
Remember me
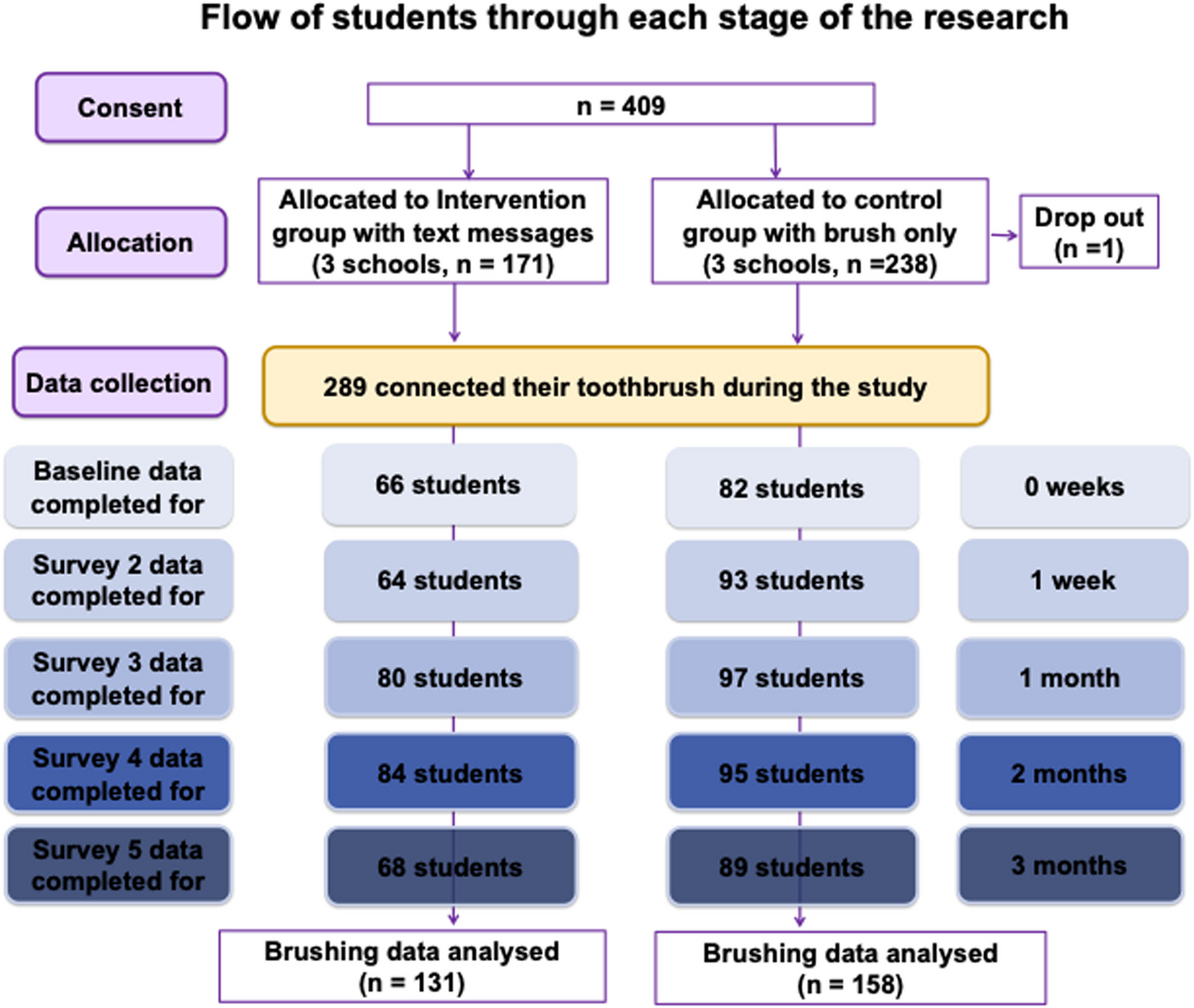
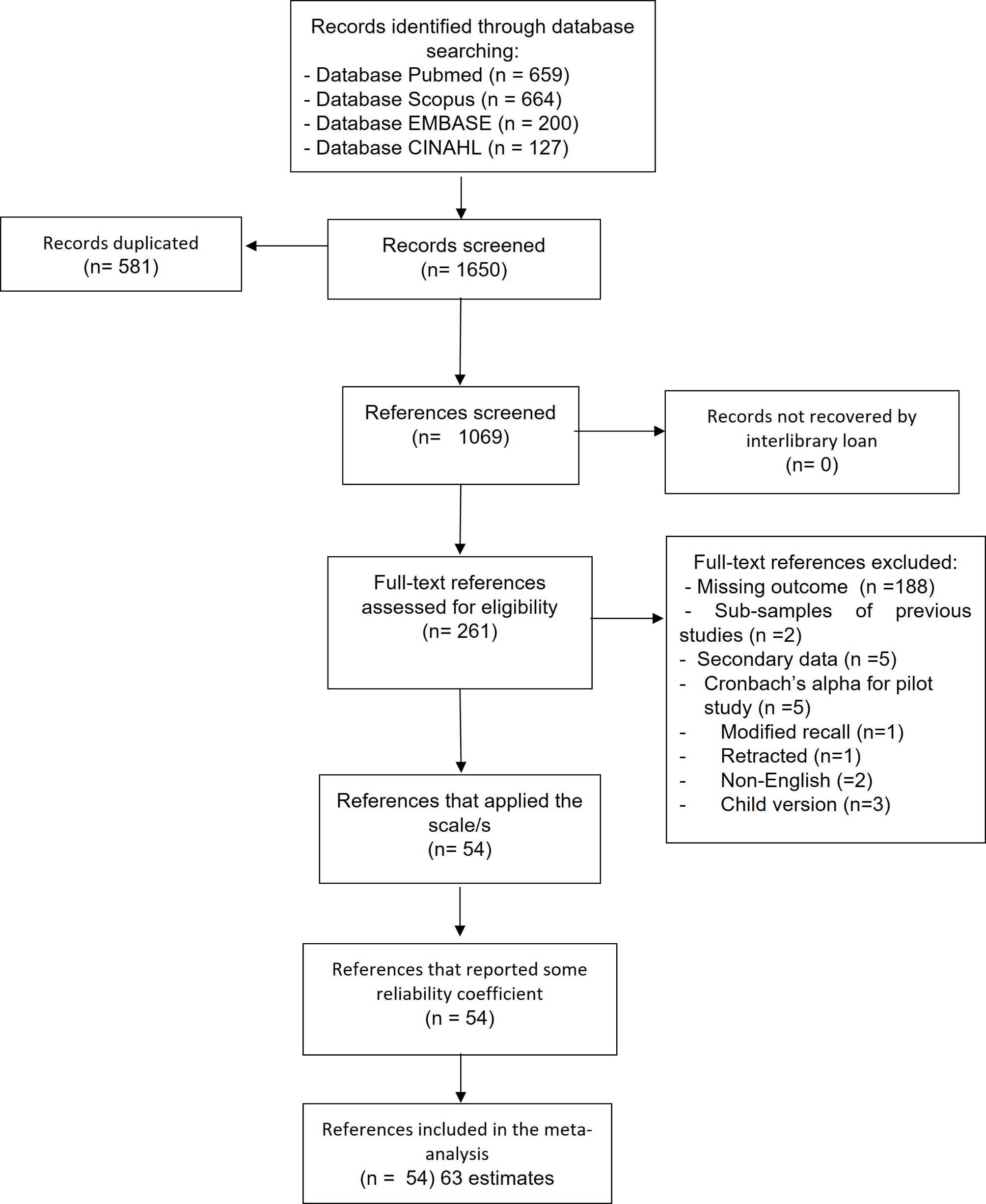



Six schools across underserved areas of Manchester were identified and approached to participate in the study. All consented and were randomised to the brush and app trial arm or brush, app and text message arm. Of 753 eligible children, 409 (54.3%) participants consented to take part in the study. Out of those, 171 (41.80% of total participants) in three schools were allocated to the intervention group with the text messages. Out of 409 consented participants, 148 completed baseline measurements, 157 1-week follow-up measurements, 177 1-month follow-up measurements, 179 2-month follow-up measurements, 157 3-month follow-up measurements. Figure 1 provides an overview of participants flow.
Fig. 1
Among the 148 participants who completed baseline surveys, the mean age of parents was 39.8 (SD5.94) while the mean age of children was 9.7 years (SD 1.6). In total, 121 mothers and 27 fathers completed baseline surveys. The majority of parents was of white ethnic background (N = 70, 47.9% of total sample), followed by Asian/British-Asian ethnic groups (N = 38, 26% of total sample), 8.9% (or N = 13) participants were of Black/Black-British/Caribbean ethnic group while 25 participants (17.1%) were of multiple ethnic or other ethnic groups. The majority of parents had full English competency (speak, read, write) (N = 120, 81.6%) with 27 participants reporting English fluency in one or more domains (speak, read or write). Most parents were in full-time employment (N = 74, 50%), with some working part-time (N = 39, 26.4%), others being stay at home parents (N = 14, 9.5%), 10 parents were unemployed (6.8%), 4 were students (2.7%), 1 retired (< 1%) and 6 preferred not to provide their occupation (4.1%). Finally, most parents and children came from households in the most deprived decile based on their Index of Multiple Deprivation (IMD) [21] scores with 77 households (52.4%) identified as decile1 (most deprived). In total, 50 households (34%) came from the second most deprived decile (score of 2), 11 (7.5%) from the 3rd most deprived decline (score of 3) while no household in the study came from deciles over 5. The overall composition of our sample closely reflects that of key areas of higher disease prevalence across the city and the country as a whole. With dental disease prevalence reducing generally, pockets of disease remain in areas of higher deprivation which as the ones targeted by our research.
Out of 20 participants who completed the follow-up, feedback, qualitative interviews, 18 (90%) were female with 17 participants (85%) from the most deprived deciles (1 and 2). There was an equal split in terms of ethnicity with 50% of participants identifying as White.
Feasibility outcomesIn terms of primary outcomes, out of 753 eligible participants across all 6 schools, 409 were consented (54.3% consent rate) with 148 participants completing baseline measurements (38.6%) as summarised in Fig. 1. Consent rates differed between participating schools with some recruiting as many as 67.8% of all eligible students while others consented around 42% of eligible students. Schools that hosted morning information sessions for parents did recruit more participants (mean 64.3 (SD4.95)) when compared to schools who did not host information sessions (mean47.0 (SD5.82)) (t(4) = 3.54, p = 0.023). The biggest reason for participants not completing their online baseline measurements was email addresses not working resulting in emails bouncing back (50 addresses not responding out of 409, 12% of consented participants). During the study, there was only 1 drop out due to inability to commit to study time commitments. All schools who participated in the survey were first-time research sites for similar research work with a very strong relationship developing between the research team, MCC OHIT and participating schools paving the way for future involvement in studies. Overall, an average of 164 participants provided data throughout the 5 follow-up points in the study reflecting 40.1% of all consented participants.
In terms of acceptability, parents found the study very enjoyable (average score of 8.9/10 in follow-up surveys), parents found the brush and app easy to use (average score of 8.7/10 in follow-up surveys). Parents of children in schools allocated to receive text messages also found them easy to understand and useful (average score of 8.9/10 in follow-up surveys) and finally, from the entire sample, most parents (N = 142, 91.6% of those completing feedback surveys) would recommend the brush and the intervention to family and friends.
Based on teacher’s feedback (provided through brief feedback surveys at the end of the study), they felt extremely valued and highly positive towards the intervention, specifically the use of the connected brush, app and the class performance tables. Teachers appreciated being part of this intervention and recognised the value of oral health for their students. Teachers reported some issues around connectivity in line with comments from parents. These issues seem to have caused some struggles for some students.
“…some students struggled to sync, it wasn’t that clear, we asked them to read the guidelines, but some still struggled…” (T3)
“…some students lost the information we provided, as it happens, so maybe circulating the information more often couId have been better…” (T4)
The overall time commitments required by teachers was not an issue for all of them and teachers also valued the deployment of the dashboard to help motivate classes to reach higher goals in their brushing frequency, coverage and duration. Also, some teachers found the use of a connected brush useful beyond the scope of the study by incorporating information from the brush into their lessons.
“(the) brush has helped with teaching students personal hygiene, I am big on personal hygiene and I’ve used the brush as a good prop to help students take care of their teeth” (T2)
Barriers & facilitators to adopting the connected brushThree key facilitators were uncovered during analyses of follow-up, feedback interviews with parents, namely: (a) enhancing children’s self-reliance, (b) increased engagement using visual cues and (c) increased motivation due to gamification.
(a)Developed adolescent children’s self-reliance in dental care
Most participants found the connected brush and app intervention helpful, primarily because it fostered self-reliance and responsibility in children. Children were taking responsibility of the device and their oral hygiene, and there was a shift in parental supervision to remote monitoring. Some reasons reported by the parents for the high engagement from children include the device’s novelty, gamification features (tracking brushing scores and immediate visual feedback through the app), and ease of use. Behavioural changes include children taking ownership of their routine, demonstrating responsibility by remembering essentials like chargers while traveling, and feeling more grown-up and independent.
“So… she was really, really keen on making sure she was on track with it, and even when we’ve gone on holiday for a weekend, she wanted to make sure that she took her charger for the toothbrush and stuff. It gave her a really good sense of independence…. I think it made her feel a bit more grown up.”—Participant 14
“So yes, it was quite useful on both sides, to be honest, for both me and for her, a little bit more enthusiasm, you know, a bit of a gadget to play with, a little bit of enthusiasm for her to brush her teeth properly. So that was quite nice. I think for me it was interesting to see how she’d been doing, and to also encourage her to pay attention to what she does when she brushes her teeth, yes.” – Participant 19
(b)Visual cues increase engagement and promote interactivity
Several participants mentioned the app provided clear, interactive and visually engaging cues that facilitated proper brushing, particularly providing real-time feedback. Parents said that visualising areas that the children were typically missing during routine toothbrushing or using visual cues to brush for a full two minutes both improved children’s toothbrushing. Visualizing their children’s toothbrushing was also helpful for parents. It improved their awareness as not all parents were aware of “how” to brush properly. It served as a useful tool for parental oversight as children grew independent while allowing parents to stay involved.
“I think, me personally, I think that app and things, it gets the parent involved as well to make sure that they’re doing it, rather than being in school and, this is how you brush your teeth, type of thing. Because at least you can be both there watching the app and making sure that she doesn’t have any food or drink afterwards and things like that. I think, personally, something like that is a lot better than them just being taught in school.” Participant 15.
It allowed parents to remotely monitor their child’s brushing, and helped build trust and accountability between the parent and child.
“It broke my heart because she said that they had to take about eight teeth out…and she can't lie to me and say, yeah, I've done it. No you haven’t. So I thought that’s really good, and I'd recommend it to other people because I think it's brilliant.” (Participant 18).
Visualizing the child’s brushing habits was also helpful for parents who felt “judged” by dental staff and felt their word was not taken seriously:
“…I think they think that she’s not cleaning her teeth, which was quite good because I could then show the dentist the app and say, look, she is, it's here, here’s the proof…” (Participant 18)
(c)Gamification and competition increase motivation in children
Gamification and goal-setting features which allowed children and parents to track progress, converted toothbrushing into a rewarding activity. Incorporating elements of play and achievement seemed to help children stay motivated. The sense of achievement kept children interested and motivated, and several children felt proud of it, reflected by them telling others about it, such as their dentist and cousins. Other features that kept children motivated were the novelty of the device, as most children had not used an electric toothbrush before. They were also motivated by competing against their siblings and other children at school.
“Yeah. Well, the app does show, it shows points to show how much you’ve done. So, my children they keep tabs on each other. So X was saying to Y, ‘oh look, I have so many’. Y, I think when he missed it once or twice, so he had lesser points. So then between themselves, they kept feeling, like, ‘oh she has more, so I should quickly get mine up as well’ Participant 10.
“I am not 100 per cent sure, but I think when they were doing the three-month monitoring of it I feel like they did something at school as well. So that encouraged a lot of the other children because it became…they wanted to [set 15:27] the points, they wanted…it became more competitive, but in a nice way.” Participant 4
Meanwhile, two key barriers ((a) unavailability of device to use the connected brush and (b) issues around safety and sustainability) were uncovered during analyses.
(a)Unavailability of device due to circumstance or preference
The availability of the phone or tablet to use the app was a major barrier. Most children were either using the app on their parent’s devices or their own tablets, which made regular app usage complicated particularly in the mornings, which tend to be busy for both parents and children. In addition, parents had concerns about children’s screen time, which tends to be a particular problem for adolescents.
“No, because obviously it’s on my phone and I work sometimes and it’s more difficult. It wasn't connected to anything else, just my phone. So in the morning, am I rushed getting to work or am I not in work, it depends. So that time I was very…I was always getting late so I'm like, you know what, I'm just deleting it from my app, just do it on your own accord.” (Participant 13)
“Do you know, I will say this one thing though, so the thing is with the app, we didn’t use it as much, ‘cause I’m trying to get my nine year old to not stay in the tablet, and when we take the tablet away from her, she’ll just [inaudible 00:19:42] phone, which I use, [to separate 00:19:45] my personal phone and the work phone, and she’ll just take my work phone and use that. So this is a bit of a challenge as well, I think from your point of view, if some parents don’t want to give their kids technology at that age, you know, ‘cause of the fear of social media and all that kind of stuff, and just sitting on a tablet mindlessly playing games, which is just brain dead.”
“We don’t really want to give her the phone, ‘cause she’ll use the phone for the app, and then she’ll just play a game with it later on.“ Participant 5
(b)Safety and sustainability concerns
There were other safety concerns that could have been addressed through detailed information leaflets and may have affected the reduced participation within the program. One participant mentioned other parents’ concerns about being “tracked” through the app.
“But when this program was happening in my school, I remember people’s feelings, I remember it quite well. But mine were quite good. They were a bit scared that ‘oh, they’re going to control us through the device, they’re going to monitor us’. That was funny because I received phone calls. So children whose mothers couldn’t speak proper English, they called me, that you know, now they’re going to be monitored all the time. I told them no, they’ll just be able to see if they’re brushing their teeth. ‘No, that’s not right, they’ll be monitoring us’.” (Participant 10)
Other concerns included the safety of electric toothbrushes in this age group and environmental concerns about the use of plastic, particularly due to the unavailability of reusable heads.
“I guess I had asked our dentist what he thought about electric toothbrushes, and whether they were too abrasive for children or anything like that. So there must have therefore somewhere in the back of my mind being a bit of apprehension. But I think overall I was like, I thought it was a good thing.” (Participant 11)
“…then came home with a plastic toothbrush, which we try and recycle. So it’s things like that that annoy me.” Participant 7
Comments (0)