Our scoping review aimed to systematically map empirical studies of the perspectives, attitudes, and experiences of healthcare professionals, dying patients, and their next of kin, about introducing noninvasive medical technology in EOL care.
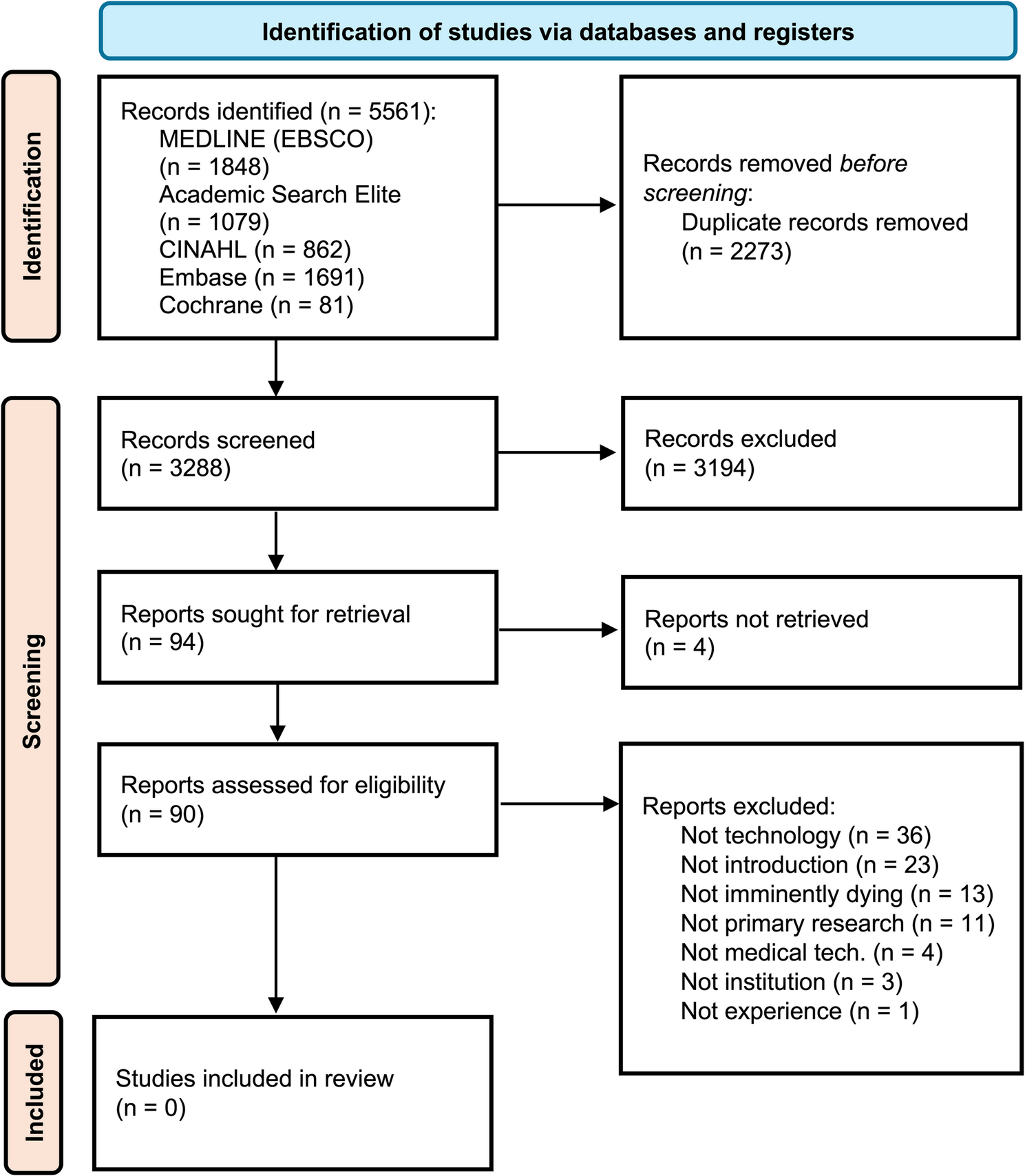
Our systematic search revealed that our empirical knowledge on the topic is limited. While the absence of eligible studies in this review might appear as a limitation, the fact that our review identified no empirical evidence from published studies on this topic is an important finding, highlighting a potentially important research gap. Such knowledge is important to understand whether the common EOL care practice of reducing technological load as patients approach death aligns with the perspectives and attitudes of those most affected by them.
We believe that the absence of published studies imply that the technological progress in improving patient care in other areas of nursing and medicine has not reached the field of EOL care, as problematized by White et al. [36]. They noted that research in this field is both challenging and controversial and that little is known about the viewpoints of dying patients and their next of kin. Additionally, as Kars et al. [37] noted, health care professionals work as gatekeepers in recruiting patients at the EOL to participate in research, which may also make the process of accessing this field more difficult. From our point of view, this becomes an ethical issue as well. We know that dying is a dreaded part of human life, and as such, it is pertinent to ensure that we provide state-of-the-art EOL care when patients are approaching death. Thus, there seems to be a need to ensure that technological development aiming to improve our knowledge of what takes place in the last hours of life is an area of importance that needs to be addressed.
In our search for articles, one study indirectly implied that dying while being attached to technology is forwarded as less peaceful and dignified than being without, but that sometimes next of kin found comfort in how technology such as heart monitoring provided information about the patient status [44]. For example, nurses may believe that EOL care is high-touch, rather than high-tech [45], and may also stand in the way for health care professionals to recognize patients as dying [46].
Furthermore, literature from related areas offers useful lessons. For example, there is evidence that digital tools such as telecommunication platforms or electronic records can help coordinate care and support patient centered practice, if they enhance rather than replace direct human contact [47]. In other words, technology is more acceptable when it is clearly an aid to everyday care and is a supplement rather than a substitute for it. It is conceivable that similar principles could guide the introduction of noninvasive medical technology in a way that can support the relational aspects of care in the EOL setting.
In one study, nurses reported inexperience with assessing symptoms near the EOL. Being able to identify subtle signs of agitation, pain and discomfort, are essential prerequisites for optimal EOL care and a necessary skill for nurses and physicians [48]. However, another study found that the electronic patient records of hospitalized dying patients often lacked assessment of pain intensity and according to the electronic patient records, 10% of the patients receive inadequate pain management [49]. It is conceivable that transient use of other sensor technologies (e.g. sweat, respiratory rate, and movements) for the purpose of provide information that is otherwise inaccessible to optimize symptom relief. For example, we know that the use of EEG technology in other fields has provided useful knowledge about patients’ states; noninvasive brain monitoring during general anesthesia is commonly used to ensure the patients are in a state suitable for surgery [50]. Such monitoring equipment may inform health care professionals not only about patients’ capacity to feel pain but also about the extent to which they can hear and understand their loved ones, despite their ability to communicate by normal means. Therefore, such technologies may provide information about the patient state that would otherwise remain unattainable. However, without high-quality, empirical research on the population in question, we may never know whether and to what extent noncommunicating patients in EOL covertly retain these capacities.
The strong tradition of “Total Care” in EOL settings reminds us that technology can unintentionally shift attention toward what is easily measured and away from the psychosocial and spiritual dimensions of care [51]. Analyses of smart sensor technologies highlight the need for careful, purposeful adoption that respects patient autonomy and maintains holistic care [51]. Furthermore, a study suggested that technologies mediate care in complex ways: they can make relational work less visible, but when used thoughtfully, they can also enhance attentiveness and support caregivers in ways that align with EOL values [52]. Such adjacent work may help provide a practical framework for how non-invasive medical equipment may be introduced responsibly and in harmony with the principles of EOL care.
We believe that distinguishing between technology as a contributor to overtreatment and noninvasive technology with the potential to improve symptom management is pertinent [35]. From our point of view, technology in itself is considered a source that disrupts peaceful dying—at least, technology other than what is used to administer sedatives and analgesics. We are well aware of the complexity of the situation and the need for a highly sensitive approach. However, we argue that these established practices influence our approach to conducting research involving dying patients [36, 37]. This may stand in the way of allowing technology to improve our knowledge of the dying process and thus our ability to care for our patients.
So, what kind of knowledge can we establish through an empty review? Obviously not the kind of knowledge that we hoped to find. Hence, we are not in a position to offer any strong conclusions regarding perspectives on, attitudes toward, and experiences with the introduction of noninvasive technology when the patient is dying. However, we argue that this empty review provides us with insight into several aspects that may shed light on why we could not find relevant studies. Yaffe et al. [53] conducted an analysis of Cochrane reviews with no included studies and described the following factors of what characterizes empty reviews: the novelty of the field, the circumstances of the study, such as population and context, or too rigid inclusion criteria. We believe that all these factors may be relevant in explaining our empty scoping review. The research team frequently discussed the possibility of widening the inclusion criteria to see if that would lead to relevant articles. However, we landed on keeping the criteria as they are.
There are several aspects of our methodology that should be considered for transparency. Our research question and inclusion criteria, focused on empirical studies of how users and stakeholders view the introduction of noninvasive medical technologies in the EOL setting, explains why no eligible studies were identified. A broader scope, for example including grey literature, studies of related technologies such as telehealth or electronic patient records, or work outside of the terminal stage, may have yielded more material for synthesis. However, we considered such broadening carefully and concluded that it risked diluting our central question.
There may be synonyms of both EOL and noninvasive medical technology that we may not have been able to identify and include in our search strategy. Our review also had some language limitations. Consequently, there may be studies we may not have been able to identify. Another limitation could be that we did not include grey literature, as we wanted to map published studies. However, it is the aim of the review that decides was type of studies or literature that should be included, and given the sensitivity of the field, we wanted to make sure to include studies that had been approved by registered ethical committees and peer reviewed. Furthermore, work in our team to best capture our research question, led to a search strategy that was broad with regards to the population [42] (patients, health care professionals, and next-of-kin) and experiences considered (perspectives, attitudes, and experiences) but narrow in terms of timeframe (imminently dying) and technologies (noninvasive medical technology attached to the patient).
Lastly, the term “non-invasive technology” in palliative care is frequently applied to a wide range of devices, including telemedicine solutions, mobile applications, artificial intelligence-driven support tools, and wearable sensors [47]. Our specific interest was to map research on wearable medical technologies; consequently, our use of “non-invasive technologies” reflects a narrower scope than what is typically described in the broader literature in this field.






Comments (0)