Symptomatic congenital pericardial agenesis is a rare clinical entity. Its symptoms are often nonspecific and overlap with other common conditions, making diagnosis challenging [7]. In our case, the patient presented with isolated chest pain, a common but nonspecific symptom, highlighting the subtlety with which this condition can manifest.
Congenital pericardial agenesis arises from a failure of the pleuropericardial membranes to fuse completely during the fifth week of gestation, resulting in the partial or complete absence of the pericardium [5]. This absence compromises the pericardium’s protective and supportive functions, increasing the risk of cardiac positional shifts within the thoracic cavity. Such displacement can place mechanical strain on the heart and great vessels, potentially leading to chest pain, especially during physical activity or changes in body position [8].
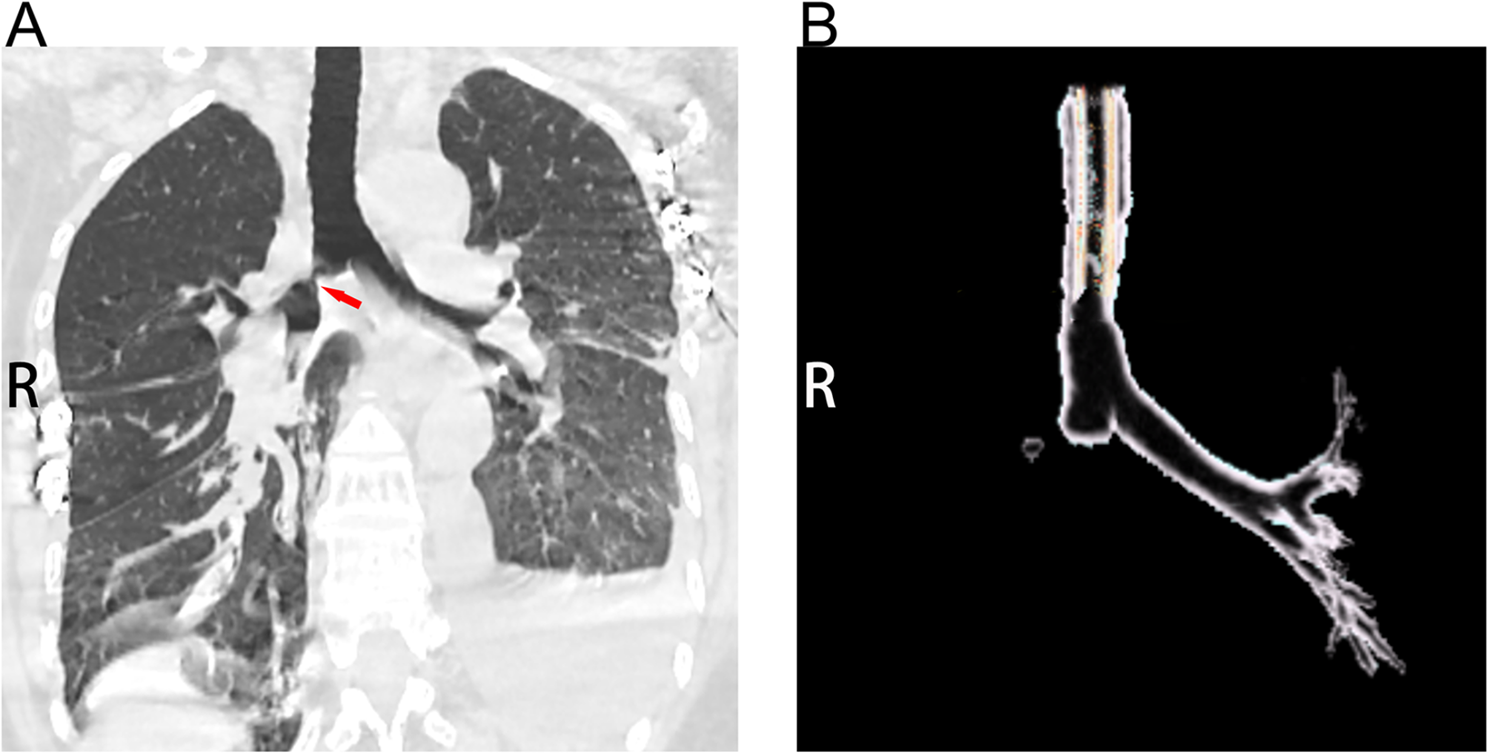
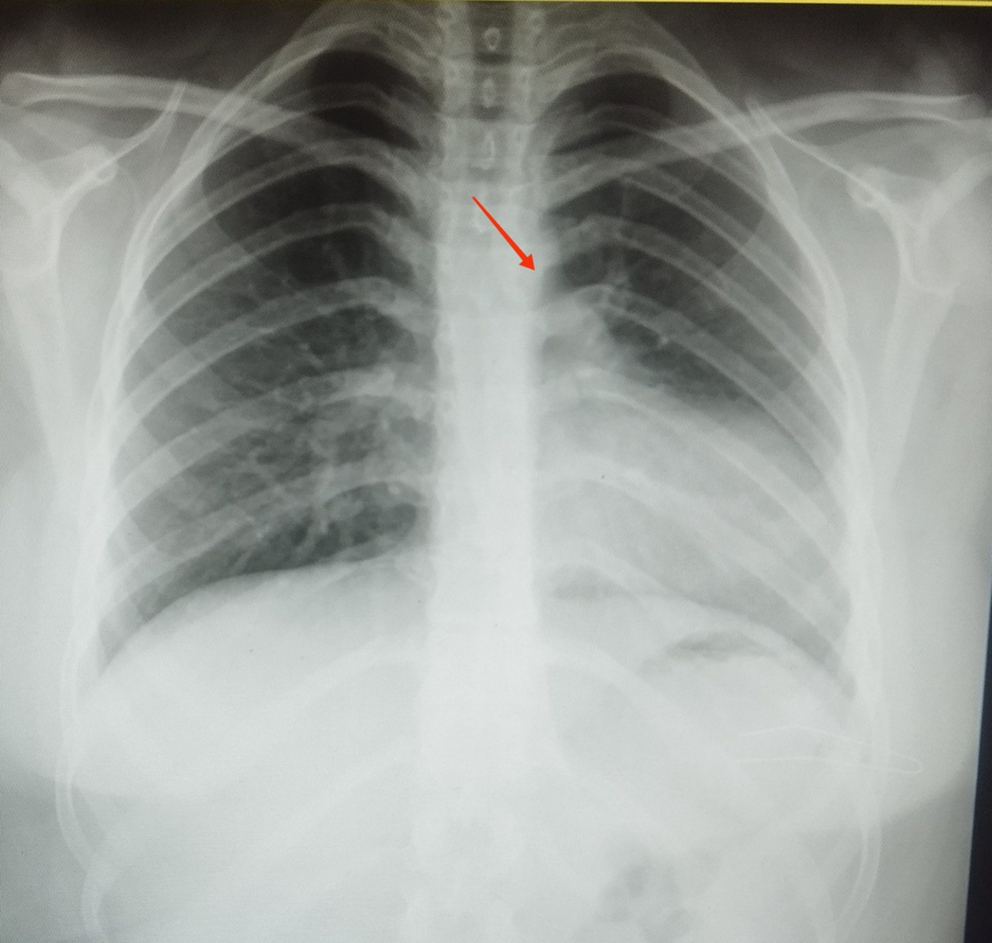
Patients with this condition often present with nonspecific symptoms such as chest pain, dyspnea, or palpitations, making diagnosis challenging. Imaging studies, including chest X-rays and CT scans, can reveal characteristic signs that help confirm the diagnosis of congenital pericardial agenesis [4, 9]. One such diagnostic clue is the ‘Snoopy sign,’ which indicates the complete absence of the left pericardium and is identified by the distinctive appearance of the cardiac silhouette on imaging [10]. According to the 2015 ESC Guidelines for diagnosing and managing pericardial diseases, multimodality imaging, including cardiac magnetic resonance (CMR) and echocardiography, is essential for a comprehensive evaluation and accurate diagnosis of pericardial conditions. These modalities confirm the diagnosis and assess the extent of the defect and its impact on cardiac function, guiding appropriate management strategies [11].
Management typically depends on the presence of symptoms; asymptomatic isolated agenesis usually requires no treatment. However, symptomatic patients, particularly those with the complete form of agenesis, may benefit from surgical intervention such as pericardioplasty to alleviate symptoms [1]. In cases of partial pericardial absence, surgery may be indicated to prevent complications such as herniation, type A aortic dissection, or coronary artery compression [6]. Partial pericardial defects can lead to serious complications, including cardiac herniation, which may result in critical conditions such as left atrial appendage strangulation or coronary artery compression, often requiring surgical intervention [5, 12]. Moreover, pericardial agenesis can precipitate significant complications like pericardial effusion or cardiac tamponade, both of which are potentially life-threatening and demand immediate diagnosis and management [11]. The prognosis of pericardial agenesis largely depends on the extent of the defect;
In contrast, complete agenesis typically has a benign course with a favorable outcome; partial agenesis carries a heightened risk of complications, necessitating closer monitoring and potential surgical intervention [1, 12]. Additionally, right ventricular enlargement and associated cardiac abnormalities in partial agenesis complicate the clinical course, underscoring the need for early and accurate diagnosis. The absence of the pericardium can cause excessive heart motion, leading to mechanical stress and increasing the risk of arrhythmias and other functional issues [13].
A study by Khayata et al. involving eight patients with congenital pericardial defects found that partial defects were more common on the left side and that right ventricular dilation was a frequent echocardiographic finding. The study also highlighted that most patients remained stable and asymptomatic during follow-up, with only one requiring surgical intervention. These findings underscore the variability in clinical outcomes, further emphasizing the need for individualized management strategies based on the extent of the pericardial defect and associated symptoms [14].
In a case report by Trimarchi et al., a 32-year-old man with complete left-sided pericardial agenesis was asymptomatic and had a good prognosis. The study emphasized that in asymptomatic cases of complete pericardial agenesis, no treatment is typically required, and a comprehensive diagnostic work-up with multimodality imaging plays a crucial role in preventing diagnostic errors and optimizing patient follow-up. However, the study also noted that partial pericardial defects are associated with a higher risk of complications, such as herniation and arrhythmias. It may require closer monitoring and, in some cases, surgical intervention [6].
In a case study by Kalekar et al., a 32-year-old male presented with chest discomfort and radiating pain that mimicked myocardial infarction. Multimodal imaging, including chest X-ray, echocardiography, and cardiac MRI, revealed complete left pericardial agenesis, characterized by significant leftward displacement of the heart. This case underscores the importance of considering pericardial agenesis in the differential diagnosis of chest pain, particularly when initial investigations are inconclusive, and highlights the critical role of advanced imaging techniques in diagnosing this rare condition [15].
The evidence summarized in the literature review table supports this approach. It compares clinical presentations, diagnostic methods, and management strategies across different studies (Table 2).
Table 2 Summary of Case reports on Pericardial Agenesis




Comments (0)