
Remember me
An in-depth description of the methodology used in these guidelines is available in Supplementary Appendix 1.
Selection of Candidate PredictorsThe following candidate predictors were selected on the basis of clinical relevance AND the presence of an appropriate body of literature, using criteria described in Supplementary Appendix 1:
Clinical Variables 1.Age
2.National Institutes of Health Stroke Scale (NIHSS) on admission
3.Blood glucose
4.Cerebral collateral circulation status
5.Hypertension
6.Infarct size
7.History of previous stroke
8.Revascularization status
9.Early neurological improvement (ENI)
Clinical Prediction Models 1.Acute Stroke Registry and Analysis of Lausanne (ASTRAL) score
2.Dense Artery, mRS, Age, Glucose, Onset-to-Treatment, and NIHSS (DRAGON) score
3.Ischemic Stroke Predictive Risk Score (iScore)
4.Totaled Health Risks in Vascular Events (THRIVE) score
PICOTS QuestionThe Population/Intervention/Comparator/Outcome/Time frame/Setting (PICOTS) question was then framed for the specific candidate predictors as follows:
“When counseling critically ill adults with acute ischemic stroke or their surrogates, should <predictor or prediction model, with time of assessment if appropriate> be considered a reliable predictor of <outcome>?”
Selection of OutcomesThe topic experts and the patient and family representative rated outcomes on the GRADE 1–9 scale on the basis of their perceived importance. Outcomes with a median rating of 7–9 were considered “critical.” While quality of life, cognitive function, and depression were critical outcomes, the body of evidence with these outcome measures was insufficient to support any recommendations. In addition, the risk of bias from the self-fulfilling prophecy within the existing body of literature on predictors of mortality was considered too high to recommend any single clinical variable to predict death when all available means of life support are used, indefinitely and without limitation [18]. A brief summary of the GRADE evidence profile and summary of findings for predictors of mortality is given in Supplementary Table 1, while a summary of recommendations for predictors of mortality is provided in Supplementary Table 2. The recommendations within these guidelines are primarily focused on the prediction of functional outcome.
Functional Outcome AssessmentThe majority of studies used the modified Rankin Scale (mRS), which ranges from 0 (asymptomatic) to 6 (death), as a measure of functional outcome [19, 20]. The definition of a “good” or “poor” functional outcome has varied across the literature. In recognition of the evolution in outcome analysis in the ischemic stroke literature (described in Supplementary Appendix 1), an inclusive definition was used for the purposes of this systematic review, encompassing all of the mRS thresholds and analyses described. Variability in outcome definition was, therefore, an inherent limitation of the review. Other acceptable measures of functional outcome in the literature included the Barthel Index, Glasgow Outcome Scale (GOS), Functional Independence Measure (FIM), and Lawton’s Activities of Daily Living (ADL) scale.
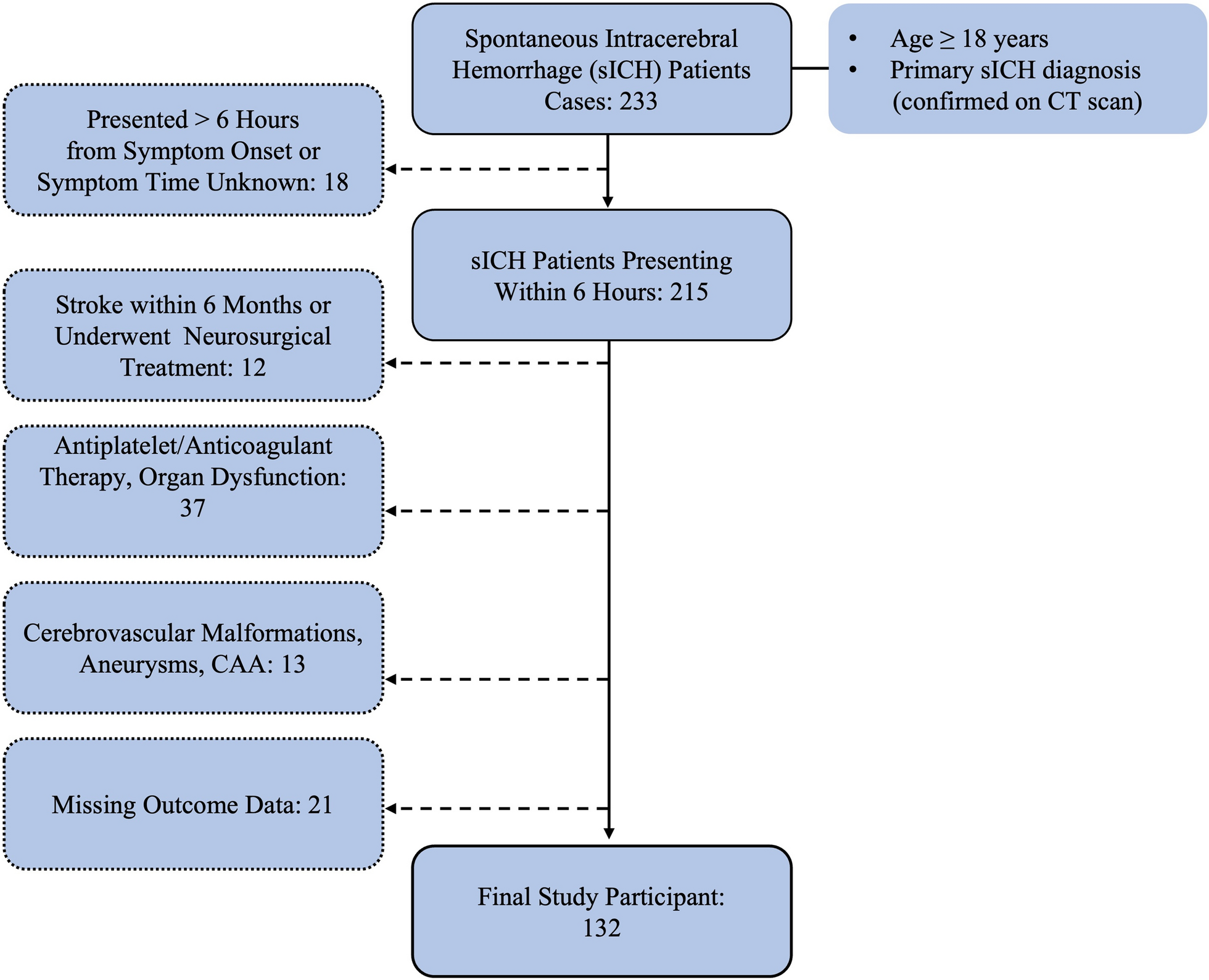
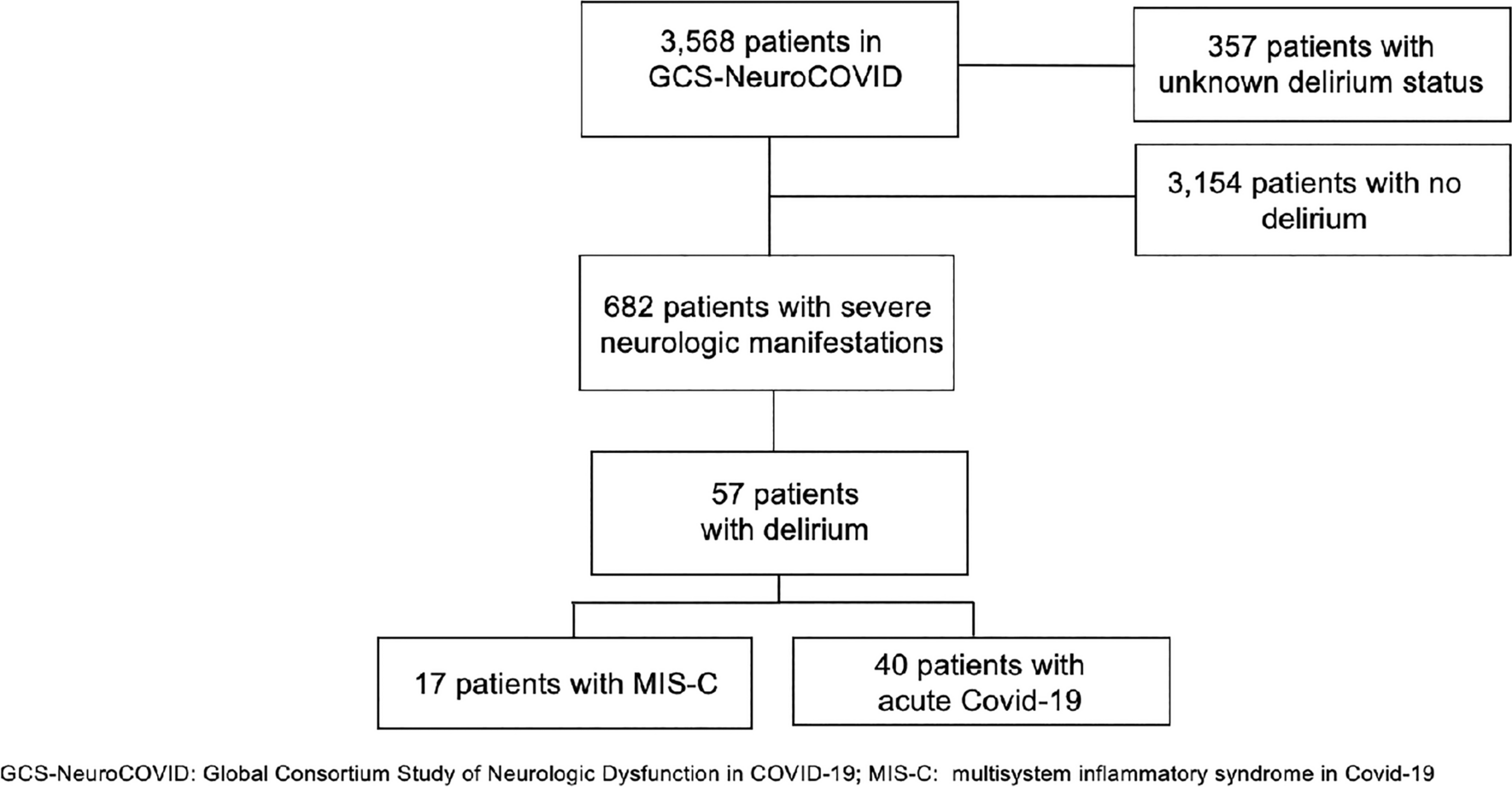
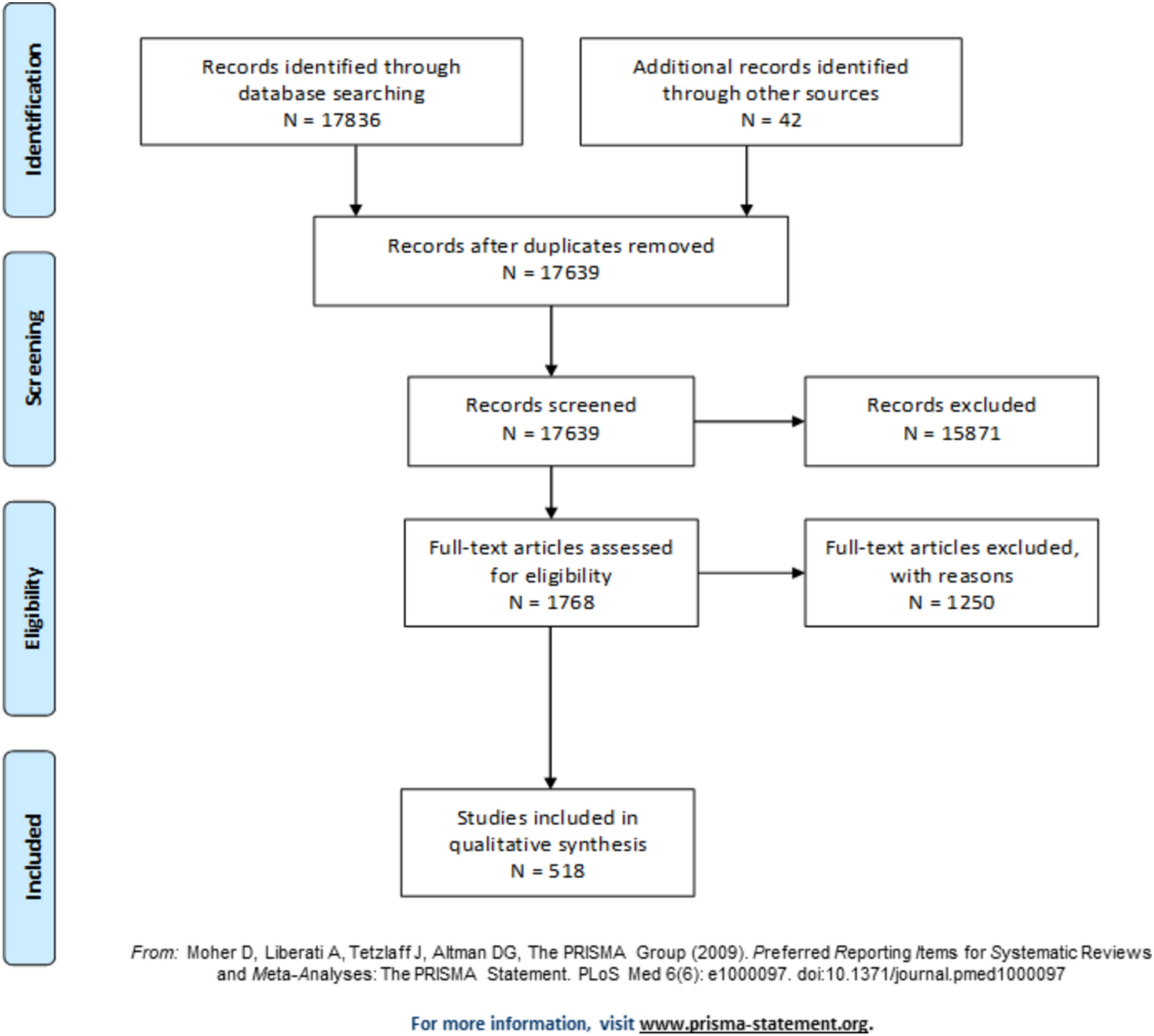
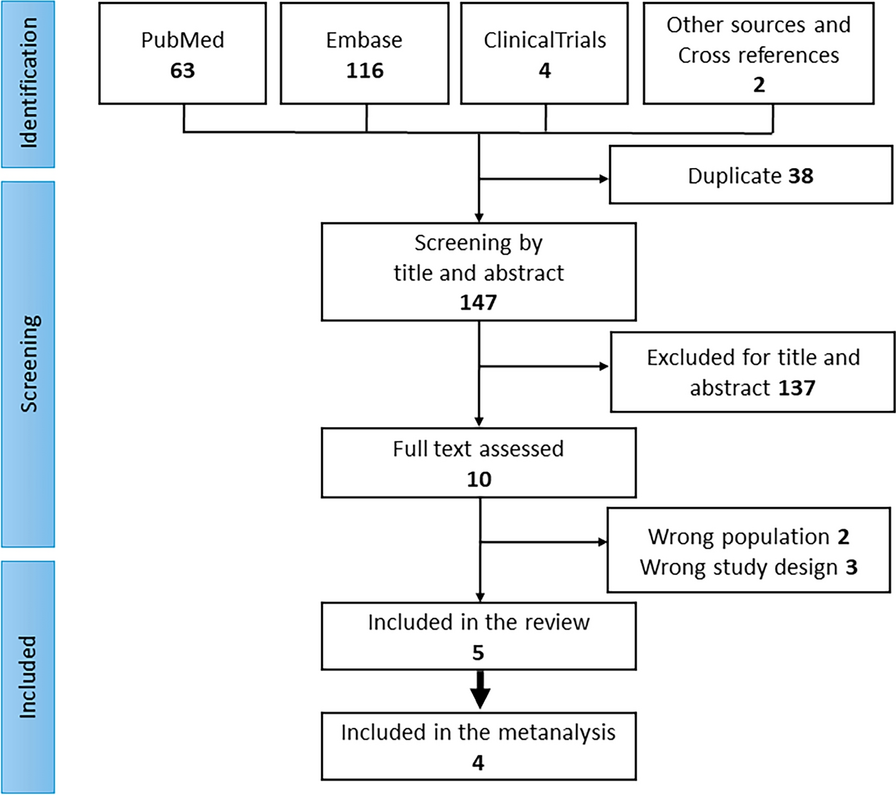
Systematic Review MethodologySince the literature on prognosis was expected to be heterogeneous, a narrative systematic review was performed. An in-depth description of systematic review methodology overall for the NCS–DGNI neuroprognostication guidelines project is given in Supplementary Appendix 1. The initial librarian search string was appropriate to the question “What are the reliable predictors (prognostic factors, variables, tests, scores, and multivariable models), prior to and on admission as well as during the hospital course to predict patient outcome at different follow-up time-points following each specific disease ?”, to identify candidate predictors. Screening of articles was completed using DistillerSR software (Evidence Partners, Ottawa, Canada). The librarian search string used for this systematic review is provided in Supplementary Appendix 2. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram is shown in Fig. 1. The initial librarian search was performed on 20 February 2019 and encompassed the period from 1946 to the search date. Databases searched included MEDLINE via PubMed, EMBASE, Web of Science, and the Cochrane Database of Systematic Reviews. Updated searches were performed on 1 August 2022 and 5 February 2024.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.PRISMA 2009 flow diagram depicting the study selection process for the systematic review, including records identified, screened, excluded, and included in the final analysis
Article ScreeningFollowing title and abstract screening, full-text screening was performed with the following exclusion criteria: (1) sample size less than 100 adult patients, (2) studies focused exclusively on transient ischemic attack (TIA) and/or mild stroke, (3) studies focused on a highly selected subgroup (such as periprocedural stroke), (4) studies of predictors not evaluated in multivariate analysis, (5) studies focused on a genetic polymorphism as a predictor, and (6) studies of clinical prediction models that did not report model discrimination.
Risk of Bias (RoB) AssessmentData extraction and assessment for risk of bias (RoB) was performed for studies that addressed the PICOTS question and fulfilled full-text selection criteria. The Quality in Prognostic Studies (QUIPS) RoB instrument was used to evaluate studies of individual prognostic variables [21]. The Prediction model Risk Of Bias ASsessment Tool (PROBAST) instrument was used to evaluate studies of clinical prediction models [22, 23]. In addition to the standard domains of these RoB instruments, studies were evaluated for the risk of bias related to the self-filling prophecy with an additional domain that included three questions: whether a treatment suspension policy was used in the study, whether clinicians were blinded to the predictor, and whether the predictor was systematically utilized by clinicians for prognostication during the time period of the study. A content expert evaluated each study for RoB, with secondary review by another content expert. Articles written or co-written by one of the authors were independently assessed for risk of bias by another author and a methodologist. Following assessment of risk of bias in each domain, an overall risk of bias—high, moderate, or low—was assigned to each study.
GRADE Assessment and Evidence ProfileFollowing data extraction and assessment of risk of bias of individual studies, a GRADE evidence profile with summary of findings table was constructed. The body of evidence was downgraded once for a moderate overall RoB across all individual studies and twice for a high overall RoB. Since most studies of predictors following AIS were not limited to critically ill patients admitted to the ICU, a downgrade for indirectness was required for the body of evidence for most PICOTS questions.
A summary of individual studies is provided in Supplementary Table 3. The GRADE evidence profile and summary of findings table for predictors of functional outcome are presented in Table 2. A summary of PICO recommendations is given in Table 3, while a color-coded summary of reliability of predictors is presented in Table 4. A summary of good practice statements is given in Table 5.
Table 2 GRADE evidence profile/summary of findings table: neuroprognostication—acute ischemic strokeTable 3 Recommendations: guidelines for neuroprognostication in acute ischemic strokeTable 4 Reliability of predictors of functional outcomeTable 5 Good practice statementsEvidence to Recommendation Criteria 1.Quality of evidence/certainty in the evidence and effect size: For the purposes of these guidelines, predictors described as “reliable” have both a higher overall certainty in the evidence and greater effect size than “moderately reliable” predictors (Table 1). The acceptable threshold for predictors of good outcome was considerably lower than for predictors of poor outcome, since an inappropriate prediction of good outcome is not expected to lead to a potentially irreversible decision such as WLST.
2.Balance of desirable and undesirable consequences: An accurate prediction of poor outcome is expected to result in grief, a sense of loss and anxiety about the future. However, accurate prediction of a poor outcome is overall desirable, since it allows surrogates and the clinical team to align goals of care to the perceived wishes of the patient with AIS, through the process of shared decision-making. Potential benefits to the family and surrogates in this situation include greater certainty and decreased decisional conflict in making patient value-congruent decisions, a sense of closure, and satisfaction from respecting the patient’s wishes. An inaccurate prediction of a poor outcome (i.e., a false-positive prediction of poor outcome), however, may lead to WLST in a patient with AIS who would otherwise have made a recovery to functional independence. Since WLST almost always leads to death in critically ill patients on life-sustaining therapy, the undesirable consequences of an inaccurate prediction of poor outcome were thought to greatly outweigh the desirable consequences, unless certainty in the accuracy of the predictor or prediction model was high. The concern for inappropriate WLST was central in the panel’s decision to recommend, or not recommend, prognostication and counseling on the basis of the selected predictors of poor outcome. The prediction of good outcome, however, involves a different balance of desirable and undesirable consequences. Patients and surrogates are likely to feel encouraged and hopeful, and continue life-sustaining treatment, which was overall considered desirable. Anticipation of a good long-term outcome may ease the psychological and physical burdens of critical illness and short-term debility, for both patients and surrogates. Anticipation of a good long-term outcome was also thought to be desirable for patient motivation during rehabilitation, which may be an independent predictor of good functional outcome following AIS [24]. An undesirable consequence of inaccurate prediction of a good outcome is disappointment and disillusionment among both patients and surrogates, which may adversely impact motivation. An inaccurate prediction of good outcome may also lead to prolongation of suffering among patients and surrogates. An additional undesirable consequence was thought to be discordance in the understanding of “good” outcome between clinicians and patients/surrogates. While clinicians generally consider a good outcome following AIS to be a return to functional independence, patients and surrogates may perceive psychological or cognitive impairment, and limitations in employment or leisure activities to represent a poor outcome despite a return to functional independence. Conversely, a physician’s perceived poor outcome might be seen by patients and families as acceptable [25,26,27]. Overall, the panel considered a prediction of good outcome to be desirable, using language commensurate to the actual likelihood of recovery, such as “more likely/more often than not,” or “highly likely, but not certain.” Clarity during counseling regarding the specific “good” outcome under discussion, such as recovery of ambulation, recovery of swallow function, or the ability to perform basic activities of daily living, was also thought to be important.
3.Values and preferences: The panel agreed that most individuals, as well as their families and surrogates, would consider an inaccurate prediction of poor outcome that led to the death of a patient who might otherwise have had a reasonable recovery to be more undesirable than a prolonged period of uncertainty in the outcome. Therefore, a high certainty in the evidence of predictor or prediction model accuracy was necessary to recommend consideration when counseling families and surrogates on prognosis in this context. Patient and family representatives on the panel, however, stated a preference for the clinical team communicating any expectations of recovery of function.
4.Resource use: An important consideration was the substantial financial burden that may be imposed on patients, surrogates, and the healthcare system with continuation of supportive measures based on an inaccurate prediction of good outcome—particularly when the patient’s outcome is inconsistent with their desired quality of life [28,29,30]. An accurate prediction of poor outcome will lead to better alignment of goals of care with the patient's wishes and avoid the extended use of resources, over days to years. The use of resources was therefore thought to favor consideration of a predictor or prediction model during prognostication, contingent on confidence in its predictive accuracy.
Recommendations: Clinical Variables as Predictors of Functional OutcomePICO question 1: “When counseling critically ill adults with AIS or their surrogates, should age alone be considered a reliable predictor of poor functional outcome assessed at 3 months or later?”.
Description of the predictor: Older age may reflect underlying frailty, the presence of comorbid conditions, and diminished cognitive reserve [31].
Recommendation: When counseling critically ill adults with AIS or their surrogates, we suggest age alone not be considered a reliable predictor of poor functional outcome assessed at 3 months or later (weak recommendation; very low quality evidence).
Rationale: The body of evidence was downgraded once each for inconsistency, indirectness, and risk of bias in the domain of study participation, attrition, outcome measurement, confounding, statistical analysis, and self-fulfilling prophecy. Despite the presence of some inconsistency, older age was a strong and independent predictor of poor functional outcome in most studies. However, age in isolation could not be recommended as a reliable predictor because older patients with AIS may nevertheless have a good functional outcome because of factors such as lower stroke severity or successful revascularization. Premorbid health and functional status varies among the elderly and may impact individual outcomes. An age threshold that universally predicts poor outcome has not been identified.
While several studies have shown that patients older than 80 years are more likely to have a poor outcome than younger patients following thrombectomy [32,33,34], data from clinical trials suggest that patients older than 85 years do not universally suffer a poor outcome. In the HERMES meta-analysis of clinical trials, patients > 85 years with premorbid functional independence treated with thrombectomy were more likely to regain functional independence (seen in 18% of patients) than control subjects [35]. Among patients 80 years and older who underwent thrombectomy, 30% regained functional independence (mRS 0–2) and 49% achieved independent ambulation (mRS 0–3) [36]. Data from clinical trials do not necessarily reflect real-world outcomes, however, since trial eligibility criteria typically select patients most likely to demonstrate benefit from the intervention. When counseling patients older than 85 years who have undergone thrombectomy, or their surrogates, we therefore suggest that statistics from clinical trials be considered a best-case estimate, and the entire range of possible outcomes be presented.
PICO question 2: “When counseling family members and/or surrogates of patients with AIS admitted to an ICU, should the admission NIHSS alone be considered a reliable predictor of poor functional outcome assessed at 3 months or later?”.
Description of the predictor: While several scales exist, the National Institutes of Health Stroke Scale (NIHSS), a 15-item scale first described in 1989 [37], was selected as the predictor in this PICO question since it is the best validated and most widely used. NIHSS was often included as a continuous variable; however, dichotomization or categorization (e.g., mild, moderate, severe) was also reported in included studies. NIHSS > 15 typically represents a severe stroke [38, 39]. Of note, the NIHSS was initially designed for use in clinical trials rather than bedside assessment, or prognostication [40].
Recommendation: When counseling critically ill adults with AIS or their surrogates, we suggest the NIHSS alone not be considered a reliable predictor of poor functional outcome assessed at 3 months or later (weak recommendation; very low quality evidence).
Rationale: The body of evidence was downgraded once each for inconsistency, indirectness, imprecision, and risk of bias in the domains of study participation, attrition, measurement of prognostic factors and outcomes, control of confounding variables, statistical analysis methods, and the self-fulfilling prophecy. Despite the presence of some inconsistency, admission NIHSS was a strong and independent predictor of poor functional outcome in most studies. However, the NIHSS in isolation could not be recommended as a reliable predictor in individual patients for several reasons. The NIHSS was measured at first assessment, prior to revascularization therapy, in most studies. Since revascularization is an effective treatment that may result in dramatic improvement regardless of baseline stroke severity, the NIHSS measured prior to therapeutic intervention is of limited prognostic value during counseling [41]. For example, in the HERMES meta-analysis, 32% of patients with the greatest stroke severity (NIHSS > 20) who underwent thrombectomy were independent (mRS 0–2) at 90 days, while 49% were able to walk independently (mRS 0–3) [36]. Second, recovery to good functional outcome was well documented across the body of evidence despite a high NIHSS assessed at various time-points during the index hospitalization. No single NIHSS threshold measured in the index hospitalization, especially in the ICU, can be used to reliably prognosticate a poor outcome in an individual patient, since factors such as young age and plasticity may result in dramatic long-term improvements with rehabilitation.
The predictive value of the NIHSS for poor outcomes does, however, increase with time: later measurements are progressively more reflective of final outcome [42, 43]. Since most patients demonstrate neurological improvement over time, the NIHSS that best predicts poor long-term functional outcome decreases with time. In the NINDS recombinant tissue Plasminogen Activator (rtPA) trial, NIHSS > 22 at 24 h had a positive predictive value (PPV) of 98% for inability to ambulate independently at 3 months, while NIHSS > 16 at 7–10 days had a PPV of 92% for prediction of the same outcome [44]. In a 2005 study, NIHSS ≥ 6 at 7 days after admission predicted poor functional outcome (inability to ambulate, death or Barthel Index < 60) with sensitivity of 84%, specificity of 92%, PPV of 77%, and NPV of 95% [43]. A consistent time of assessment and NIHSS threshold have not been identified, however. High-quality prospective studies in the era of third-generation thrombectomy devices are required to validate the predictive value of the NIHSS (or clinical prediction models that incorporate the NIHSS) measured at later time-points during the initial hospital stay [45].
PICO question 3: “When counseling critically ill patients with AIS or their surrogates, should hemorrhagic transformation alone be considered a reliable predictor of poor functional outcome assessed at 3 months or later?”.
Description of the predictor: Hemorrhagic conversion after ischemic stroke is the occurrence of bleeding within an area of the brain initially affected by ischemia. Hemorrhagic transformation has been variably defined across the literature. The European Cooperative Acute Stroke Trials (ECASS) classification includes three radiological categories: no HT, hemorrhagic infarction (HI), featuring small petechial hemorrhages along the infarct margins, and parenchymal hematoma (PH), characterized by confluent hematoma [46, 47]. The presence or absence of clinical deterioration (symptomatic vs. asymptomatic) may be incorporated into the classification, in addition to radiological features [48,49,50].
Recommendation: When counseling critically ill patients with AIS or their surrogates, we suggest hemorrhagic transformation alone not be considered a reliable predictor of poor functional outcome assessed at 3 months or later (weak recommendation; very low quality evidence).
Rationale: The body of evidence was downgraded once for inconsistency, once for indirectness, once for imprecision, and twice for risk of bias in the domains of study participation, attrition, prognostic factor measurement, outcome measurement, confounding, statistical analysis, and self-fulfilling prophecy. Across the body of evidence, a good functional outcome was feasible despite the occurrence of hemorrhagic transformation, even with concomitant clinical deterioration [51,52,53,54,55,56,57,58]. While more severe hemorrhagic transformation might be expected to have a greater impact on neurological status and functional outcome, there is an insufficient body of evidence evaluating the degree of hemorrhagic transformation as a predictor of poor outcome.
PICO question 4: “When counseling critically ill patients with AIS or their surrogates, should infarct size alone be considered a reliable predictor of poor functional outcome assessed at 3 months or later?”.
Description of the predictor: Infarct size is defined the total volume of brain tissue permanently damaged owing to insufficient blood flow. Early estimation of infarct size on computed tomography (CT) may be performed using the Alberta Stroke Program Early CT Score (ASPECTS), through identification of regions with ischemic changes [59]. Magnetic resonance imaging (MRI) with diffusion-weighted imaging (DWI) is more sensitive than CT for acute and hyperacute delineation of infarct size [60]. Final infarct size is generally established by day 30 [61]. True quantification of infarct volume requires manual tracing of the infarct perimeter, while other techniques include pixel thresholding for automated differentiation, stereological counting grids for statistical volume estimation, and measuring the largest diameters of the infarct [62]. Definitions and volume thresholds for “large” core infarcts have varied across the literature [63,64,65,66].
Recommendation: When counseling critically ill patients with AIS or their surrogates, we suggest infarct size alone not be considered a reliable predictor of poor functional outcome assessed at 3 months or later (weak recommendation; very low quality evidence).
Rationale: The body of evidence was downgraded once for inconsistency, once for indirectness, once for imprecision, and twice for risk of bias in the domains of study participation, attrition, prognostic factor measurement, outcome measurement, confounding, statistical analysis, and self-fulfilling prophecy. Substantial inconsistency was present in the body of evidence. A large core infarct at initial presentation could not, in isolation, be considered a reliable predictor of poor outcome. Infarct location and morphology may impact outcomes independent of size: the presence of infarcts confined to gray matter, infarcts sparing the corticospinal tract, and scattered (compared with territorial) infarcts have been shown to predict better outcomes, independent of infarct size [67,68,69,70]. The extent and neurological impact of cerebral edema associated with a large infarct may also impact outcome [71]. Older patients with greater cerebral atrophy may be less likely to suffer acute neurological deterioration from large infarcts [71].
Of note, several recent clinical trials of patients with large core infarcts (defined by an ASPECTS score 3–5 or core infarct volume ≥ 50 mL on perfusion imaging) have demonstrated the potential for recovery to ambulation, or even functional independence, with endovascular therapy [63]. Across trials, about 41% of patients who received endovascular therapy and 24% of patients treated medically regained independent ambulation, while 23% of patients who received endovascular therapy and 9% of patients treated medically regained functional independence. The results of clinical trials do not reflect the outcomes likely to be observed in real-world clinical practice: for example, these trials mostly excluded patients older than 80 years and all patients with baseline functional impairment. In addition, early trial termination may have resulted in overestimation of treatment effect. However, these trials do demonstrate the feasibility of good long-term outcome despite a large infarct core at presentation. We suggest that statistics from clinical trials of revascularization in patients with a large-infarct core be considered a best-case estimate of outcomes at the time of prognostication and counseling, and the entire range of possible outcomes should be discussed with patients and surrogates.
PICO question 5: “When counseling critically ill patients with AIS or their surrogates, should a history of previous stroke alone be considered a reliable predictor of poor functional outcome assessed at 3 months or later?”.
Description of the predictor: One in four patients presenting with stroke have had a prior stroke [1]. Across studies, these historical data were collected through a combination of patient- and/or surrogate-reported past medical history and examination of medical records.
Recommendation: When counseling of critically ill patients with AIS or their surrogates, we suggest a history of previous stroke alone not be considered a reliable predictor of poor functional outcome assessed at 3 months or later (weak recommendation; very low quality evidence).
Rationale: The body of evidence was downgraded once for inconsistency, once for imprecision, once for indirectness, and twice for risk of bias in the domains of study participation, attrition, prognostic factor measurement, outcome measurement, confounding, statistical analysis, and self-fulfilling prophecy. Across the body of evidence, a good long-term functional outcome was feasible in patients with a history of previous stroke.
PICO question 6: “When counseling critically ill patients with AIS or their surrogates, should successful revascularization alone be considered a reliable predictor of good functional outcome assessed at 3 months or later?”.
Description of the predictor: Revascularization or recanalization was determined after acute reperfusion therapies including thrombolysis, mechanical thrombectomy, or both. Revascularization/recanalization was most often classified according to the modified Thrombolysis in Cerebral Infarction (mTICI) scale, with successful revascularization defined as mTICI grade 2b (antegrade reperfusion of more than half of the previously occluded target artery ischemic territory), 2c (near-complete perfusion except for slow flow or distal emboli in a few distal cortical vessels), or 3 (complete antegrade reperfusion of the previously occluded target artery ischemic territory, with absence of visualized occlusion in all distal branches) [72, 73]. The thrombolysis in myocardial infarction (TIMI) grade has also been used: 0 = no recanalization, 1 = minimal recanalization, 2 = partial recanalization, and 3 = complete recanalization [74]. Repeat or follow-up imaging was most often obtained within 6–24 h after initial imaging, but could occur as early as 2 h and as late as 48 h. Typically revascularization was dichotomized into good or poor/none, though sometimes categorized as none, partial, or complete.
Recommendation: When counseling critically ill patients with AIS or their surrogates, we suggest successful revascularization alone not be considered a reliable predictor of good functional outcome assessed at 3 months or later (weak recommendation; low quality evidence).
Rationale: The body of evidence was downgraded once for imprecision and once for risk of bias in the domains of study participation, attrition, outcome measurement, confounding, statistical analysis, and self-fulfilling prophecy. The body of evidence was overall robust in identifying successful revascularization in patients who undergo thrombectomy as an independent predictor of good outcome. However, successful revascularization alone does not guarantee a good outcome since several patients will suffer infarct expansion prior to completion of revascularization or suffer a subsequent complication that compromises neurological recovery. Across clinical trials of thrombectomy, long-term recovery to functional independence was observed in fewer than half of patients in the intervention arm, despite rates of successful revascularization > 70% [36].
PICO question 7: “When counseling critically ill patients with AIS or their surrogates, should early neurological improvement (ENI) assessed 24 h following revascularization, or 24 h following admission for patients who are not candidates for revascularization, be considered a reliable predictor of good functional outcome assessed at 3 months or later?”.
Description of the predictor: Early (or rapid) neurological improvement (ENI), which is most commonly observed following successful revascularization but may also occur spontaneously, occurs in approximately 20–40% of patients with AIS [43, 75,
Comments (0)