
Remember me



This study was approved by the local ethics committee (2016047X, Beijing Anzhen Hospital, Capital Medical University). This patient is a 51 years old male, whose information was collected on August 3, 2016 in Anzhen hospital. He has BAV with left/right cusp fusion and mild-stenosis as well as dilated AAo with diameter of 4.5 cm by echocardiography. We confirmed the patient doesn’t have a history of hypertension, hyperlipidemia, coarctation of aorta, aortic dissection or Marfan syndrome.
Aortic model reconstructionThe model of the aorta was established based on the MRI data (in-plane resolution of 512 by 512 pixels with a pixel size of 0.7 mm and slice thickness of 1.25 mm, total 600 images). This MRI was obtained by the Trio Tim 3.0 T MRI scanner of Siemens of Germany, with the maximum switching rate of 200 T/(ms) and the maximum gradient strength of 45mt/m under the phase-controlled front ring and the electrocardiography gated control scan. Image segmentation and surface reconstruction of the aorta from the BAV patient were accomplished by a semi-automatic threshold-based segmentation tool (Mimics17.0, Materialise Inc., Belgium).
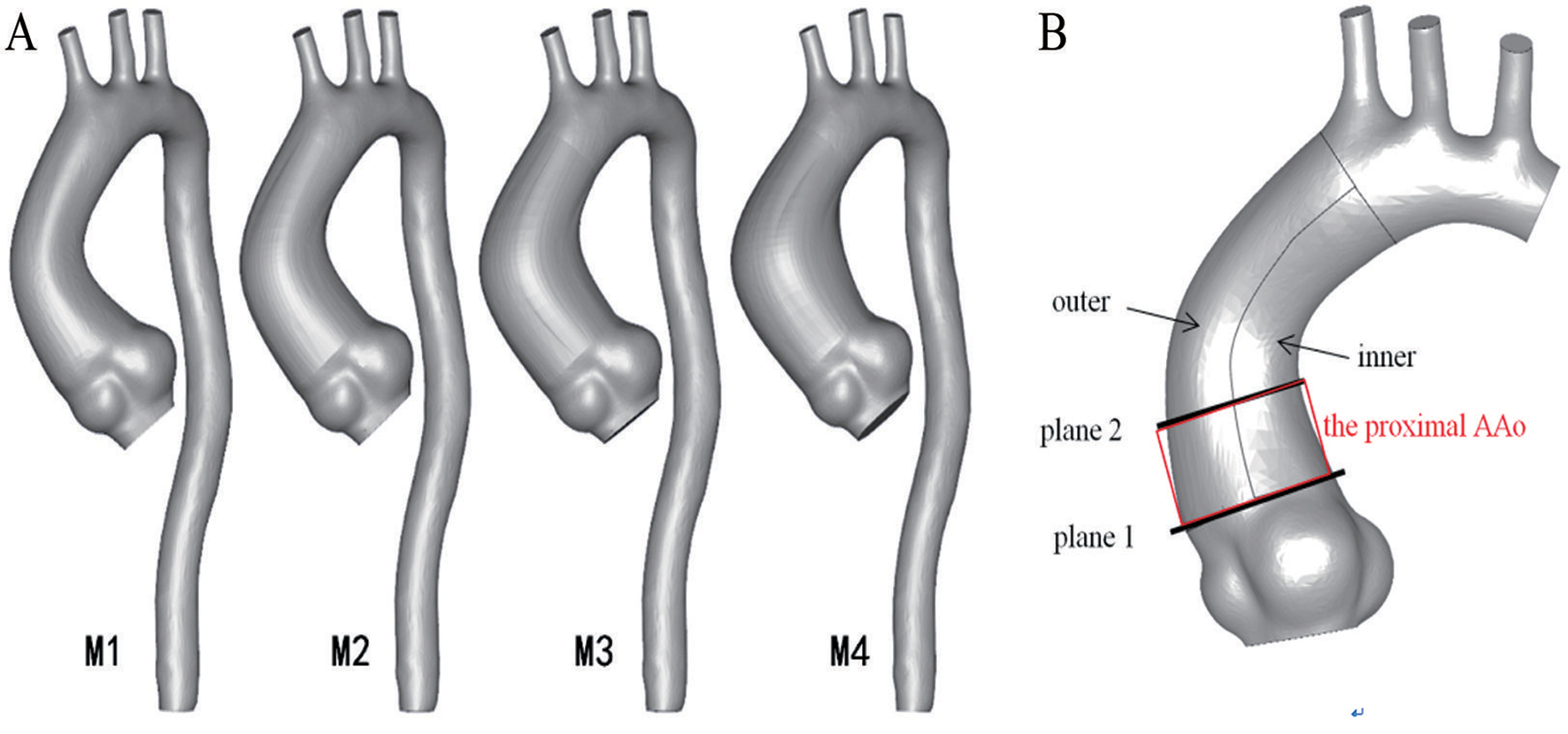
The model was smoothed after surface reconstruction. The format of the aorta model was subsequently saved as X_T format (a kind of parasolid model file format) from stereolithography by extracting surface function (Geomagic Wrap2015, Geomagic Inc., USA). Starting from the sinotubular junction to the end of the AAo, the aorta model was cut off at the region of maximum diameter. The profile of the cross-section at the maximum diameter of the AAo was traced, and the diameter of the cross-section was set to 4.0 cm, 4.5 cm, 5.0 cm and 5.5 cm, respectively. Along the aorta axis, lofting was made by contours of three sections by a CAD (Computer Aided Design) tool (SolidWorks2015, SolidWorks Inc., France). The final four models named Model1, Model2, Model 3 and Model 4 (M1, M2, M3 and M4) are shown in Fig. 1. In this study, hemodynamic parameters from the aortic model, such as streamline, spiral flow, wall shear stress, and secondary flow, were used to represent the position, length, and direction of the parametrically altered dilation.
Fig. 1
Four anatomical models of BAV anatomical models were established. (A) The diameters of the ascending aorta (AAo) are 4.0 cm, 4.5 cm 5.0 cm and 5.5 cm, respectively; while, the size and the appearance of other parts are fixed; (B) Regions of interest where the hemodynamics were analyzed
Fig. 2
The cross-sectional velocity profile of the inlet at the AAo. The data is obtained from in vivo measurements. (A) Inlet velocity waveform over one cardiac cycle. (B) Outlet pressure waveform over one cardiac cycle
Fig. 3
Flow pattern within the AAo analysis at the peak systole phase (t = 0.17s) and the late systolic phase (t = 0.29s) by drawing lines that are tangential to the instantaneous velocity vectors. These lines are contoured by velocity magnitude
Fig. 4
Vector contours of two sections at peak systole. The (A) and (B) display the flow pattern of the sinotubular junction (plane 1) and the proximal AAo (plane 2), respectively. The left side of the contours is the outer wall and the right side is the inner wall
Fig. 5
Pressure distribution (mmHg) displays the WSS distributions of the four models with different diameters at peak systole (t = 0.17s) (mmHg)
Fig. 6
Displays the WSS distributions of the four models with different diameters at five featured moments
Fig. 7
The histogram displays oscillatory shear index (OSI) average value of the inner (the blue color column) and outer (the red color column) wall in each model
MeshingA semi-automatic adaptive meshing technique was employed in HyperMeshv10.0 (Altair HyperWorks, Troy, MI, USA) to optimize both computational efficiency and element quality. 3D aortic models were meshed with tetrahedral elementsin the core region and prismatic cells (5 layers) in the boundary layers near the aortic wall, as shown in Supplemental Fig. 1. The grid was divided into various entrance, exits and the inner/outer of AAo regions. The number of elements and nodes of models meshed are shown in Supplemental Table 1.
Boundary conditions and flow modelsTransient analysis was adopted to investigate the pulsationof blood flow. No-slip boundary conditions were assigned at the wall in all cases. The numerical simulation was based on the three-dimensional incompressible Navier-Stokes equations and continuity equations:
$$\rho \left[ \over }} \right) + (\vec u \cdot \nabla)\vec u} \right] + \nabla p - \nabla \cdot \tau = 0$$
(1)
$$\nabla \cdot \vec u = 0$$
(2)
Where \(\:\overrightarrow}\)and p represent the fluid velocity vector and the pressure respectively. ρ denotes the blood density( ρ = 1050 kg/m3), and τ is the stress tensor. It was assumed that blood is incompressible, and blood has same kinematic viscosity and density of a Newtonian fluid [16]. The relative viscosity of blood is 4 ~ 5 mPa/s. The blood density is 1.050 ~ 1.060 ml/g.
Time-varying velocity profile was imposed at the inlet of the aorta, based on the flow velocity waveforms obtained from the Doppler ultrasound measurementsof 20 volunteers [17],which was detailed in Supplemental Table 2. The flow rates entering the brachiocephalic, left common carotid, and left subclavian arteries were specified to be 12%, 5% and 8% of the blood flow rate entering the aortic root, respectively [18, 19]as shown in Fig. 2A. A pulsatile waveform of pressure was assigned at the thoracic outlet for the simulation, as depicted in Fig. 2B.
The calculation time step and cardiac cycle were set to 0.01s and 0.8s, respectively. To minimize the influence of initial flow conditions, all simulations were carried out by a commercial finite-volume-based CFD solver (Fluent14.5, ANSYS, Inc., USA) for six cardiac cycles to achieve a periodic solution, and the results presented here were obtained in the sixth cycle. In the current study, the convergence criteria were set to 1.0E-18 to run 120 iterations for each time step. Grid and time step independence tests were conducted in the current study, confirming the rationality of the base grids and base temporal resolution in this study. The base grid consisted of 915,330 elements, while the finer grid comprised 1,903,254 elements. To quantify flow differences, wall shear stress (WSS) at the test position was compared between the base grid model and the finer grid model. The results showed that WSS exhibited identical variation patterns between the base and finer grid models, with an average discrepancy of 1.62%. Additionally, we conducted a study on time independence. The base time step was 0.01 s, while the finer time step was 0.005 s. Comparing the exact variations in wall shear stress between the test models, we found an average difference of 2.31%.The results of time and mesh independence test were detailed in Supplemental Fig. 2.
Derived hemodynamic parametersDerived hemodynamic wall parameters include the velocity, pressure, WSS, and oscillatory shear index (OSI). WSS is an analytical factor used to describe the dynamic friction between the viscous fluid and the solid wall, which is caused by the lateral movement of the viscous fluid. The time-averaged wall shear stress (TAWSS) is obtained by averaging the WSS in a cardiac cycle and is a better representative of WSS.
$$TAWSS}} \over T}\int_}^T $$
(3)
OSI reflects the cyclic departure of the WSS (or velocity) vector from the predominant direction of blood flow and is calculated as Eq. (4):
$$OSI = \left( dt} } \right|} \over } \right|dt} }}} \right)$$
(4)
where \( }\) is wall shear stress and T is one cardiac cycle. The OSI values vary from 0 to 0.5: 0 represents unidirectional flow, and 0.5 signifies complete oscillatory flow.
In this study, after the completion of CFD calculation, CFD-POST was imported for post-processing, and the peak pressure, wall shear stress (WSS), shear strain rate (SSR), and time averaged wall shear stress (TAWSS) and time averaged shear strain rate (TASSR) of each node of the ascending aorta wall during the cardiac cycle were output. In order to describe the results intuitively, five featured moments selected from one cardiac cycle based on the velocity waveform of the aortic inlet, including the early systolic phase (t = 0.10s), the peak systole phase (t = 0.17s), the late systolic phase (t = 0.29s), the maximum regurgitation phase (t = 0.43s) and stable diastolic phase (t = 0.51s), respectively.
Comments (0)