
Remember me





First, we examined whether our study sample reflected the use of PC at the end of life in Germany. For this purpose, we analyzed the development of the utilization rates for OPC and IPC (percentage of deceased insured persons with OPC or IPC out of all deceased insured persons in a given year). The use of OPC increased from 25.5 to 28.8% from 2015 to 2019. IPC use increased from 7.7 to 8.5%. The results of the utilization rates for OPC and IPC can be found in Supplement Figure S2.
Study cohortStudy population for inpatient palliative care at baselineOur study cohort consisted of 43,896 patients, of whom 20,015 (45.60%) were male and 23,881 (54.40%) female. At baseline the mean age was 78.62 years. 558 patients (1.27%) received IPC and about 20% of the patients were already living in a nursing home at baseline. (Table 1). A cancer diagnosis was documented for 21.72% of the study participants; 24.84% had a dementia diagnosis, 47.71% had neither dementia nor a cancer diagnosis. About 5% had a combination of dementia and cancer diagnosis. The most common comorbidities in the study group were diabetes (43.48%), congestive heart failure (42.33%), cardiac arrhythmias (39.54%) and renal diseases (35.71%). Dementia-related medications were prescribed to more than 40% of patients (Table 1). The average observation period was 2.94 quarters (one quarter minimum, four quarters maximum).
During the observation period, the distribution of patients between groups changed. At the beginning of the observation period, most patients were still non-dementia & non-cancer patients, but by the quarter of death, the largest group were the dementia patients with 32.79%. Non-dementia & non-cancer patients were the second largest group with 31.28%, followed by the cancer patients (24.77%). The proportion of the patients group cancer & dementia increased to 6.05%, the group dementia & subsequent cancer increased to 2.17%, and the group cancer & subsequent dementia increased to 2.95%. In subsequent quarters, the proportion of patients with an IPC prescription increased to a proportion of 11.89%. All results can be found in supplement Table S4.
Inpatient palliative care patients at prescriptionAt time of IPC prescription (N = 9,699), more than half (57.26%) were diagnosed with cancer (Table 1). Non-dementia & non-cancer patients were the second largest group, accounting for 18.79% of all IPC patients. Patients were often affected by disturbances in fluid and electrolyte balance (64.14%), peripheral vascular disorders (46.19%), congestive heart failure (44.95%), and peripheral vascular disorders s (44.36%). More than a third of patients (34.43%) were already receiving OPC.
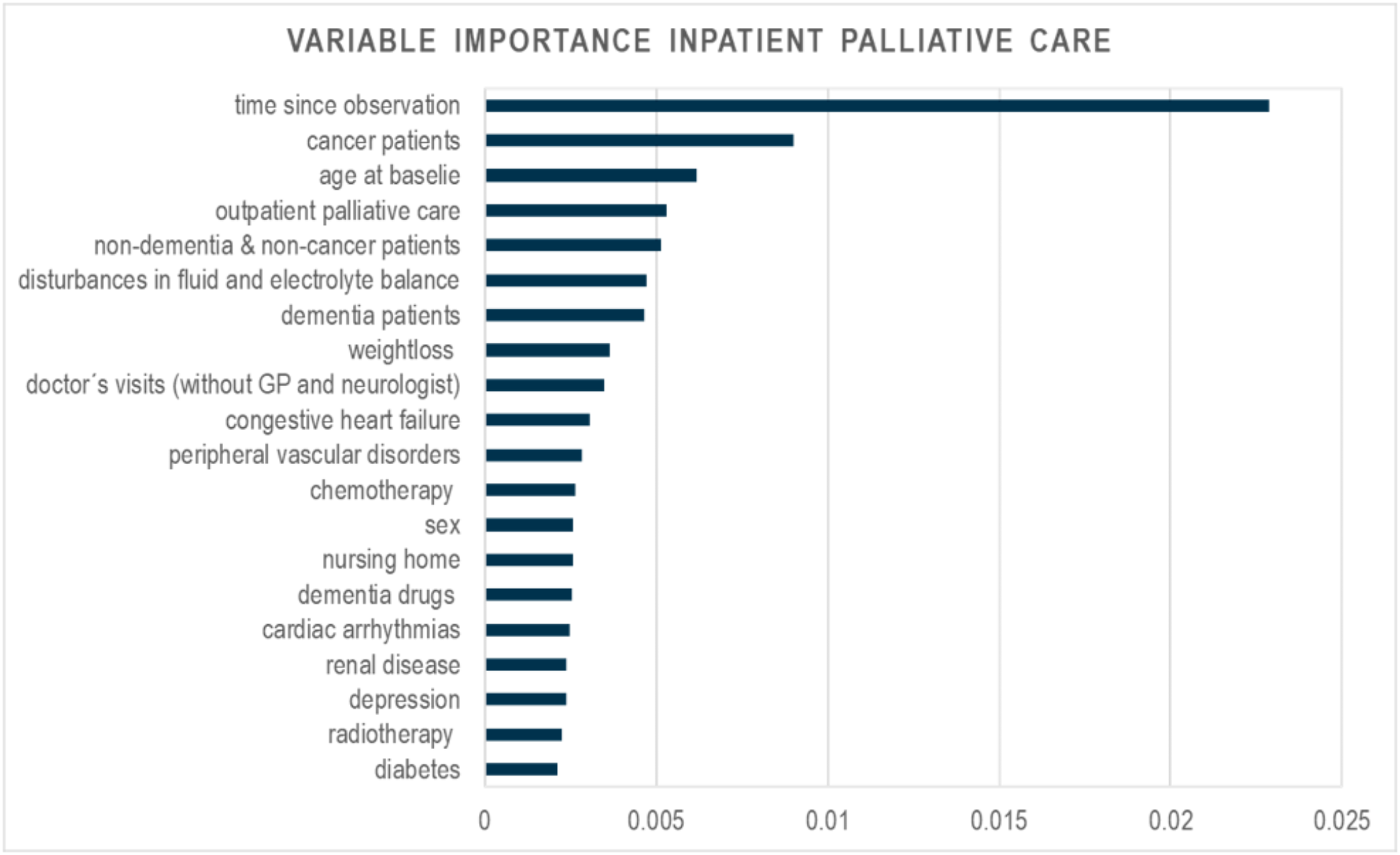
Table 1 Characteristics of the study population at baseline and the time of prescription of IPCFig. 1
Variable importance for the model of inpatient palliative care. AOK data 2014–2019
Study population for outpatient palliative care at baselineThe dataset included a total of 37,430 patients. Of these, 48.77% had no dementia & no cancer diagnosis, 27.13% had a dementia diagnosis and 18.14% had a cancer diagnosis. Around 6% of patients had a cancer and dementia diagnosis (Table 2). The mean age at baseline was 79.28 years. The most common comorbidities with a frequency of over 30% were disturbances in fluid and electrolyte balance, depression and renal disease (Table 2). About 21% of all patients live in a nursing home and 8% receive long-term care. The average observation period was 2.94 quarters (one quarter minimum, four quarters maximum).
The distribution of patients among the groups changed during the observation period. The proportion of non-dementia & non-cancer patients decreased over the observation period from 48.77 to 34.87%, while the proportion of patients in all other patient groups increased. At the end of the observation period, 33.99% of the patients had a dementia diagnosis and 20.93% had a cancer diagnosis. 5.57% of the patients were cancer & dementia patients, and 1.85% of the patients were dementia & subsequent cancer patients. The proportion of cancer & subsequent dementia patients was 2.79%. At baseline, 4.31% of patients (n = 1,612) were already receiving OPC prescriptions. In subsequent quarters, the proportion of patients with a prescription varied. Only shortly before death the proportion of patients increased to 15.36% (quarter of death). All results can be found in supplement Table S5.
Outpatient palliative care patients at prescriptionOPC patients (N = 9,992) were predominantly cancer patients (41.57%), followed by dementia patients (30.77%) (Table 2). Women were more likely to receive OPC (58.13%) and the most common comorbidities were disturbances in fluid and electrolyte balance (68.04%), renal disease (49.51%), and depression (42.96%). In addition, 11.19% of patients had previously received IPC.
Table 2 Characteristics of the study population at baseline and the time of prescription of OPCFig. 2
Variable importance for the model of outpatient palliative care. AOK data 2014–2019
Model evaluationFirst, we used both a glm and a cforest to predict IPC as well as OPC. The cforest had a higher discriminatory power than the glm model for the prediction of IPC. However, the calibration of the cforest was worse than that of the glm model. All results are shown in Supplementary Table S6 and Figure S3. Therefore, we used a combined model of both approaches. The c-index was 0.737 (95% CI = 0.721–0.754), and the calibration was acceptable with an intercept of -0.023 (95% CI = -0.030 - -0.016) and a slope of 1.418 (95% CI = 1.332–1.504) (Fig. 3).
Fig. 3
Calibration plots. Intercepts and slopes were calculated using logistic recalibration (95% confidence intervals in parentheses)
The discriminative power of glm and cforest for OPC was comparable. The glm model tended to slightly overestimate the predicted values, while the cforest had the opposite effect and tended to underestimate the predictions. All results are shown in Supplementary Table S6 and Figure S3. Again, we decided to combine both models to predict OPC. The c-index was 0.689 (95% CI = [0.675–0.704]), and the calibration plot showed that the combined model was better calibrated than the individual models, with intercept close to 0 and slope close to 1 (intercept: -0.006; 95% CI = -0.010 - -0.003; slope: 1.122; 95% CI = 1.083–1.161) (Fig. 3).
Most important variablesInpatient palliative careThe most important variable was the time since observation (Fig. 1). The second and third most important variables were cancer diagnosis and age at baseline. In addition to cancer diagnoses, non-dementia & non-cancer, and dementia diagnoses were among the top 20 predictors (3/6). Eight diseases from the comorbidities (disturbances in fluid and electrolyte balance, weight loss, congestive heart failure, peripheral vascular disorders, cardiac arrhythmias, renal disease, depression and diabetes) (8/28) and one therapeutic remedy and rehabilitation (number of doctor´s visits) (1/8) were among the most predictive factors. Three medical interventions and major medications (chemotherapy, dementia medications, radiotherapy) (3/5), and two care interventions (OPC and nursing home) (2/5) were also among the top 20 predictors.
The probability of prescribing IPC was primarily increased by characteristics of comorbidities, medical interventions and major medications (Supplement Figure S4). Patients who receive chemotherapy (OR = 1.51; 95% CI = 1.41–1.61), radiation therapy (OR = 1.10; 95% CI = 1.05–1.15), or dementia drugs (OR = 2.95; 95% CI = 2.69–3.24) had an increased probability of IPC compared to patients who did not receive any of these medical interventions or major medications (Table 3). With each quarter of observation, the probability of IPC increased. Women and patients who had already received OPC had a significantly increased probability of IPC (women: OR = 1.16, 95% CI = 1.11–1.22; OPC: OR = 1.65 95% CI = 1.56–1.73).
All patient groups had a significantly lower probability of receiving IPC compared to cancer patients (dementia: OR = 0.28, 95% CI = 0.26–0.30; non-dementia & non-cancer: OR = 0.30, 95% CI 0.20–0.32; cancer & dementia: OR = 0.61, 95% CI = 0.56–0.67; dementia & subsequent cancer: OR = 0.70, 95% CI = 0.60–0.82; cancer & subsequent dementia: OR = 0.58, 95% CI = 0.51–0.67).
Table 3 Odds ratios from logistic regression with inpatient palliative care as the outcomeOutpatient palliative careThe most important predictor was time since observation (Fig. 2). This was followed by non-dementia & non-cancer diagnosis and cancer diagnosis. In addition to these diagnosis dementia, cancer & dementia were predictive for OPC (4/6). The comorbidities weight loss, disturbances in fluid and electrolyte balance, depression, paralysis and renal disease (5/28) were predictive for OPC. In addition to time since observation, the demographic factors of age at baseline and sex were important predictors of OPC (3/3), as well as long-term care, IPC and nursing home from care interventions (3/5), doctors’ visits (without GP and neurologist), physiotherapy and rehabilitation from therapeutic remedies and rehabilitation (3/8), and chemotherapy and radiotherapy from medical interventions and major medications (2/5).
The probability of an OPC prescription was mainly influenced by the comorbidity structure of the patients, as well as therapeutic remedies, rehabilitation and care interventions (Supplement Figure S5). The OPC probability increased significantly with the use of physiotherapy (OR = 1.09; 95% CI = 1.03–1.15), rehabilitation (OR = 1.58; 95% CI = 1.38–1.82), chemotherapy (OR = 2.05; 95% CI = 1.89–2.23) and radiotherapy (OR = 1.57; 95% CI = 1.38–1.80) (Table 4). Patients with existing care intervention also had an increased probability of OPC compared to patients without these care (long-term care: OR = 1.93, 95% CI = 1.83–2.05; nursing home: OR = 1.49, 95% CI = 1.41–1.57; IPC: OR = 1.97, 95% CI = 1.82–2.13).
The probability of OPC was lower in all groups (except those with dementia & subsequent cancer diagnosis) compared to those cancer diagnosed (dementia: OR = 0.33; 95% CI = 0.31–0.36; non-dementia & non-cancer: OR = 0.18; 95% CI = 0.17–0.19; cancer & dementia: OR = 0.64; 95% CI = 0.59–0.70; and cancer & subsequent dementia: OR = 0.54; 95% CI = 0.48–0.62).
Table 4 Odds ratios from logistic regression without patient palliative care as the outcome
Comments (0)