
Remember me



A 55-year-old female patient with no history of diabetes, hypertension, or coronary artery disease presented following a motor vehicle accident one month prior, which caused multiple rib fractures, hemopneumothorax, and scapular fractures. She initially underwent emergency surgery, including bilateral rib fracture reduction and fixation (L4-7, R6-7) and repair of a left lung lingular laceration, and was discharged two weeks later. However, five days before the current admission, she developed progressive dyspnea of unclear etiology and was admitted to a local hospital. Chest CT revealed right lung atelectasis, and the patient was intubated and placed on mechanical ventilation. She was subsequently transferred to our hospital for further management.On admission, physical examination revealed a collapsed right chest wall, reduced respiratory movement on the right side, and diminished breath sounds over the right lung. Chest CT showed increased density in the right lung, atelectasis, right-sided pleural effusion with blood, and left-sided pleural effusion with partial expansion defect (Fig. 1). The patient was on mechanical ventilation with 100% oxygen, and arterial blood gas analysis indicated a PaO2 of 67 mmHg, PaCO2 of 34 mmHg, and oxygen saturation of 88%. Despite this, no mediastinal emphysema was observed. Due to the inability to maintain oxygen saturation despite mechanical ventilation, a right main bronchus rupture was suspected, necessitating emergency surgery.
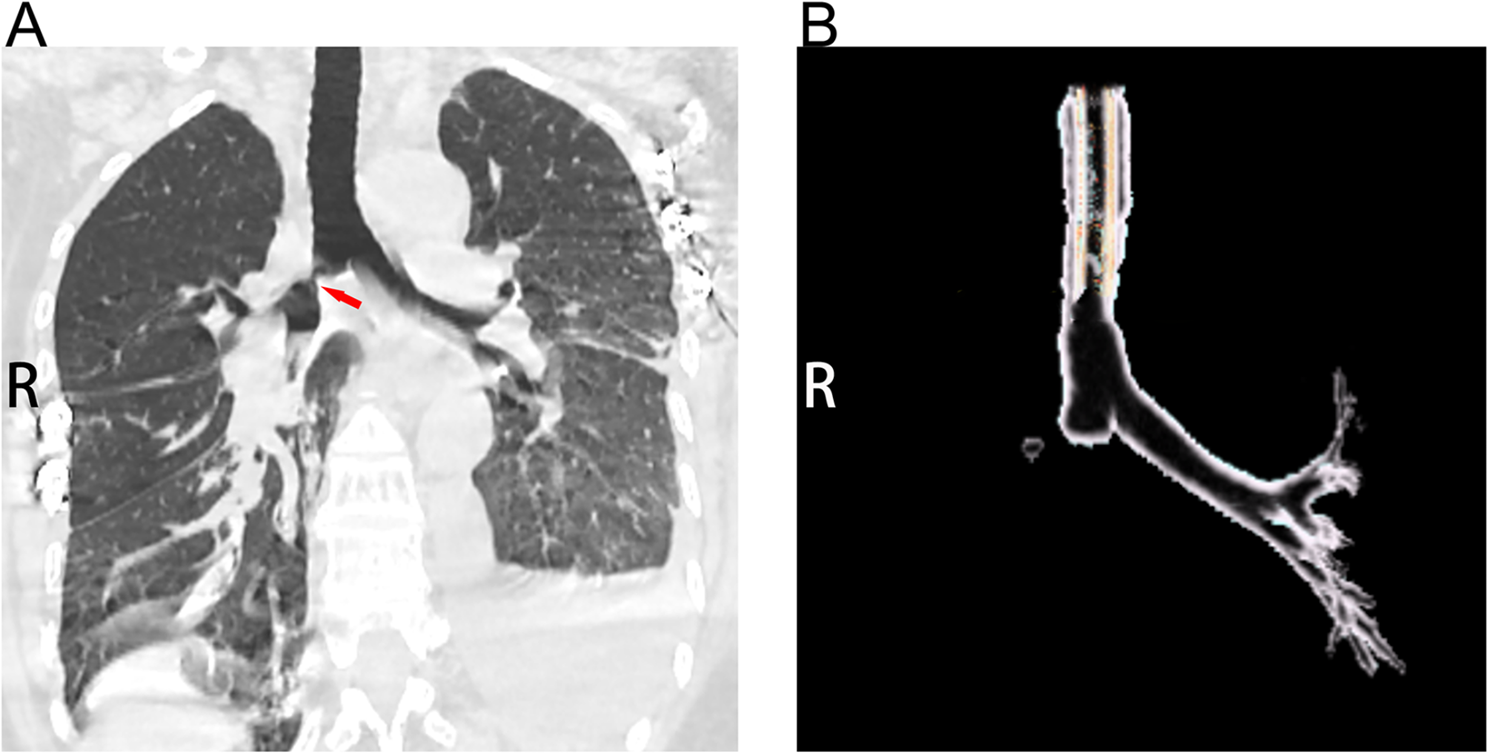
Fig. 1
Coronal CT scan and 3D reconstruction of tracheobronchial anatomy. (A) Coronal chest CT demonstrating significant pathological changes. The red arrow indicates a suspected tracheal lesion near the carina. The right lung (R) shows signs of collapse or atelectasis. (B) 3D reconstruction of the tracheobronchial tree highlighting the structural anatomy. The right bronchus (R) is not visualized, suggesting a possible rupture, consistent with the findings on the CT scan
Under ultrasound guidance, ECMO cannulas were inserted into the right femoral vein and right internal jugular vein for VV ECMO support. Following ECMO initiation, oxygen saturation increased to 100%. The patient was anesthetized, and a right-sided intercostal incision was made at the sixth rib space. Intraoperatively, extensive adhesions were found between the right lung and chest wall. After careful dissection, the right main bronchus was exposed. The innominate vein was found to be densely adherent to the bronchus and was clamped and divided. The right main bronchus was dissected free, and a bronchoscope was inserted to identify the site of obstruction approximately 1 cm from the carina. The bronchus was incised, revealing granulation tissue filling the lumen (Fig. 2). The obstructed segment was resected, and the bronchus was anastomosed with 3 − 0 Prolene sutures. Post-anastomosis bronchoscopy confirmed a complete and non-stenotic anastomosis. Extensive sputum suction and lavage of all lung segments were performed. After confirming no air leaks, hemostasis was achieved, a chest drain was placed, and the chest was closed in layers. The patient was extubated and weaned off ECMO, with stable vital signs and oxygen saturation of 100% on 60% oxygen supplementation.
Fig. 2
Intraoperative findings and gross pathology of the tracheobronchial lesion. (A) Intraoperative bronchoscopy showing the tracheal lesion with visible mucosal irregularities and narrowing, consistent with the suspected rupture. (B) Surgical field during the resection of the tracheal lesion, with white arrows indicating the location of the rupture. Careful dissection was performed to free and resect the affected area, followed by bronchial anastomosis. (C) Gross specimens of the resected tracheal segments, demonstrating severe damage and disruption of the tracheal wall, further supporting the diagnosis of tracheal rupture. The scale bar represents 1 cm
The patient was transferred to the ward with a tracheostomy, continued mechanical ventilation, and received prophylactic antibiotics, fluid resuscitation, and analgesia. The extubation was removed 17 h postoperatively, and respiratory care was intensified to promote coughing and sputum clearance to prevent pulmonary infection. Postoperative chest CT revealed linear and increased density shadows in both lungs, suggestive of resolving pulmonary contusion, and high-density shadows in the right hilum. Multiple rib fractures with post-fixation changes were also noted. On postoperative day 8, the patient’s vital signs were stable, with slightly coarse breath sounds and no significant rales or rhonchi, leading to discharge. A follow-up chest CT one month after discharge showed minimal pleural effusion, pleural thickening, adhesions, multiple rib fractures, and post-fixation changes, with no other abnormalities (Fig. 3).
Fig. 3
Postoperative CT findings and 3D reconstruction of the tracheobronchial tree. (A) Postoperative coronal chest CT showing resolution of the previously noted right lung atelectasis (R). The tracheobronchial anatomy appears restored, with no evidence of residual obstruction or rupture. (B) 3D reconstruction of the tracheobronchial tree illustrating the restored continuity and patency of the airway. The previously absent right bronchus (R) is now fully visualized, indicating successful surgical repair and anastomosis
Comments (0)