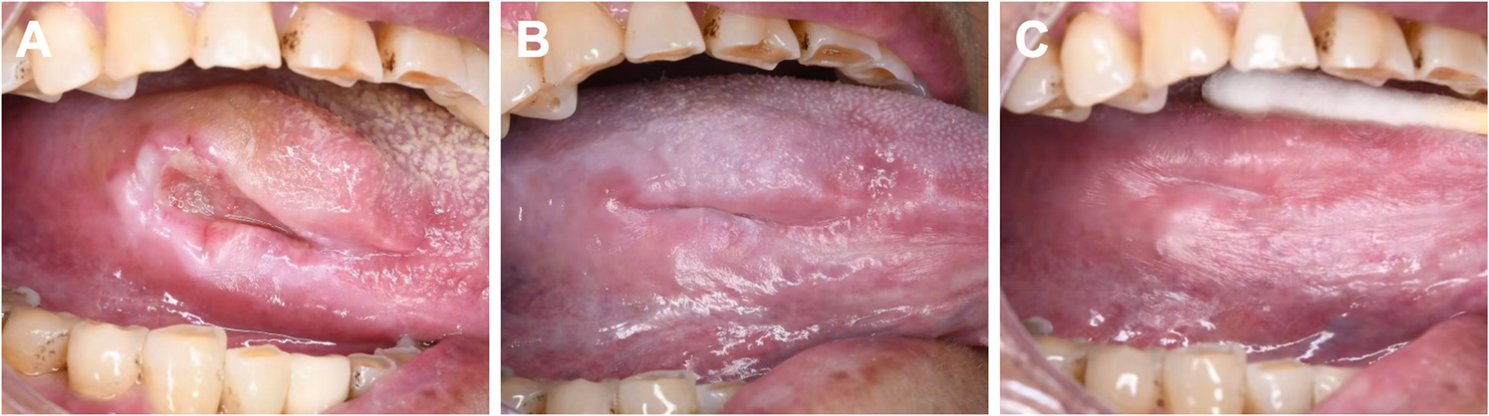
Ulcers that do not heal for a long time in the mouth have a risk of cancer, especially those located in high-risk areas such as lingual border. They need to be differentiated from oral cancer, and pathology is the gold standard for differentiation. PG is usually difficult to differentiate from oral malignancy when ulceration is present on the surface for a long time. As a limited lesion, PG usually has clear borders and regular shape. Because it is composed of mainly neoplastic capillaries and endothelial cells, it is relatively soft in texture and bleeds easily upon irritation [14]. Oral cancer, on the other hand, will become slightly harder in texture as the cancer cells proliferate and infiltrate the surrounding tissues [10]. The reason for the tougher texture of the PG in this case may be due to the fact that after repeated mechanical stimulation, the tissue is repeatedly in the process of injury and repair, resulting in a proliferative buildup of the fibrous tissues involved, which may be the reason for the lack of significant bleeding of the PG under prolonged sharp-tip stimulation in this case. PG is usually bright red or dark red due to its abundant capillaries. In oral malignant tumors, the tumor cells grow fast, And local tissue necrosis occurs due to insufficient blood supply on the surface of the mass and appears grayish-white. Oral cancer is mostly OSCC. Notably, this female patient presented with a painful ulcerative mass on the tongue interfering with mastication, which had persisted for five years. However, the tongue remained fully mobile, and physical examination revealed no enlarged cervical lymph nodes. These clinical findings are less suggestive of malignancy. OSCC in high-risk sites such as the lateral tongue border typically exhibits aggressive behavior. A study of 171 patients with early-stage tongue OSCC reported lymph node metastasis in 40 cases (23.4%) [15]. Ahmed SQ et al. reported in their study of 78 early-stage tongue OSCC patients that cervical lymph node metastasis occurred in 69% of cases with tumor thickness > 5 mm, whereas no metastasis was observed in patients with tumors < 5 mm in thickness [16]. Pathologically, PG consists of lobular proliferative granulation tissue forming a rich vascular network, infiltration of scattered inflammatory cells, and an increased fibrin layer within the epithelium is seen within lesions that have ulcerated [17]. In contrast, disorganized squamous epithelial cells with varying degrees of differentiation and significant cellular anisotropy can be observed in OSCC. Certain PGs share similar clinical manifestations with OSCC, so histopathologic examination is important in determining the nature of both.
PG is often caused by traumatic injury, inflammation, hormonal changes, or medications [14]. This patient had sharp dental cusps in the lesion counterpart, which may have been the most important factor contributing to this patient’s tongue PG. Physical friction or chemical irritation causes the release of a variety of endogenous substances and angiogenic factors in the corresponding areas of the oral mucosa resulting in a disturbed vascular distribution in the lesion area [18]. Therefore, we speculate that long-term and sustained sharp cusps stimulation can keep tongue lesions in an inflammatory state for a long time, breaking the normal damage/repair mechanism. This sustained inflammatory environment will continuously release growth factors in local tissues, which will further stimulate the growth of blood vessels and fibrous tissues. A study by Yuan et al. found that several important angiomorphogenetic factors have higher levels in PG than in normal tissues, suggesting that PG may result from an imbalance between these angiomorphogenetic factors [19]. Therefore, we immediately regulated the grinding of the sharp cusps of the teeth as soon as this risk factor was detected.
In this case, the patient was at an older age and we hypothesized that the PG might also be related to its altered estrogen secretion levels. At this stage, ovarian function declines, resulting in a significant decrease in estrogen. Estrogen has an important protective effect on the oral mucosa, and under normal conditions, estrogen promotes the proliferation and differentiation of oral mucosal cells and maintains the thickness and elasticity of the mucosa. With decreased estrogen, the self-repairing ability of the oral mucosa decreases [20]. Therefore, when the oral mucosa is damaged, the repair process may be abnormal and tend to trigger an inflammatory response, which can increase the risk of PG. However, PG is more common in women during pregnancy, when the level of estrogen secretion increases significantly. Existing studies suggest that the increase in estrogen may have an effect on the microcirculatory system, stimulating angiogenic factor production, increased vascular permeability, and vascular proliferation, which may trigger PG [17, 21]. Therefore, whether lack of estrogen in women can trigger or induce PG still requires further study.
This woman has been taking antidepressants for a long time, and the main antidepressants currently in use are Selective Serotonin Reuptake Inhibitors (SSRIs), and there have been no reports of antidepressant-induced PG in the literature. But some scholars have also discovered drug-related PG, and carbamazepine may stimulate the release of angiogenic factors through inflammatory processes [22]. Levothyroxine, through its promotion of angiogenesis and proliferation, may be a possible cause of PG occurrence [23]. The use of SSRIs can lead to an increase in inflammatory markers in vivo, and cytokine expression levels of Tumor Necrosis Factor-α (TNF-α) and Interferon-γ (IFN-γ) were increased in depressed patients taking SSRIs [24]. We hypothesized that the patient’s use of antidepressants may lead to altered levels of some of these inflammatory factors, which in turn affects the permeability of the vascular endothelium, which may act as a trigger for the production of PG.
This patient has a history of gastric carcinoma, which increases the incidence of oral cancer. On the other hand, the patient had also undergone a partial gastrointestinal resection, which is associated with impaired absorption of nutrients, and the intake of some nutrients plays an important role in maintaining the integrity and function of the oral mucosa. For example, vitamin B12 deficiency interferes with the normal metabolism and repair of the oral mucosa [25]. In addition, there is a close correlation between the microbial communities of the gastrointestinal tract and the oral cavity [26]. Gastrointestinal resection surgery disrupts the gastrointestinal microbiotal community, which in turn has a certain impact on the oral microbial community. The imbalance of oral microbiota makes patients more susceptible to inflammatory responses after local stimulation.
Oral PG is prone to recurrence, with a recurrence rate of 15%. The recurrence rate of PG in the gingiva is much higher than that in other parts of the oral mucosa [27]. Given the high recurrence risk associated with PG, long-term surveillance remains imperative. Although the 6-month and 1-year telephone follow-up confirmed no recurrence, this approach has inherent limitations: inability to visually inspect the lesion site; absence of palpation for submucosal changes; and potential bias in patient self-reported symptoms.
The conventional treatment is surgical resection, and minimally invasive treatments include laser, corticosteroid injections, cryotherapy, and sclerotherapy [28]. After the patient was identified as a PG, we administered a mixture of triamcinolone acetonide acetate and lidocaine hydrochloride to the patient for local multipoint injection. Considering the patient’s poor tolerance, performing non-surgical treatment can avoid secondary incisions in the short-term period after the patient’s biopsy and also reduce the trauma during surgery. Mixing with lidocaine hydrochloride in equal proportions reduces the concentration of triamcinolone acetonide while simultaneously alleviating injection site pain. As a corticosteroid, triamcinolone inhibits the production of key inflammatory mediators—including prostaglandins, leukotrienes, and cytokines—and significantly decreases vascular permeability [29]. Corticosteroids were found to reduce vascular endothelial growth factor (VEGF) expression and angiogenic potential, which may account for the effective treatment of oral PG with corticosteroids [30]. Parisi et al. reported for the first time the use of corticosteroids for the treatment of oral PG. They administered four times injections over 9 weeks to a patient with PG accompanied by satellite lesions, and observed improvement in the lesions at each visit [31]. Amr Bugshan et al. injected corticosteroids into five different sites of palatal PG lesions in conjunction with topical application of 0.05% clobetasol propionate ointment for 2 weeks, And the lesions had completely disappeared at the 3-week follow-up [32]. Additionally, adjunctive wet compress application of triamcinolone acetonide enhances the local anti-inflammatory effects of corticosteroid therapy.
The ulcerated surface of the patient’s PG lesion is highly susceptible to colonization and infection by abundant oral bacteria. These microorganisms and their metabolites act as potent inflammatory stimuli, exacerbating local inflammatory responses. The compound chlorhexidine gargle contains both chlorhexidine and metronidazole. As a cationic agent, chlorhexidine electrostatically binds to anionic bacterial cell walls, disrupting membrane permeability and inducing bacterial death through leakage of intracellular components [33]. Metronidazole’s nitro group undergoes anaerobic reduction to cytotoxic intermediates that disrupt bacterial DNA structure and inhibit nucleic acid synthesis, culminating in cell death. Cetylpyridinium chloride, a quaternary ammonium cationic surfactant, exerts antimicrobial effects via electrostatic adsorption of its cationic moieties to anionic microbial membranes. This competitive displacement disrupts membrane integrity and induces lysis in bacteria and fungi [34]. Compound chlorhexidine gargle or cetylpyridinium chloride mouthwashes facilitate ulcer healing in PGs by reducing local irritants and bacterial load, thereby optimizing the oral microenvironment for tissue repair.
Bovine bFGF gel contains a substantial amount of bFGF, a potent mitogen for fibroblasts and a significant angiogenic factor. At ulcer sites, it markedly stimulates the proliferation and migration of nearby fibroblasts and vascular endothelial cells into the wound, promoting tissue repair and healing [35]. However, in cancerous ulcers, bFGF can directly stimulate the proliferation of cancer cells, accelerating tumor growth and infiltration [36, 37]. We previously confirmed the absence of cancer cells through histopathological examination before utilizing bovine bFGF gel to promote ulcer healing.
In conclusion, this case highlights the need to differentiate ulcerative PGs from oral malignancies, prioritize the provision of non-surgical treatment options with a clear pathologic diagnosis is more acceptable for older patients, And provides insights for further clinical understanding of extragingival PGs. Despite relocation-related follow-up limitations, 1-year remission supports the efficacy. Long-term monitoring remains crucial, and future research can standardize remote assessment protocols for such cases.




Comments (0)