Design and participants
In a cross-sectional study conducted from August to December 2023, 500 participants were enrolled using cluster sampling. Participants were selected from clients of health centers in Shiraz, the capital of Fars Province in southern Iran. Assuming a sample-to-material ratio of 1:10 to 1:20 [13, 14], and considering the selection of 20 to 30 samples from each cluster (averaging 25 samples) across the 20 studied clusters [15], the approximate number of samples was estimated to be 500. The target population included adults aged 18 years and older who provided informed consent and visited the health centers in Shiraz. Data were collected using a self-administered questionnaire that comprised four sections: demographic characteristics, the Persian version of the OHVS, the Persian version of the Oral Health Impact Profile (OHIP-14) and The Health Literacy in Dentistry Questionnaire (HeLD-14).
Instruments
The sociodemographic characteristics recorded included age, sex, educational level (illiterate, elementary to middle school, high school to diploma, university graduate), occupational status (student, employed, unemployed, or retired), and place of residence (urban or suburban).
Oral health values scale questionnaire
The original Oral Health Values Scale (OHVS) questionnaire quantitatively evaluates the significance that an individual attributes to oral health. This instrument consists of 12 items and is systematically organized into four distinct subscales that examine pertinent domains of Oral Health Values: professional dental care (items 4, 8, and 11); esthetic appearance and health (items 3, 7, and 12); flossing practices (items 2, 5, and 10); and the maintenance of natural dentition (items 1, 6, and 9). Each item was assessed using a 5-point Likert scale, which was defined as follows: 1 = “Strongly disagree,” 2 = “Disagree,” 3 = “Neutral,” 4 = “Agree,” and 5 = “Strongly agree”. The aggregate score was derived by summing the responses for the Oral Health Value Scale (OHVS) items, implementing reverse scoring for items 2, 4, 6, 8, 9, and 11 in accordance with established guidelines for the construction of psychometric scales [8]. In the Persian version of the Oral Health Values Questionnaire, all questions were answered with a positive theme. To improve the evaluation of the requested items and the respondents’ understanding of the questions, the Likert scale scoring method was modified as follows: 1 = “Strongly disagree,” 2 = “Disagree,” 3 = “have no opinion,” 4 = “Agree,” and 5 = “Strongly agree”. In addition, the questions related to each factor were organized and categorized in order (Appendix).
Oral Health Impact Profile (OHIP-14)
The Oral Health Impact Profile (OHIP) questionnaire is a tool designed to assess individuals’ perceptions of the social impact of oral and dental disorders on their quality of life, with a particular focus on the impact on oral health-related quality of life. The questionnaire comprises 14 items that are answered on a 5-point Likert scale, ranging from 0 (never) to 4 (very often). The questionnaire was divided into seven dimensions: pain, psychological distress, physical disability, psychological disability, social disability, and disability. Each dimension includes two items that address functional and physical limitations. The internal consistency of the total score is highlighted in different cultural models. The Persian version has adequate psychometric properties [16].
Health Literacy in Dentistry Questionnaire (HeLD-14)
The Health Literacy in Dentistry Questionnaire (HeLD-14) is an instrument designed to assess an individual’s health literacy specifically in the field of dental care. This study consists of 14 items that assess various aspects of health literacy, such as understanding, accessing, and using dental health information, and the questions are in the form of a 5-point Likert scale. Scores were calculated by assigning 0 to the “no problem” response and 4 to “I cannot do this”. The scores ranged from 0 to 56, with higher values indicating lower oral health literacy. The validity and reliability of the Persian version of the questionnaire were well documented [17].
Assessing the suitability of an implementation tool
In the preliminary phase, the applicability of the OHVS questionnaire in assessing oral health values within the context of Iranian culture must be evaluated. Accordingly, a panel was convened, consisting of two dental specialists with expertise in medical education and two community dental specialists, to review and approve the suitability of the questionnaire. The panel deliberated on two questions concerning the appropriateness of the OHVS items for use in the Iranian population:
Do the values assessed in the OVHS questionnaire align with the oral health culture of the Iranian society?
Second, it is important to determine whether behaviors associated with oral health values should be included in the OHVS questionnaire [18].
Semantic equivalence
The next step involved creating a pre-final version of the Persian OHVS that was both conceptually and semantically equivalent to the original English OHVS. The semantic equivalence between the versions was assessed to evaluate the similarity in meaning and usage of terms, following the four steps proposed by Guillemin, Bombardier and Beaton (1993) [19]:
First, the OVHS questionnaire was translated into Persian using a rigorous back-translation process. For this purpose, two bilingual native Persian speakers translated the OVHS into Persian independently.
The resulting Persian translations were subsequently reviewed by a team of four subject-matter experts to consolidate them into a cohesive Persian version. A back-to-back translation of this Persian version into English was then conducted by two additional bilingual translators who produced two independent translations. The translations were discussed with the researchers to create the final English version. The expert committee reviewed the translations and ultimately approved the pre-final Persian OHVS, noting that no major or significant changes were recommended.
Operational equivalenceFace validity
To evaluate qualitative face validity, the Persian version of the OVHS was distributed to 12 dental specialists from the Faculty of Dentistry at the Shiraz University of Medical Sciences. They were asked to assess the items based on three criteria: difficulty (the challenge of understanding words and sentences), relevance (the relationship of items to the dimensions of the questionnaire), and ambiguity (the likelihood of misinterpretation of sentences or unclear meanings of words). After qualitative face validity was evaluated, the defective items were revised. Dental specialists were also asked to employ the item impact method to assess quantitative face validity and determine the significance of the items. For this purpose, participants rated each item on a 5-point Likert scale: (5 = very important; 4 = important; 3 = fairly important; 2 = not very important; and 1 = not at all important). Finally, all questionnaires were collected and analyzed, with impact scores above 1.5 deemed acceptable [20].
Content validity
The content validity of the instrument was evaluated using both qualitative and quantitative methods. In the qualitative assessment, twelve dental professionals were invited to rate items based on their necessity, importance, relevance, and overall evaluation. Additionally, in the quantitative assessment, metrics such as the Content Validity Ratio (CVR), Content Validity Index (CVI), and the Scale-level Content Validity Index (S-CVI/Ave) were calculated. The CVR was determined by the same group of dental professionals using a 3-point Likert scale, where items were classified as essential, useful but not essential, or unnecessary. Items with a CVR of 0.49 or higher were deemed suitable for retention. [21–22]. Furthermore, the relevance, clarity, and simplicity of each item were evaluated by dental professionals using a 4-point Likert scale to derive the CVI. The S-CVI/Ave was subsequently calculated based on the average CVI score across all items, with an S-CVI/Ave score of 0.90 or higher considered acceptable [23].
Reliability test
To assess the reliability of the questionnaire, two methods were employed. Cronbach’s alpha was used to measure internal consistency [24], while stability was evaluated using test-retest correlation methods with a two-week interval in a sample of 50 participants (10% of the total sample size) [25–26]. Additionally, the Intraclass Correlation Coefficient (ICC) test was utilized [27].
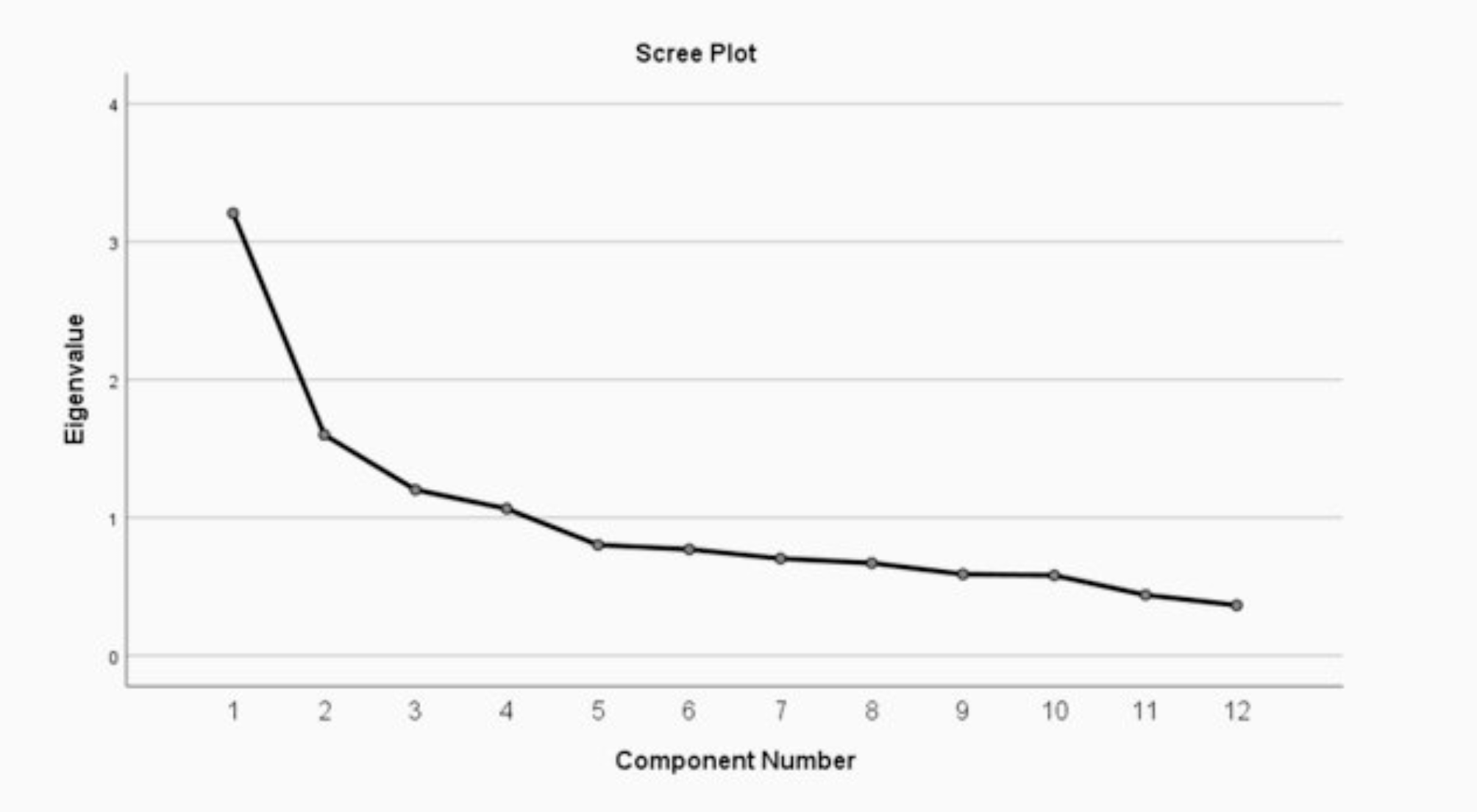
Exploratory factor analysis and internal consistency
To assess the structural validity, we employed factor analysis to examine the internal consistency of the questionnaire statements and identify variables Kaiser-Meyer-Olkin (KMO) sampling adequacy test was used to evaluate the suitability of the sample, along with Bartlett’s test of sphericity (BTS) to determine whether factor analysis based on the studied matrix is justified and appropriate. Additionally, we used principal component analysis, a scree plot, and varimax rotation. A minimum factor loading of 0.40 was deemed necessary to retain each item in the extracted factors from the factor analysis [28].




Comments (0)