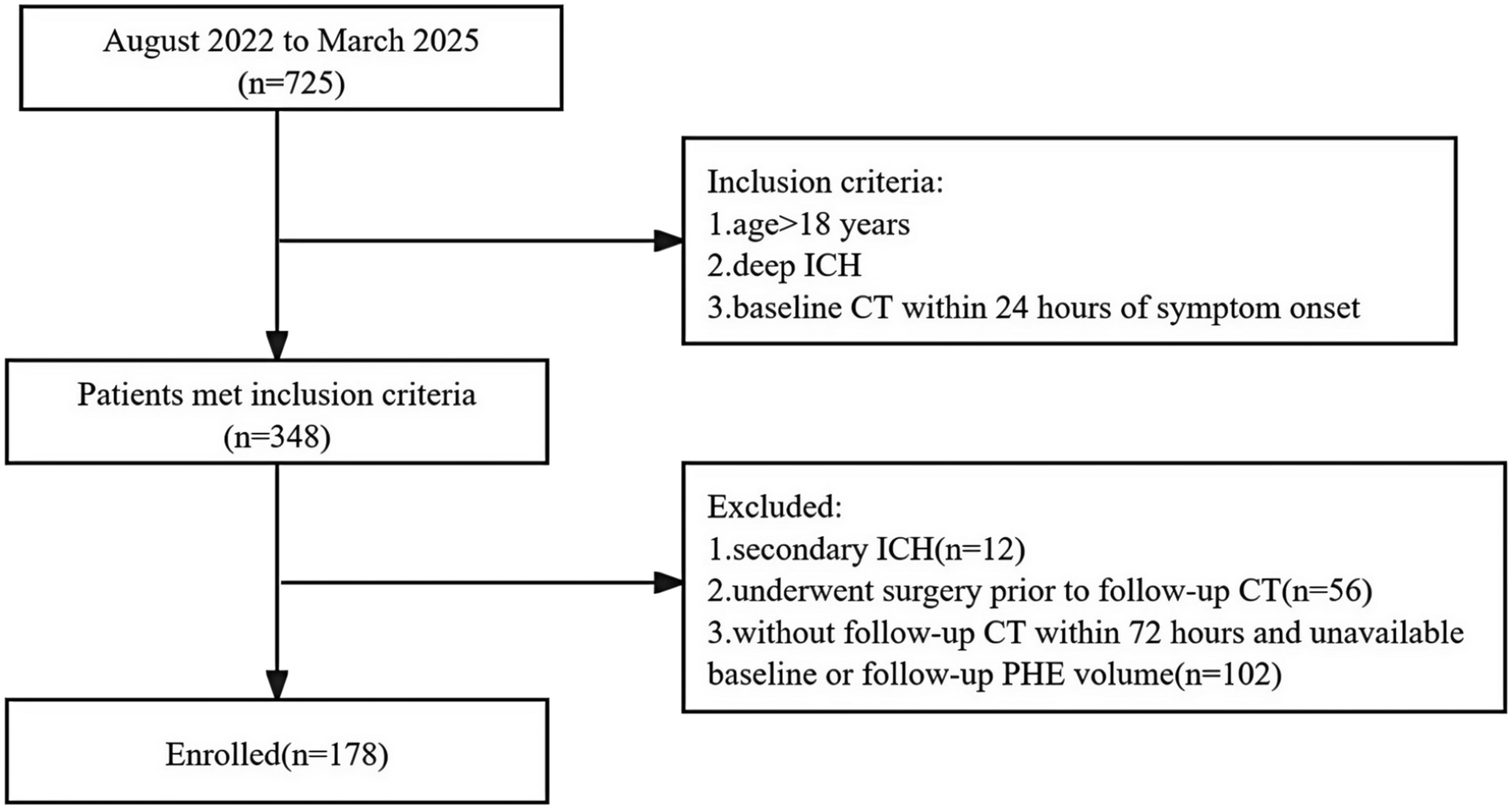
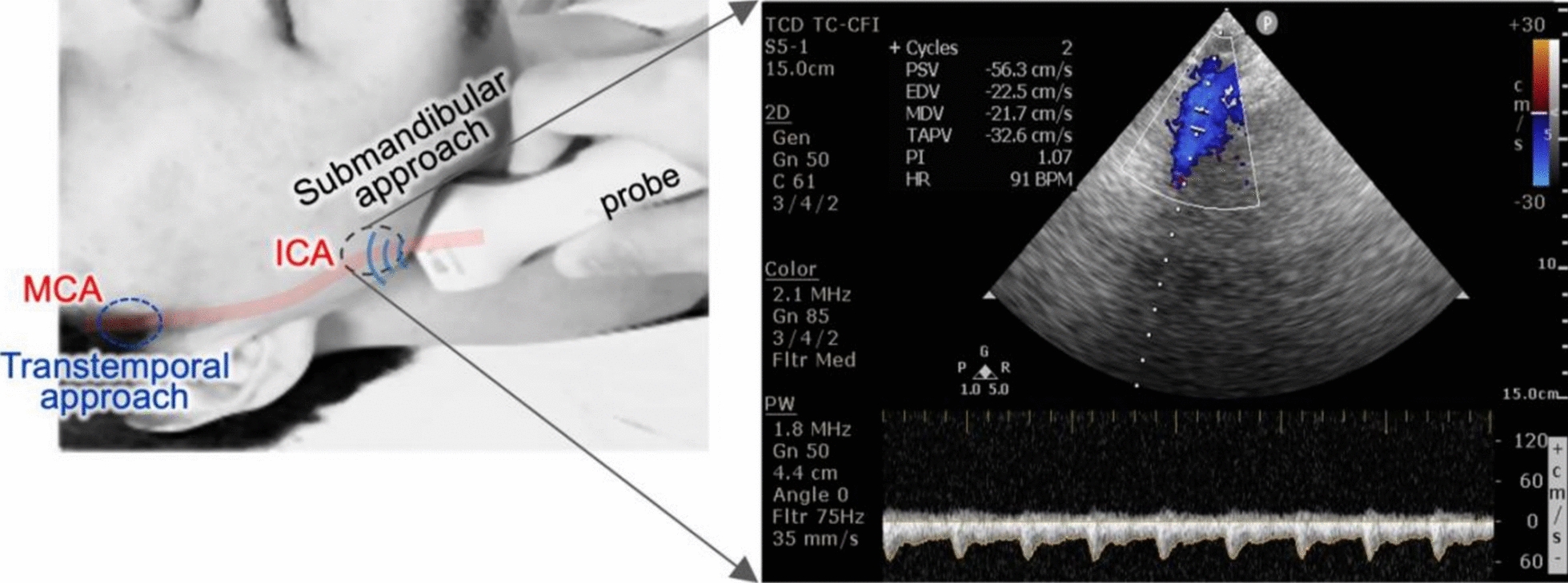
Reperfusion StatusReperfusion status (represented by mTICI) in the follow-up imaging was significantly different between dependent, bedridden, or dead patients (mRS score 3–6, n = 67) and patients with a good functional outcome (mRS score 0–2, n = 24, p < 0.0001; Fig. 3b). Higher rates of successful recanalization were detected in patients receiving at least one kind of recanalization therapy or the combination of both treatments compared to patients without any recanalization therapy (p < 0.0001, Fig. 3a). However, data (especially for individuals without any acute recanalization therapy) were incomplete. As a result, the group sizes varied greatly here (IVT only group n = 10, IVT + MT group n = 24, MT only group n = 30 vs. no IVT, no MT group n = 6).
Fig. 3
a, Frequency distribution of the reperfusion status (represented by mTICI score) in the individual treatment groups (IVT only group: 30% TICI 0, 30% TICI IIb, 40% TICI III; IVT + MT group: 9% TICI 0, 42% TICI IIb, 4% TICI IIc, 44% TICI III; MT only group: 17% TICI 0, 3% TICI I, 3% TICI IIa, 30% TICI IIb, 47% TICI III; no IVT + no MT group: 67% TICI 0, 17% TICIIIb, 17% TICI III; p < 0.0001). b, Frequency distribution of the reperfusion status in the dependent (mRS 3–6) vs. the independent (mRS 0–2) patients (mRS 3–6 group: 24% TICI 0, 1% TICI I, 1% TICI IIa, 37% TICI IIb, 1% TICI IIc, 34% TICI III; mRS 0–2 group: 29% TICI IIb, 4% TICI IIc, 67% TICI III; p < 0.0001). IVT intravenous thrombolysis, mRS modified Rankin scale, MT mechanical thrombectomy, TICI Thrombolysis in Cerebral Infarction
FEES Assessments During Ward StayFifty-eight of the patients (60.42%) were treated by our speech and language therapists during their hospital stay, 16 (27.59%) of whom were examined by FEES. Thirty-eight of the patients (39.58%) were not examined because of persistent intubation/severe vigilance disorder. Of the 58 patients examined (+ /−FEES), 30 (51.72%) showed dysphagia and 28 (48.28%) did not. Of the 30 patients with neurogenic dysphagia, 11 patients (36.67%) were discharged or transferred with a nasogastric tube (and thus a poorer prognosis for full recovery of the dysphagia). Fifteen patients (50%) were at least partially to fully oralized. No information on the nutritional status of four patients (13.33%) was available at discharge. Among the 42 patients who did not undergo FEES but were alert enough for a clinical swallowing examination, 22 (52.4%) patients did not have adequate cooperation or alertness for FEES, 13 (31%) showed normal findings, and 7 (16.6%) exhibited abnormalities, though none required a nasogastric tube.
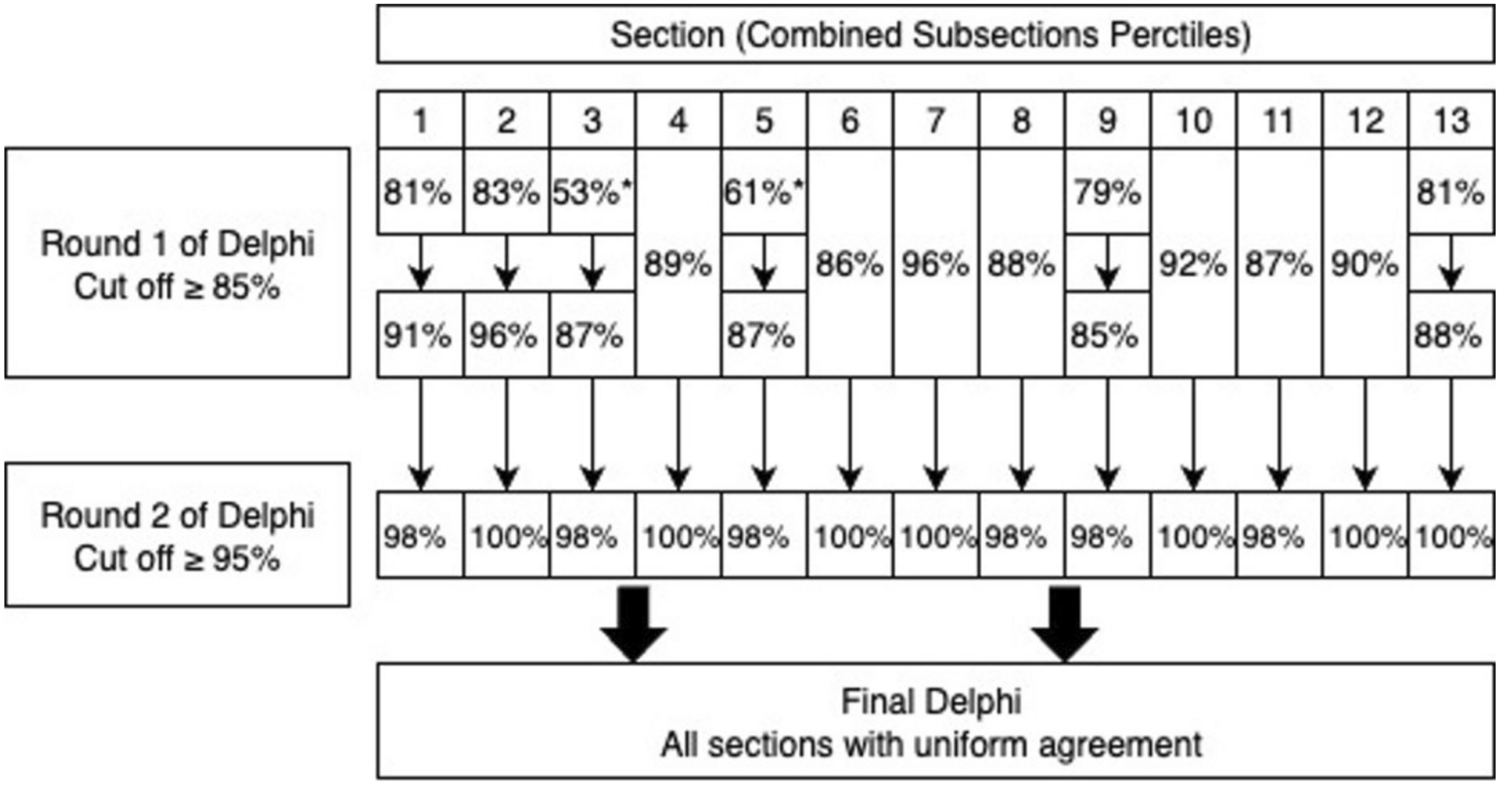
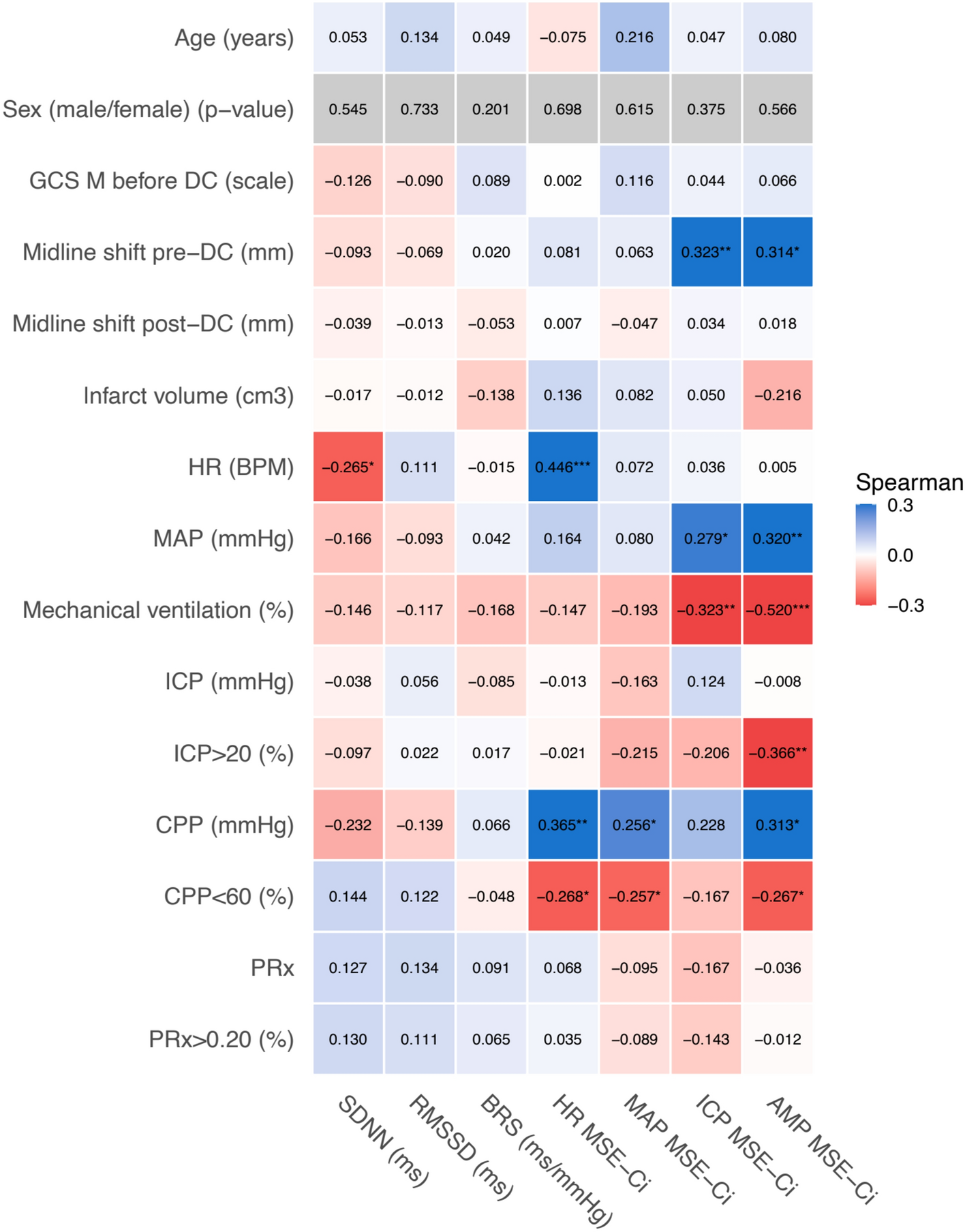
Clinical Outcomes at DischargeAlthough not designed for therapy comparisons, our study found significant differences in functional outcomes. Patients treated with both IVT and MT showed better NIHSS scores at discharge (median 4, IQR 1–20, n = 45) compared to patients treated with IVT alone (median 9, IQR 2–35, n = 11), MT alone (median 20, IQR 4–42, n = 30), or no therapy (median 32, IQR 2–42, n = 10; p = 0.0115; Fig. 4b). The median mRS score at discharge was 4 for IVT (IQR 3–6, n = 11) or IVT + MT (IQR 2–5, n = 45) and 5 for MT alone (IQR 2–6, n = 30) or no therapy (IQR 4–6, n = 10; p = 0.0845; Fig. 4a). Among MT patients, those with prior IVT had significantly better mRS outcomes (Mann–Whitney U-test between IVT + MT [n = 45] and MT only [n = 30] groups, actual median rank difference 1, p = 0.046).
Fig. 4
a, Frequency distribution of the neurological outcome based on mRS at discharge (IVT only group: n = 11; IVT + MT group: n = 45; MT only group: n = 30; no IVT + no MT group: n = 10; p < 0.001). b, median NIHSS score at discharge (IVT only group: 9 [IQR 2–35], n = 11; IVT + MT group: 4 [IQR 1–20], n = 45; MT only group: 20 [IQR 4–42], n = 30; no IVT + no MT group: 32 [IQR 2–42], n = 10; p = 0.0115). IQR interquartile range, IVT intravenous thrombolysis, mRS modified Rankin scale, MT mechanical thrombectomy, NIHSS National Institutes of Health Stroke Scale
In the univariate analysis (Spearman correlation), the NIHSS and GCS scores at admission, prior mRS score, thrombus length, age, and success of recanalization assessed by the TICI score were significantly associated with functional dependence at discharge as measured by mRS and BI (Supplemental Table S3). In a next step, we added a multivariable median regression model that (consistent with the results of the univariate analysis) identified recanalization success, as measured by the TICI score, and the GCS score at admission as independently associated with functional outcome at discharge, as measured by mRS and BI, respectively (Table 3). When comparing patients with favorable outcome (mRS score ≤ 2) and patients with poor outcome (mRS score ≥ 3), we identified a detrimental impact of ataxia and thalamic infarcts (Table 4).
Table 3 Multivariable median regression model for functional outcomesTable 4 Association of case characteristics with functional outcome at discharge
Comments (0)