Patients’ demographic characteristics
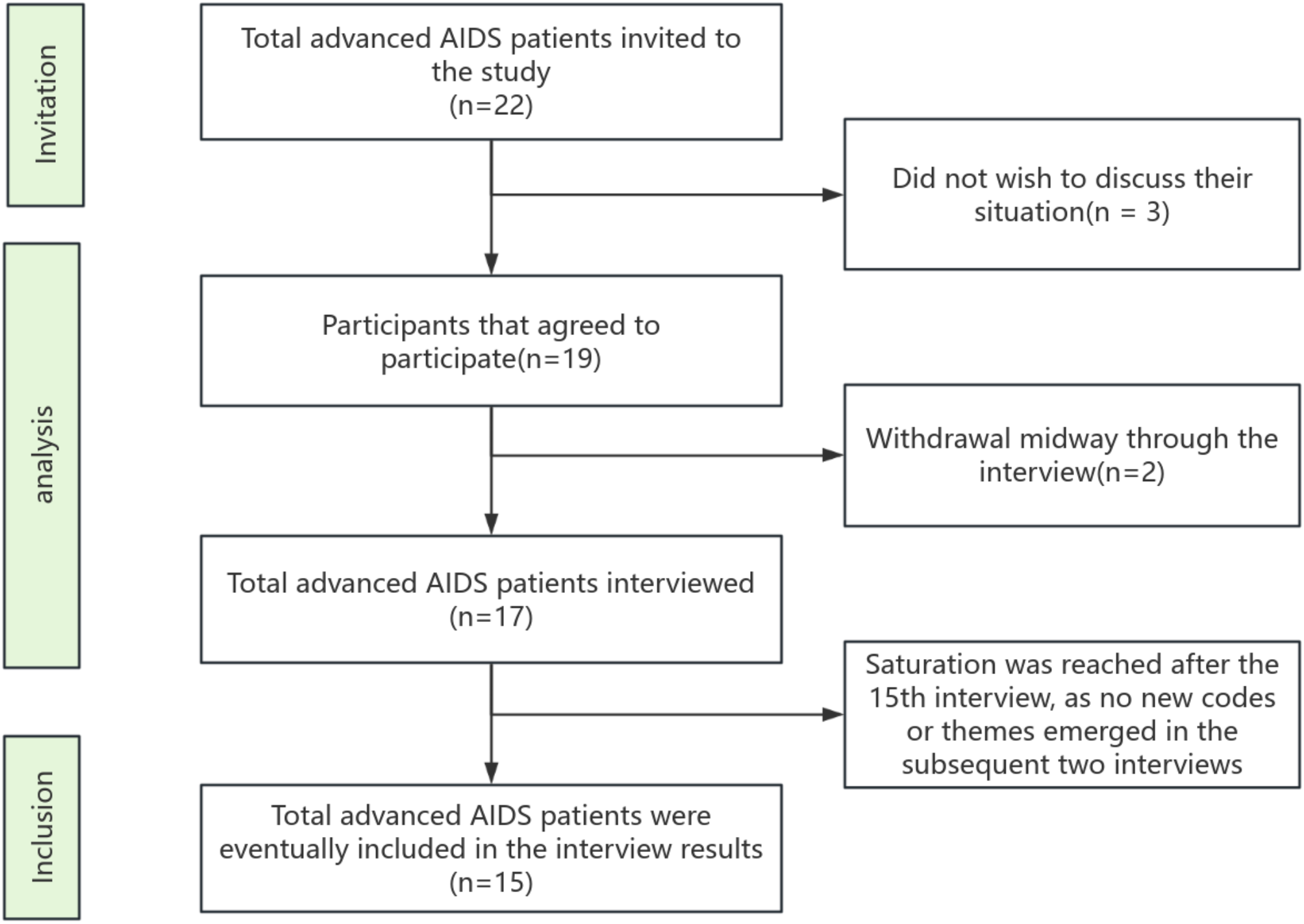
Between March and May 2024, A total of 22 potential participants were contacted between March and May 2024, and a total of 17 participants were eventually interviewed, reaching saturation after the 15th interview, 15 advanced AIDS patients were finally included in this study as no new codes or themes emerged in the two subsequent interviews. To protect patient privacy, patients were assigned numerical codes in the order of their participation in the study, with the letter N preceding the numerical code, and the patients numbered N1, N2, N3……N12, and N15. The study participants’ place of residence was from rural and urban areas, 10 (66.67%) patients The study participants were from rural and urban areas, 10 (66.67%) patients were aged > 50 years, 10 (66.67%) were males, 2 patients were religiously affiliated, 6 (40%) patients were married, only one patient was homosexual, 6 (40%) were highly educated and 6 (40%) were aware of their HIV serostatus for at least 10 years. Table 2 shows the demographic information of the study participants.
In this section, four themes emerged from the interviews and were discussed with the support of direct quotes from patients. This study found that the palliative care needs of advanced AIDS patients were not adequately met, as evidenced by (1) Physiological needs (Relief of multiple physical symptoms, need for self-care); (2) Informational needs (Knowledge and guidance on HIV treatment, Drug-related information, Participation in communication and medical decision-making, Choosing a palliative care place); (3) Psycho-spiritual needs (Desire for respect and companionship, Preservation of dignity and reduction of discrimination, guilt and ambivalence towards family, worries and fears for the future); (4) Social support needs (Social interaction, financial support, continuity of care needs) Table 3 describes the themes and sub-themes that emerged from the study.
Table 2 Sociodemographic characteristics of advanced AIDS patients (N = 15)Table 3 Themes and subthemes for palliative care of advanced AIDS patientsTheme 1 Physiological necessitySubtheme: Relief of multiple physical symptoms
The majority of advanced AIDS patients repeatedly mentioned in interviews the persistence of symptomatic distress, including AIDS-related symptoms and adverse reactions caused by medication, especially insomnia, pain, and fatigue, which affected their daily lives; symptoms such as coughing and recurring fevers further aggravated physical discomfort. Although some of the symptoms were partially relieved by treatment during hospitalization, the overall situation has not completely improved and continues to have a serious impact on the quality of life of the patients.
“The kidneys on both sides of my lower back hurt excruciatingly (rubbing the area). The pain is constant and recurring, making it impossible to sleep, even with painkillers. It’s so irritating and offers no relief.” (N6, male, age 75, urban).
“I have no strength in my body, no strength, no strength at all, no strength at all, what should I do? (crying quietly)” (N11, male, age 55, urban).
Subtheme: Need for self-care
Many patients gradually lost their ability to care for themselves due to the deterioration of their illness and expressed a strong need for assistance with daily activities during the interviews, mainly in terms of control over their movements and independence in life. However, due to the impact of the disease, many patients often had limited mobility were often dependent on the help of others, and were unable to take full control of their lives. However, age-related differences were also evident, with participants over the age of 50 expressing greater concern about mobility and loss of independence.
“Being here for a long time in the future for dialysis is cumbersome for one person to be admitted to the hospital because of problems with vision due to age and not being good at operating the process of treatment or payment.” (N2, male, age 57, urban).
“I got this disease at a young age and I have parents and children to support, every day I just lie in the hospital, I’m weak, I can’t do anything, I can’t go to work, I don’t know what to do, I want to earn money to support my family.” (N13, female, age 29, urban).
Theme 2: Information needsSubtheme: Knowledge and guidance on HIV treatment
Advanced AIDS patients generally lacked sufficient knowledge related to disease treatment in the face of a complex condition. They wanted more timely and detailed information on the progress and effectiveness of disease treatment, treatment options, next steps, and prognosis. For more guidance, especially in coping with and managing common symptoms. Some patients mentioned that they could only obtain information on their own through the Internet or other sources, but the accuracy and applicability of this information could not be guaranteed.
“My idea is the first one is to add a little bit of family promotion on family HIV prevention and control so that no one thinks that if a family lives together they will be infected, and the second question is what is the bridging program for the medication taking process for retired, off-site patients like us.” (N2, male, age 57, urban).
“I noticed red bumps a year ago and thought it was a skin disease, but it worsened. After searching online, I suspected AIDS. A home test kit confirmed my fears, and the hospital diagnosis felt like my world collapsed.” (N14, female, age 44, rural).
Subtheme: Drug-related information
Patients generally report difficulties in obtaining disease-related information, and they want to know more about how medications are used, potential side effects, and their relationship to symptom management. However, serious problems such as information asymmetry arise due to insufficient communication between doctors and patients and the often overly specialized information provided, resulting in patients’ difficulty in understanding and often feeling confused and anxious.
“When I asked the doctor about the medicine, he explained, but I couldn’t understand. I just trusted the prescription and took it without knowing what it was for (shaking hands)?” (N3, male, age 39, rural).
“Yes, I still want to know about my disease, some of its treatment options and medication and so some (knowledge), and my treatment of other diseases need to eat the medicine there is no influence and conflict, what are the side effects? What’s it all like?” (N4, male, age 84, rural).
Subtheme: Participation in communication and medical decision-making
In addition to treatment progress, patients also wanted to know the future direction of their condition, aspired to have more autonomy in disease management and treatment, and hoped that doctors and nurses could communicate with them about their condition, rather than just passively accepting treatment options, and they hoped that doctors would listen to them and respect their choices.
“The doctors seem to be pretending like they don’t know. I’ve had lab tests so many times, and I’ve told the doctor that my skin was itchy, but nobody cared. I kept saying it, and it seemed to annoy them, so now I don’t dare to mention it anymore.” (N2, male, age 57, urban).
“When the doctor checks on me every morning, they talk among themselves and don’t explain anything to me. After they leave, I still don’t know my current condition. I wish they would communicate properly, ask questions, and help me understand what’s happening. It would give me peace of mind.” (N13, female, age 29, urban).
Subtheme: Choosing a palliative care place
Patients demonstrated a strong need when it came to choosing a suitable place of care, however, many patients reported a lack of comprehensive information about the different places of care, including information on the treatment options available, the type of services provided, the healthcare-related costs and the quality of care, as well as various limitations and barriers to accessing them, which resulted in patients often struggling to make an appropriate choice.
“I didn’t know which hospital to go to receive appropriate treatment care; no one gave me clear guidance. I had to rely on internet searches, which only added to my anxiety.” (N3, male, age 39, rural).
“The community hospital transferred me but they did not explain why, only that they did not want me to stay in the hospital anymore; I felt abandoned and lost.” (N10, female, age 58, rural).
In addition, geographic and socio-economic factors played an important role in decision-making. For example, the challenge is more acute for patients in rural areas. Limited healthcare facilities and the cost of traveling add to their burden. Patients from rural areas tend to spend more time and money and have limited options, while those living in cities cite concerns about overcrowding in hospitals and difficulty in staying there.
“It’s not just about finding the right place, it’s about how far I have to travel and whether I can afford to go there.” (N12, female, age 56, rural).
“The city hospital is better equipped but it is always full, I have to queue for a long time every time to be admitted and I don’t know if they will be able to admit me in time.” (N2, male, age 57, urban).
Theme 3: Psycho-spiritual needsSubtheme: Desire for respect and companionship
AIDS patients, especially those in the terminal stage of the disease, face great psychological pressure and loneliness. They longed for more love and companionship from family, friends, and healthcare professionals. Many patients mentioned that they felt socially isolated and lacked emotional support due to the specificity of the disease. However, it is worth noting that female participants emphasize social stigma and discrimination more frequently than male participants, and hope to be understood and accompanied by their families.
“Because of my condition, my parents don’t understand me and feel ashamed of this disease, I am afraid to get close to my children and some hospitals treat me differently…” (N14, female, age 44, rural).
Compared to the female participants, the male participants were more inclined to discuss their concerns about their jobs as well as financial instability.
“I am under a lot of stress because of this disease, I am afraid of losing my job if my colleagues and bosses in the company find out, and my wife has divorced me.” (N15, male, age 47, rural).
Subtheme: Preservation of dignity and reduction of discrimination
Patients not only had to endure physical pain but also faced prejudice and discrimination from society. Many patients mentioned in the interviews that they felt different levels of discrimination during the medical process, and even in some public places, they encountered unfair treatment because of their condition.
“Going to another department for a checkup is still inconvenient; people know you have this disease and look at you strangely, almost like you’re contagious. I hope the community understands us better, as we don’t have any bad intentions!” (N8, male, age 52, rural).
Subtheme: Guilt and ambivalence toward family
For advanced AIDS patients, family relationships are often an important pillar in their journey through the disease. However, due to the long duration of the disease, many patients feel a deep sense of guilt towards their family members. They believe that they are not only a financial burden to their families, but also put their families under tremendous emotional stress. Patients’ attitudes towards treatment are often full of contradictions. On the one hand, they want to continue to adhere to the treatment, on the other hand, they worry about becoming a burden to their family.
“If there was a special help center, it would relieve my family’s burden so that I could also receive treatment with peace of mind. My mother is old and has to worry about me. I am so sorry for them (cover up the face and cry).” (N14, female, age 44, rural).
Subtheme: Worries and fears about the future
In the face of the irreversibility of the disease and the limited nature of treatment, the interviewed patients were filled with uncertainty and a sense of helplessness about the future effects of treatment and the outcome. This sentiment was strongly echoed in the interviews. Many patients expressed anxiety about their future survival, and patients were often skeptical about future treatments, especially if multiple treatments failed to bring about significant improvement, and they may develop a loss of confidence in treatment.
“I still have a child to support, and my parents depend on me. I feel helpless about the future. I hope to be cured, but after researching online, I know that there is no cure. This illness will follow me until I die (crying).” (N14, female, age 44, rural).
Theme 4: Social support needsSubtheme: Social interaction
Patients generally expressed the need for normal social interactions, especially in the face of illness and loneliness, and the desire to establish normal interactions and connections with family and friends, other patients, and the community. However, due to the special nature of AIDS, patients often suffered from social discrimination and rejection, coupled with the fact that many of them often suffered from deteriorating conditions, which led to great restrictions on social activities, and they hoped to receive understanding and support from society.
“Sometimes talking with other patients helps ease the heart, but we dare not share too much due to privacy concerns. Everyone is afraid of others spreading rumors, and I do not want to discuss my illness with others.” (N1, female, age 56, rural).
“It’s just me, you know it’s a bit inconvenient for us to talk and communicate all this in the first place, and there’s no one to communicate with…” (N15, male, age 47, rural).
Subtheme: Financial support
Financial stress is a significant issue for advanced AIDS patients. Many patients often reported that the high cost of treatment and daily living expenses were overwhelming that expectations for treatment and recovery from the disease were often limited by their financial situation, and that lack of financial support prevented effective treatment, so many patients mentioned the need for more financial support.
“Can the medical fees be further reduced a little bit for special people like us, you see we would have had this humiliating disease, and it’s not good to borrow money, not good to tell our relatives. Seriously, it would be better if there could be some financial help to ease the burden on the family.” (N6, male, age 75, urban).
“If we can provide help, we hope that the medical fees can be reduced a little bit, you see we are all rural people, we don’t have any money, and we still want the hospitalization fees to be lower.” (N10, male, age 58, rural).
Subtheme: Continuity of care needs
Patients want continuity of care after the disease has reached its terminal stage. However, existing continuity of care resources are insufficient, such as bed constraints and inter-regional transfers, leaving patients with a severe care gap after discharge. This care disconnect leads to significant uncertainty and safety risks for patients after discharge, and they would like more support to ensure timely care in the event of a change in their condition.
“My family and friends abroad told me that in foreign countries when a patient is hospitalized, family members are not allowed to enter for care. The hospital provides comprehensive care for the patient until discharge and even offers psychological counseling to the family after the patient passes away. But it’s not like that here. We need holistic care like they have abroad.” (N2, male, age 57, urban).
“To be honest, after discharge, it’s inconvenient to return. Hospitals often require advance bed reservations, and transferring to other hospitals is complicated. Smaller hospitals often say they don’t have the necessary medicine or can’t provide treatment, making it very inconvenient.” (N10, male, age 58, rural).






Comments (0)