
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Remember me
Occupational lung diseases, such as silicosis, are a significant global health concern, especially with increasing exposure to engineered stone dust. Early detection of silicosis is helpful for preventing disease progression, but existing diagnostic methods, including x-rays, computed tomography scans, and spirometry, often detect the disease only at late stages. This study investigates a rapid, non-invasive diagnostic approach using atmospheric pressure chemical ionization-mass spectrometry (APCI-MS) to analyze volatile organic compounds (VOCs) in exhaled breath from 31 silicosis patients and 60 healthy controls. Six different interpretable machine learning (ML) models with Shapley additive explanations (SHAP) were applied to classify these samples and determine VOC features that contribute the most significantly to model accuracy. The extreme gradient boosting classifier demonstrated the highest performance, achieving an area under the receiver-operator characteristic curve of 0.933 with the top ten SHAP features. The m/z 442 feature, potentially corresponding to leukotriene-E3, emerged as a significant predictor for silicosis. The VOC sampling and measurement process takes less than five minutes per sample, highlighting its potential suitability for large-scale population screening. Moreover, the ML models are interpretable through SHAP, providing insights into the features contributing to the model's predictions. This study suggests that APCI-MS breath analysis could enable early and non-invasive diagnosis of silicosis, helping to improve disease outcomes.
Export citation and abstractBibTeXRIS
Workplace dust exposures contribute substantially to the burden of occupational lung diseases (OLDs) with a resurgence of pneumoconiosis (or dust-induced lung fibrosis) over the last 10 years [1]. In particular, silicosis is an emerging epidemic both in Australia and internationally, impacting broad cross-sections of the population [2–4]. Globally there were over 138 000 reported incident cases, 2.6 million prevalent cases, and over 12 000 deaths attributable to silicosis in 2019, with highest prevalence rates in China, North Korea, Chile and Mexico [5, 6]. This is a 64.4% increase from around 85 000 incident cases globally in 1990, predominantly due to the mining industry and the expansion of the artificial stone industry [7, 8]. A recent study found that more than one in four stonemasons in Victoria who had worked with artificial stone benchtops developed silicosis [9]. Without established treatments, silicosis and silica-related diseases will continue to strain the resources of the health and medical sectors. While preventative measures exist to reduce exposure (e.g. exposure limits and personal protective equipment), they are often not adhered to; hence early detection has the greatest potential to improve survival rates [10].
OLDs, including silicosis, are currently detected and diagnosed using long established methods including questionnaires, spirometry and plain chest radiographs [11]. While chest x-rays are the traditional mainstay of diagnosis and enable classification of disease according to the International Labour Organization system, they are insensitive for detecting disease in early stages as there is a delay between histopathological onset and radiographically visible lesions [12]. One recent study found that chest x-rays had sensitivities of only 48% when screening for disease presenting with only minimal opacities on the x-ray [13]. Furthermore, x-ray images cannot definitively identify specific disease due to radiological similarities and clinical overlap with other lung diseases [14]. Hence, further confirmatory invasive testing such as biopsies may be required for diagnosis. Unlike plain chest radiography, computed tomography (CT) scans offer a much higher level of detail and can be used to detect diseases in the early stage, but involve exposure to higher doses of radiation, and are more expensive [15]. Similarly, spirometry has shown limited sensitivity when detecting abnormalities in lung function in early-stage disease and even in severe disease results may fall within reference ranges [16]. Current silicosis surveillance methods rely on progression of lung disease to the stage that this is visible in imaging techniques or has significantly restrictive or obstructive lung function below the lower limit of normal. This reduces the likelihood of OLDs being detected in the very early stages where disease progression can more effectively be slowed, highlighting the need for new sensitive detection methods.
Exhaled breath analysis offers an additional non-invasive diagnostic approach that is rapid and agreeable to patients [17–19]. Such analysis would ideally enable large scale screening at the point of care by detecting volatile organic compounds (VOCs) as biomarkers for lung disease [20–22]. This field has expanded rapidly over the last 20 years, with significant application in lung disease detection, monitoring and screening. To date, exhaled breath analysis has proven application in asthma [23], chronic obstructive pulmonary disease (COPD) [24], lung cancer [25] and OLDs including asbestosis, [26, 27] but has not been widely investigated in silicosis [28]. The presence of disease changes metabolic processes which alter the chemical profile of breath [20]. When crystalline silica is deposited in the lungs, macrophages ingesting the dust particles cause an inflammatory response which releases potential biomarkers, altering the abundances and identities of aldehydes, alkanes, and other VOCs in breath [29–32]. Similarly, pulmonary fibrosis has been shown to increase the concentrations of a range of chemicals (carbon monoxide, nitric oxide, protein, 3-nitrotyrosine and 8-isoprostane) in exhaled breath condensate [33] and in exhaled breath [34]. Such 'breathprints' may enable the detection of early disease in individual workers; however, the concentrations of such chemicals are low, which highlights the need for ultra-sensitive methods in chemical analysis [35].
To develop accurate prediction models for disease state using large datasets such as untargeted MS data, supervised machine learning (ML) algorithms are commonly used [36]. Supervised ML methods are generally preferred to unsupervised methods such as principal component analysis as the majority of variance in bodily samples is not caused by the presence of disease and hence unsupervised methods are likely to classify the data based on alternate factors [37]. Supervised ML algorithms look for differences in the data based on the disease label, with different algorithms classifying the data based on differing methods such as linear combinations, hyperplanes, decision trees, or neural pathway modeling [37]. It is not trivial to predict which method will work best for different data sets as it is dependent on the relationship between features and this is often unknown, particularly for explorative research. However, more advanced ML approaches such as extreme gradient boosting (XGB) and neural networks (NN) have been designed for large data sets that are often non-linearly correlated [38].
Here, untargeted atmospheric pressure chemical ionization-mass spectrometry (APCI-MS) was used to obtain 'breathprints', followed by ML classification and Shapley Additive explanation (SHAP) analysis [39, 40] to discover features that could represent breath biomarkers for the early detection of silicosis. APCI-MS is a highly sensitive and rapid analytical technique that allows for the analysis of VOCs in low concentrations. APCI-MS has been commonly used for the analysis of food volatiles during digestion [41], but has yet to be widely explored for disease VOCs.
2.1. SubjectsThe study cohort was recruited based on inclusion in one of two groups: patients with clinically diagnosed silicosis, and healthy controls without documented lung disorders. Patients with a diagnosis of silicosis were recruited prospectively from specialist clinical practice at Holdsworth House Medical Practice (HHMP), Sydney, NSW. The diagnosis of silicosis was made according to acknowledged criteria (Australian National Dust Diseases Taskforce 2022 [11, 42]) involving information from exposure history and respiratory symptoms questionnaires, complete lung function testing, chest x-ray, and often high resolution CT scan and blood tests. The disease severity was stratified into either simple silicosis or complicated silicosis, based on the size, extent and location of scar tissue in the lungs as determined from chest x-ray and/or CT scans. Both simple and complicated silicosis samples were used in the study to enable identification of biomarkers relevant across different stages, as some individuals are diagnosed with complicated silicosis without prior diagnosis of simple silicosis. Control patients were recruited prospectively from both HHMP and The University of New South Wales. Control patients had no respiratory conditions and had no previous crystalline silica exposure, and were chosen to ensure age and gender match with silicosis patients. The demographic characteristics, smoking status, medical history and silica exposure history was recorded for all participants. The study was approved by the University of New South Wales Human Research Ethics Committee (HC2203367) in accordance with the National Statement on Ethical Conduct in Human Research (2007) requirements. Written informed consent was received from all participants.
2.2. Pulmonary function testingPulmonary function was assessed via spirometry for all (31) silicosis participants as part of their routine medical care around the time of the breath sampling. Lung function parameters including forced vital capacity (FVC), forced expiratory volume in one second (FEV1), diffusing capacity for carbon monoxide (DLCO) and total lung capacity (TLC) were measured using an EasyOne Pro (ndd Medical Technologies). All spirometric tests were performed by qualified practitioners following American Thoracic Society (ATS) guidelines. Fractional exhaled nitric oxide (FeNO) readings were obtained for 24 silicosis participants, following ATS guidelines, including the use of nose clips [43]. The following was the reference range for normal lung function [44–46]: FVC: greater than 80% predicted, FEV1: greater than 80% predicted, FEV1/FVC ratio: greater than 0.7, TLC: greater than 80% predicted, DLCO: greater than 60% predicted, FeNO: less than 25 ppb.
2.3. Breath samplingBreath samples were collected from participants using a 1 l Tedlar bag (Merck Life Science, Australia) fitted with a 0.25" outer diameter tube and threaded valve for sampling. Participants were instructed to rinse their mouths with water prior to sample collection and provide late expiratory breath by exhaling excess inspired air and the lung tidal volume and then filling the Tedlar bag with any remaining air from the lungs (functional residual capacity). This process was repeated until the bag was ∼80% full.
Unlike in FeNO sampling, nose clips were not used, as the method of late expiratory breath collection discards the initial breath portion that contains dead-space and nose air that contain the majority of exogenous VOCs. This is consistent with many breath VOC sampling protocols in the literature [47]. Participants were not required to fast before breath sampling. However, data on recent food and drink intake, smoking, and exercise were collected via a questionnaire to assess potential variability. All breath samples were collected in the same clinical setting using identical consumables and analytical conditions to ensure uniform background air composition across both silicosis patients and healthy controls. This minimizes the potential influence of environmental VOCs on classification.
Samples were stored at room temperature in a dark environment until analysis. A 10 minute heated preconditioning at 40 °C was used immediately prior to analysis to re-vaporize any condensed VOCs. All samples were analyzed on the same day as collection with a maximum time between collection and analysis of six hours.
2.4. Mass spectrometryBreath samples were analyzed by APCI-MS using a custom-made APCI source consisting of a Teflon tube with a high-voltage needle that was equipped to the inlet of a linear trap quadrupole MS (LTQ-XL, Thermo Fisher Scientific). Samples were infused into the APCI-MS at a flow rate of 420 ml min−1. Mass spectra were obtained in positive ionization mode by applying potentials of +3.6 kV, 0 V, and +26 V to the corona discharge needle, capillary inlet and tube lens respectively. The capillary inlet temperature was set to 400 °C. Spectra were acquired using a mass range of 50–600 m/z for 90 s per sample. For each sample, the spectra were averaged over 60 s, exported as nominal mass, and normalized to the base peak to obtain relative peak abundances as input for ML algorithms to assess diagnostic performance.
2.5. MLThe APCI-MS breath data was used as input for analysis by six supervised ML algorithms (NN, XGB, logistic regression (LR), random forest (RF), linear discriminant analysis (LDA), and support vector machine (SVM)) to classify persons with silicosis from healthy controls. This was implemented using CRANK-MS [39] in Python (v. 3.8) to determine the diagnostic performance of ML algorithms for binary classification. The hyperparameters for each algorithm were optimized using the grid search script in CRANK-MS [39] (table S1). The results from the ML algorithms were interpreted using SHAP analysis to determine the contribution of each feature to the model prediction [39, 40].
2.6. Performance metricsFor each algorithm, a bootstrap model was used in which the data set was split randomly 100 times into 60% training data and 40% validation data (i.e. 100 'bootstraps'). Each diagnostic performance metric was calculated based on the mean of the 100 bootstrap measurements, and error was calculated as one standard deviation of the mean. For each ML algorithm, accuracy, precision/positive predictive value (PPV), sensitivity/recall (SN), specificity (SP), F1 score, Matthews correlation coefficient (MCC), and negative predictive value (NPV) were calculated using equations (1)–(7):







where TP, TN, FP and FN correspond to true positive, true negative, false positive and false negative respectively. Receiver operating characteristic (ROC) and precision-recall (PR) curves were generated and used to calculate area-under-curve (AUC). Briefly, an ROC curve is a plot of the sensitivity against the specificity, and a PR curve is a plot of the precision rate against the sensitivity. These curves are beneficial as they allow for a visual representation of the trade off that often exists between performance metrics, and the area under these curves represent a summary of the model performance. ROC curves are generally more informative when the two classes are balanced in number, and PR curves are preferred when there is an imbalance.
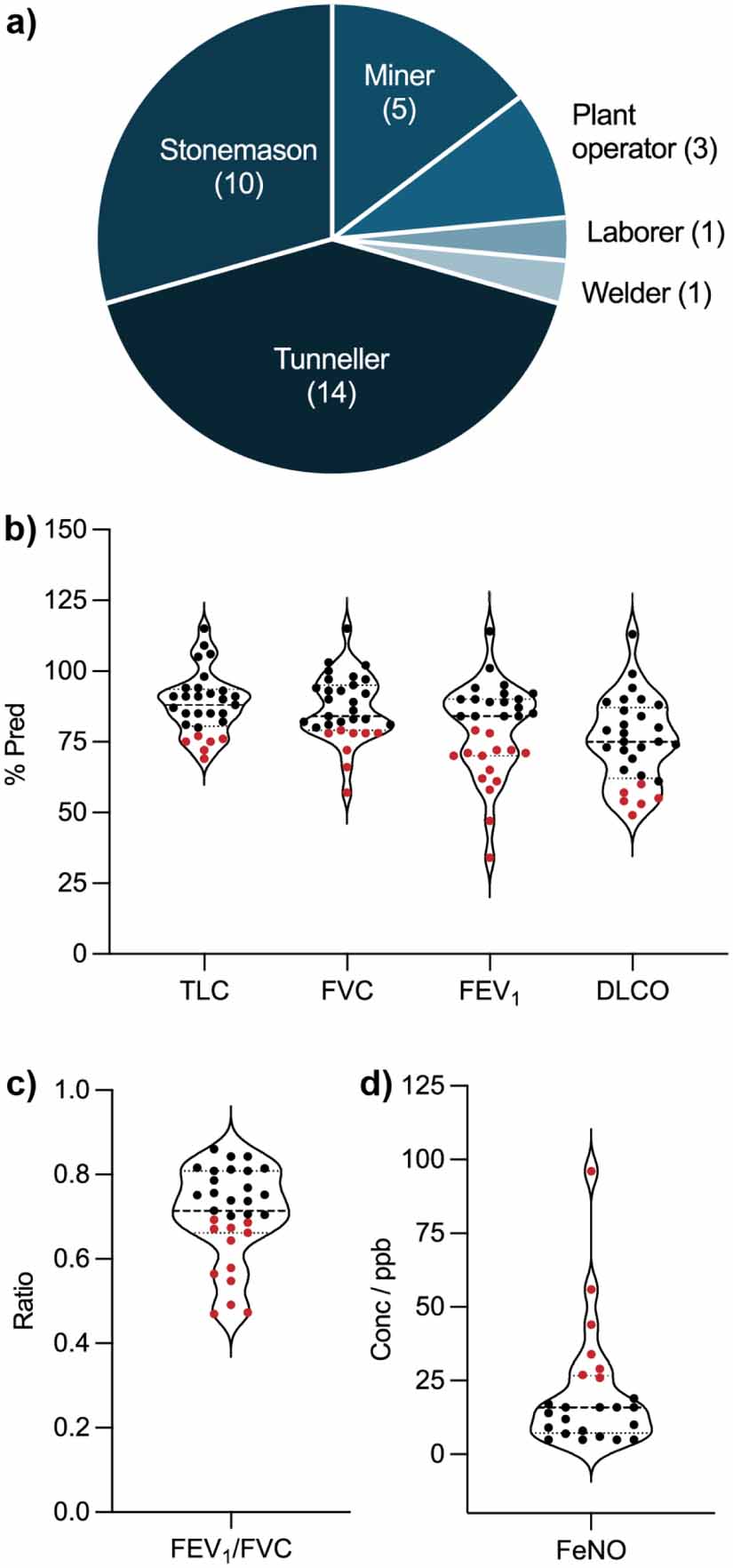
A total of 91 patients were recruited for this study and consisted of adult males aged 36–79. The study cohort comprised of two groups: 31 patients with clinically diagnosed silicosis, and 60 healthy controls without any documented lung disorders. The demographics of the silicosis and control groups are summarized in table 1. There were no statistically significant differences between the groups for age and gender. However, the silicosis group exhibited a higher prevalence of comorbidities, including hypertension, heart disease, and diabetes (42% of the silicosis group compared to 12% of the control group), as well as other lung diseases (48% of the silicosis group and 0% of controls, by definition). Additionally, the silicosis group had a higher proportion of both current smokers (23% of the silicosis group compared to 8% of the control group) and ex-smokers (52% of the silicosis group compared to 12% of the control group). Among the silicosis group, 24 participants had simple silicosis, while 7 had the more severe, complicated form. Seventy-seven percent of the silicosis group had been exposed to silica through their occupations as stonemasons or tunnelers, while the remaining participants had been exposed through other professions, such as mining, welding, laboring, and plant operations (figure 1(a)). Spirometry, diffusion, and FeNO measurements for the silicosis group showed normal readings for most participants (55%–79%, figures 1(b)–(d)), suggesting that most cases were not yet severe enough to cause significant functional impairment. For factors that could affect breath variability, a subset of participants (30% of silicosis patients and 40% of healthy controls) reported eating or drinking within two hours prior to sampling. Additionally, 10% of silicosis patients and 20% of healthy controls reported engaging in physical activity within the previous 24 h. No participants in either group reported smoking within two hours prior to sampling.
Figure 1. Silicosis group spirometry, diffusion and occupation data. Panel (a) represents an occupation breakdown for the silicosis patients, noting that three participants worked in multiple industries. Panel (b) represents total lung capacity (TLC), forced vital capacity (FVC), forced expiratory volume in one second (FEV1) and diffusing capacity for carbon monoxide (DLCO) as a percentage of predicted. Panels (c) and (d) represent the FEV1/FVC ratio and fractional exhaled nitric oxide (FeNO), respectively. For panels (b)–(d), data points in black indicate a normal reading and points in red indicate an abnormal reading [44–46].
Download figure:
Standard image High-resolution imageTable 1. Summary of patient demographics.
CharacteristicSilicosisHealthy controlNumber3160Silicosis category simple24N/A complicated7 Average agea51 ± 1251 ± 11Gender (% male)100100Smoking status Non-smokers748 Ex-smokers167 Current smokers75 Vape users3b8cComorbiditiesd Hypertension77 Heart disease52 Diabetes23 Liver disease00 None of the above1853Other lung diseasese Asthma50 COPD80 Emphysema30 Latent tuberculosis20 Sleep apnoea20 Hypersensitivity pneumonitis10 Chronic pneumothorax10 Chronic bronchitis10 None1660a±1 standard deviation. bAll three vape users are also in the ex-smoker category. cThree vape users also currently smoke, and the other five vape users have never smoked. dThree people in the silicosis group and five in the control group had multiple comorbidities. eSeven people in the silicosis group had multiple other lung diseases.COPD = chronic obstructive pulmonary disease.
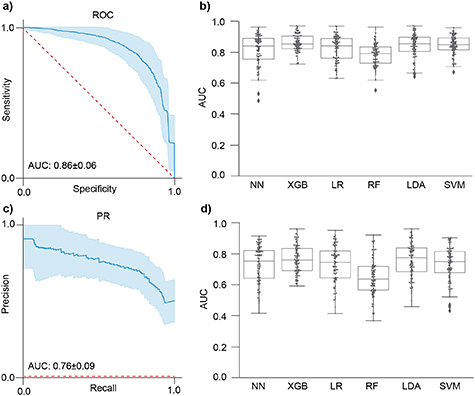
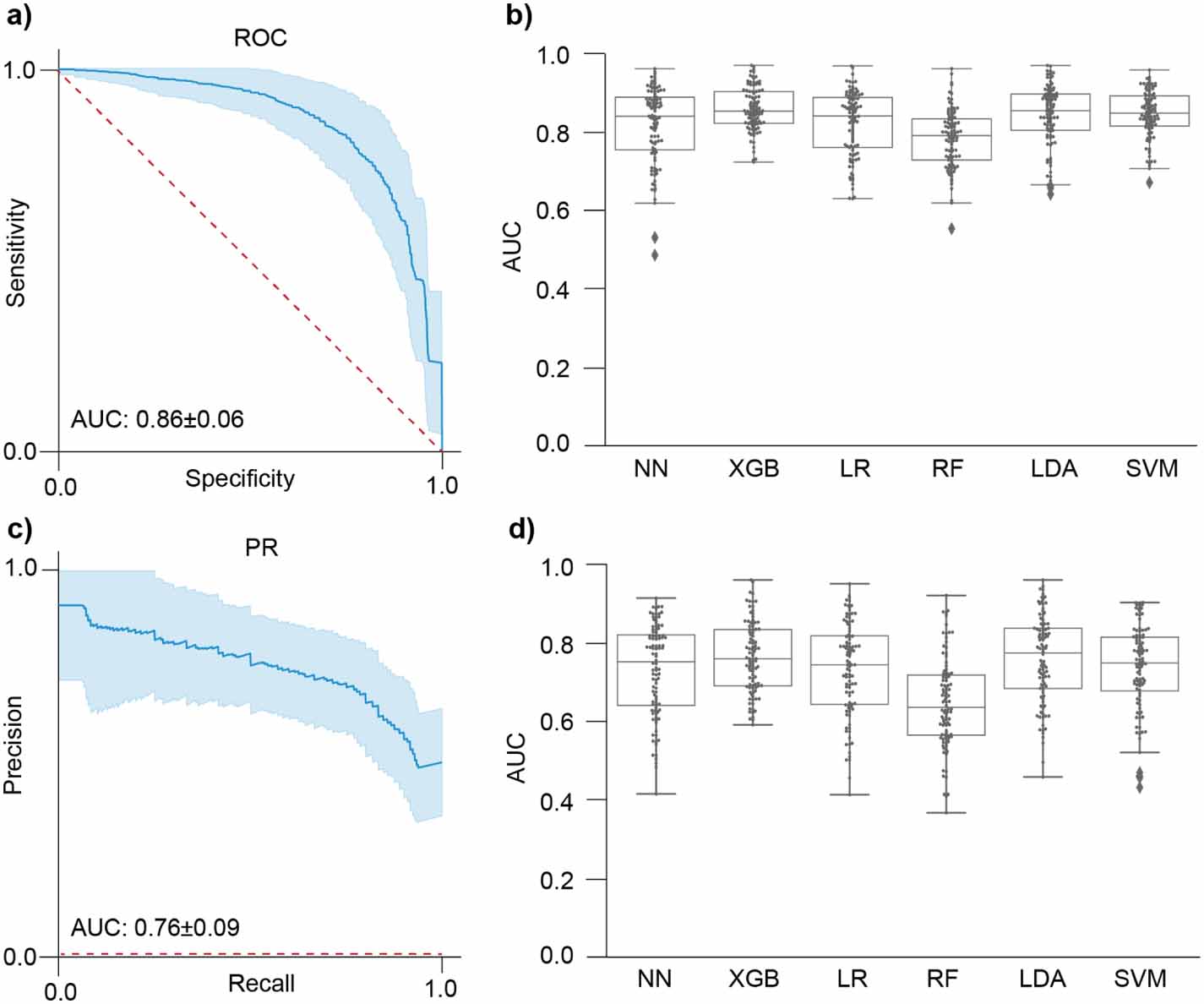
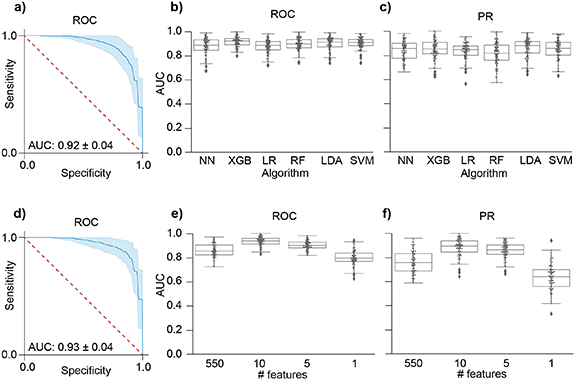
The APCI-MS data from 50 to 600 m/z was analyzed using six ML algorithms to assess their diagnostic performance in classifying silicosis and healthy control samples. Among the evaluated algorithms, the XGB, LDA and SVM classifiers exhibited the highest overall performances that were statistically equivalent for both AUC (ROC) and AUC (PR) metrics. The XGB, LDA and SVM classifiers achieved AUC (ROC) values of 0.858 ± 0.055, 0.843 ± 0.078 and 0.845 ± 0.061, respectively (PXGB−LDA = 0.127, PXGB−SVM = 0.106, PLDA−SVM = 0.895), and an AUC (PR) of 0.760 ± 0.090, 0.756 ± 0.081 and 0.733 ± 0.110, respectively (PXGB−LDA = 0.745, PXGB−SVM = 0.057, PLDA−SVM = 0.151) (figure 2, table S2). The performance of the remaining algorithms was also robust, with five out of the six classifiers obtaining an AUC (ROC) above 0.8 (figure 2, table S2).
Figure 2. Performance of six machine learning algorithms for the classification of silicosis from healthy controls using APCI-MS data without any feature selection. Receiver-operating characteristic (ROC) curve (a) and precision recall (PR) curve (c) for XGB are shown with a 95% CI in blue, and a dotted red line representative of an algorithm with no predictive power. The performance of the six machine learning algorithms is compared through swarm plots of the area under the curve (AUC) for ROC curves (b) and PR curves (d), with points representing each of 100 bootstraps performed for each of the algorithms: neural networks (NN), extreme gradient boost (XGB), logistic regression (LR), random forest (RF), linear discriminant analysis (LDA) and support vector machine (SVM).
Download figure:
Standard image High-resolution imageThe MCC score was highest for the XGB and LR classifiers with normalized scores of 0.764 ± 0.178, and 0.760 ± 0.189, respectively (P = 0.878) (table S2). MCC is recognized as a more informative metric for binary classification, particularly in datasets with an imbalance in the size of the cohorts [48]. Other classifiers, including LDA and SVM, demonstrated lower MCC scores of, 0.749 ± 0.224, and 0.742 ± 0.204, respectively (table S2) that were statistically lower (P < 0.05) than XGB and LR classifiers. In terms of the NPV, the XGB, LR and SVM classifiers performed the best with statistically equivalent NPV scores of 0.814 ± 0.079, 0.823 ± 0.071, and 0.810 ± 0.080, respectively (PXGB−LR = 0.435, PXGB−SVM = 0.772, PLR−SVM = 0.225) (table S2). NPV is clinically important because it assesses the likelihood that subjects who receive a negative test result are truly healthy, thereby helping to minimize unnecessary follow-up tests. For all six algorithms, randomly permuting the silicosis and healthy data labels resulted in average accuracies that are statistically the same as 50% within one standard deviation (figure S1), consistent with a 'random guess' for binary classification as expected for this control test.
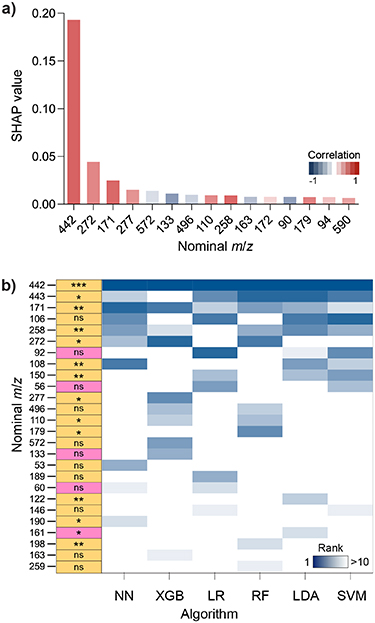
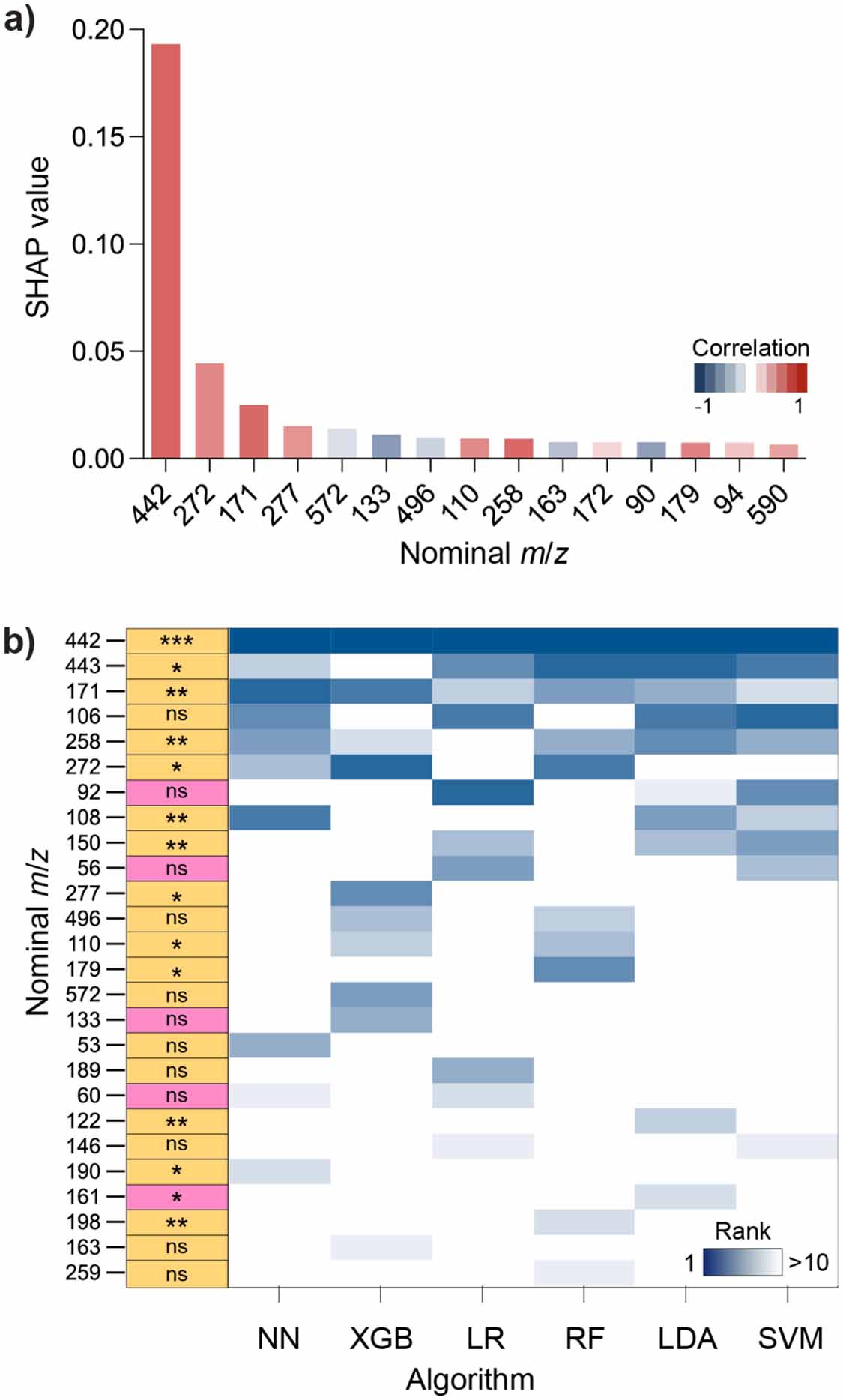
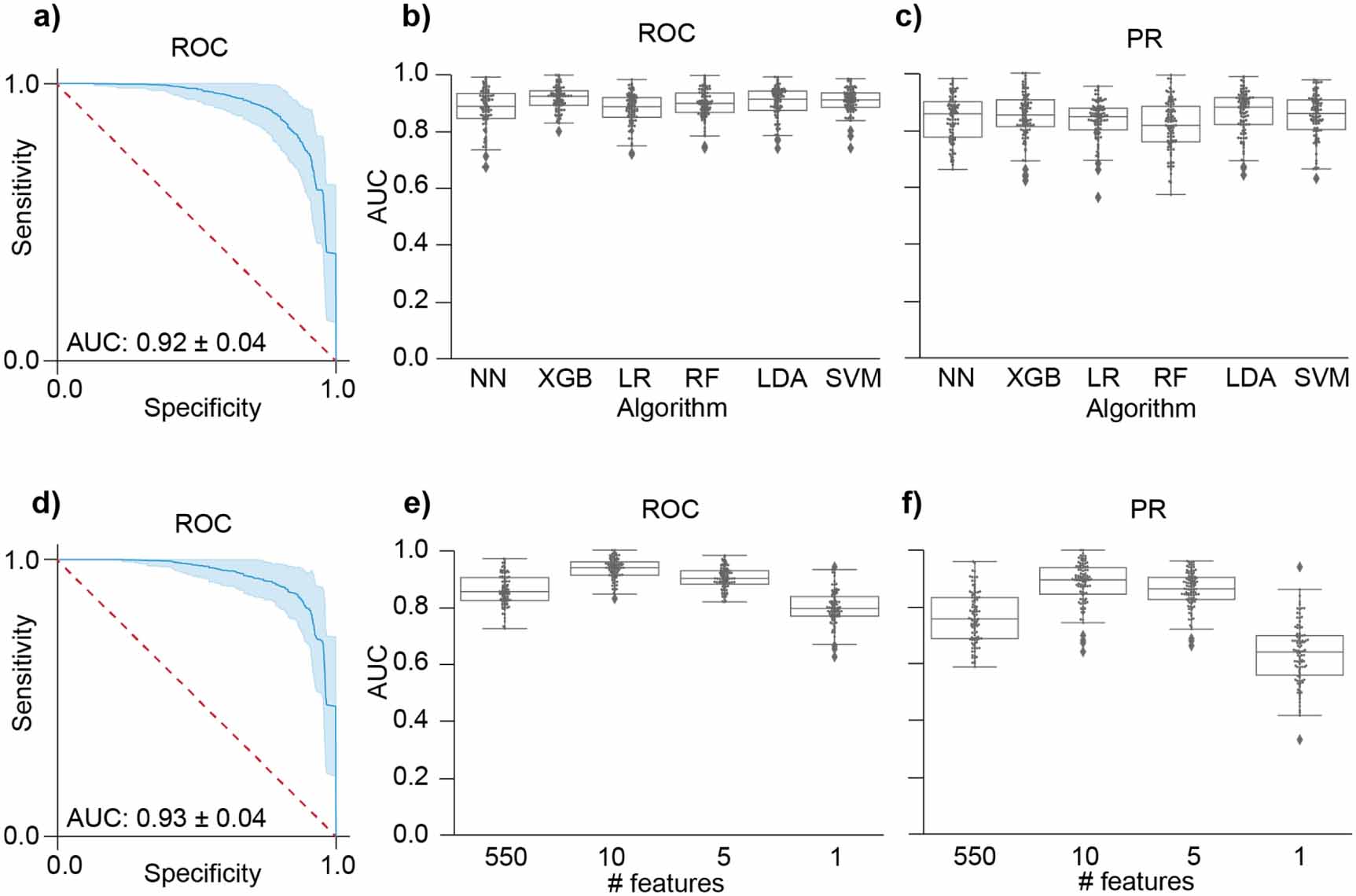
To further investigate the contribution of specific features to the classification performance, SHAP analysis was conducted, revealing that the feature at m/z 442 was the most significant predictor across all six algorithms (figure 3). The m/z 442 feature intensity was statistically significant between the silicosis and control groups with a p-value of 2 × 10−4 (figure S2, table S3). Additional SHAP features, including ions at m/z 272, 171, and 277, also contributed to the model predictions, though to a lesser extent (figure 3). When the ML algorithms were applied to a reduced dataset containing only the top 26 SHAP features, an improvement in diagnostic performance was observed across all algorithms (figures 4(a)–(c), table S2), with the XGB and SVM classifiers achieving equivalent AUC (ROC) values of 0.917 ± 0.042 and 0.911 ± 0.042, respectively (P = 0.275). Further reduction of the feature set to the top ten SHAP features resulted in the highest performance metrics, with the XGB classifier achieving an AUC (ROC) of 0.933 ± 0.038, an AUC (PR) of 0.882 ± 0.073, a normalized MCC score of 0.852 ± 0.126 and a NPV of 0.879 ± 0.069 (figures 4(d)–(f), table S4). Feature reduction to the top five features and top one feature did not further improve the predictive performance, with AUC (ROC) values of 0.901 ± 0.039 and 0.798 ± 0.060, and AUC (PR) values of 0.859 ± 0.064 and 0.634 ± 0.107, for five and one feature/s, respectively (figures 4(d)–(f), table S4).
Figure 3. Key nominal m/z values from APCI-MS analysis of breath used in algorithm predictions. Panel (a) shows Shapley additive explanations (SHAP) values for the top 15 ions (nominal m/z) that had the highest contribution to a correct silicosis prediction using the XGB classifier. The average correlation corresponds to whether the feature is greater in intensity (red) or lower in intensity (blue) in silicosis samples. Panel (b) shows comparative SHAP rankings for the top 10 metabolites for all six algorithms with the first column summarizing statistical analysis of the features including p-value (P < 0.0001 = ***, P < 0.001 = **, P < 0.05 = * and P > 0.05 = not significant (ns)) and fold change relative to healthy (yellow = higher intensity in silicosis, pink = higher intensity in healthy).
Download figure:
Standard image High-resolution imageFigure 4. Using a feature-selected model based on SHAP rank increased the performance of all algorithms with XGB remaining the best performing classifier. Panels (a)–(c) represent algorithm performance using the combined top 10 SHAP features from all algorithms (26 features total), with (a) showing the ROC curve for XGB classifier, and (b) and (c) showing comparative swarm plots of the AUC for ROC curves and PR curves, respectively. Panels (d)–(f) represent a comparison of the performance of XGB with differing number of features. The ROC curve for the XGB classifier using the top 10 SHAP features is shown in (a), and comparative swarm plots of AUC for ROC and PR curves for differing numbers of input features are shown in (e) and (f), respectively.
Download figure:
Standard image High-resolution imageThis study aimed to evaluate the diagnostic performance of various ML algorithms in classifying silicosis and healthy control samples using non-invasive breath sampling coupled with a rapid VOC fingerprinting test through APCI-MS, rather than targeting specific VOCs. The results demonstrated that the XGB classifier performed consistently highly across most performance metrics, particularly in terms of ROC and PR AUC values, normalized MCC score and NPV score (0.933 ± 0.038, 0.882 ± 0.073, 0.852 ± 0.126 and 0.850 ± 0.070, respectively using the top ten SHAP features). These findings suggest that the overall approach, particularly when using the XGB classifier, can be highly effective in facilitating the rapid and accurate diagnosis of silicosis, owing to its ability to account for complex patterns in the VOC data that may not be readily apparent with alternative methods.
Breath tests have emerged as a promising non-invasive tool for diagnosing various respiratory conditions, including OLDs [27, 49, 50], Most of the current research in this area has relied on gas chromatography-mass spectrometry (GC-MS) to identify VOCs in exhaled breath that can serve as biomarkers for these diseases. While GC-MS is highly sensitive and capable of detailed chemical analysis, it typically involves long analysis times, making it less practical for large-scale screening efforts. For COPD, studies using GC-MS have shown that specific VOC profiles can differentiate between disease stages [24] and even predict exacerbations [51]. Similarly, breath analysis in asbestosis has identified compounds linked to lung inflammation and fibrosis [26], though the specificity of these biomarkers remains a challenge. Despite these advances, only two studies to date have examined the potential of breath analysis for silicosis diagnosis [28, 29]. Both studies used solid phase microextraction (SPME) GC-MS for analysis. One study from 2016 only included four silicosis participants, and hence could not make conclusions on the diagnostic performance of the identified potential biomarkers [29]. A study from 2023 with greater patient numbers also identified potential biomarkers using orthogonal partial least squares discriminant analysis, obtaining a sensitivity and specificity of 60.3% and 89.2% [28]. While the use of SPME-GC-MS is beneficial in allowing for more detailed compound identification, the total extraction and run time for each sample is 95 min, which presents a challenge for using it widely as a screening tool. For example, Coal Services Australia conducted nearly 9792 screening tests in the 2022–23 reporting year [52], which would require over 15 500 h of sampling processing and instrument time if exhaled breath analysis was included in the screening process.
The approach used in this study, utilizing APCI-MS, offers a significant advantage with an analysis time of less than two minutes and no preconcentration is required. This rapid analysis opens the possibility of its application in larger-scale screening including routine respiratory surveillance, which is particularly relevant for silicosis given its irreversible nature and lack of effective treatments. Early and accurate diagnosis through such a test could be crucial in early diagnosis and prevention of disease progression by removal from further exposure, also potentially reducing the reliance on invasive procedures. However, further confirmation of specificity and sensitivity is required in a prospective double-blind study using larger numbers of participants.
This study represents a potential advance in respiratory disease diagnostics, as it is the first example in the literature of a rapid, non-invasive breath test for silicosis that is feasible for large-scale screening. These results were obtained using breath that had been stored in Tedlar bags for up to six hours. Previous studies have demonstrated the loss of sample complexity after as little as 10 min due to interactions with, and losses through the bag material [53–55]. However, our results show that despite potential losses of some VOCs, the remaining sample still contains relevant information for silicosis diagnosis. While no fasting period was enforced before breath sampling, questionnaire data indicated that food and drink intake was more common among healthy controls than silicosis patients (40% vs. 30%). This suggests that any dietary-related variability is unlikely to have introduced systematic bias favoring disease classification. Similarly, physical activity within the previous 24 h was more common among controls than silicosis patients (20% vs. 10%), though specific data for the 2 h period before sampling were unavailable. Future studies could explore the potential impact of these factors in more detail. By leveraging advanced ML algorithms to analyze breath VOC profiles obtained through APCI-MS and using this method in addition to conventional testing, this research suggests that exhaled breath profiling could represent promising rapid and non-invasive biomarker analysis to facilitate the diagnosis of silicosis. This could potentially overcome current diagnostic limitations including the low sensitivity of radiography modalities [13, 56], and of pulmonary function tests with reported PPVs of 41%–58% [57]. which was similarly observed in this study where 55%–79% of spirometry and diffusion measures were in the normal range for silicosis participants.
The APCI process used for sample analysis results in the formation of protonated monomers [M + H]+, with a nominal neutral mass of 441 Da corresponding to the 442 m/z feature, tentatively assigned to leukotriene-E3 (LTE3), a molecule with an exact mass of 441.25 Da. While leukotrienes, including LTE4, LTD4, and LTB4, are well-established markers in obstructive lung diseases such as asthma [58] and COPD [59] their presence in restrictive lung diseases like silicosis has been less explored. Recent evidence suggests that leukotrienes could play a role in fibrotic lung diseases through their involvement in inflammatory signalling pathways. Elevated levels of LTE4 and LTD4 have been observed in pneumoconiosis linked to asbestos and silica exposure [60]. Given the inflammatory nature of silicosis, driven largely by the NLRP3 inflammasome, it is plausible that leukotrienes, which are potent mediators of inflammation, could also be involved in the disease process [61]. Leukotriene antagonists, commonly used in asthma, are not typically applied in silicosis, as this disease involves different inflammatory pathways, particularly those regulated by the NLRP3 inflammasome rather than leukotriene-mediated mechanisms. [62, 63]. Thus, its potential as a biomarker for silicosis and an understanding of its interaction with NLRP3-mediated inflammation should be further explored.
4.1. LimitationsWhile the results are promising, several limitations are acknowledged. First, the study's sample size is relatively small, and expanding the population to include a broader range of lung conditions and stages of silicosis is necessary. This is particularly important for differentiating silicosis from other similar respiratory conditions such as interstitial pulmonary fibrosis [64] and sarcoidosis [65], which often present overlapping symptoms. Differentiating these diseases is crucial because they may require distinct treatment approaches, and misdiagnosis can lead to inappropriate therapies, particularly for future therapies that are currently in the development pipeline [64]. The results from this study demonstrate the feasibility of distinguishing silicosis patients from healthy controls, providing a foundation for further investigation. Healthy controls were selected to establish a biomarker baseline in the absence of exposure-related effects. Some biomarkers may be linked to exposure rather than disease. To address this, our next study will focus on silica-exposed individuals who have not been diagnosed at the time of sampling and will include those with other confounding respiratory conditions (e.g. COPD). This will allow us to assess whether our approach can differentiate silicosis from other lung diseases and determine its potential for early detection. Second, unambiguous identification of the detected biomarkers requires further validation. Higher-resolution mass spectrometry and ion fragmentation data, supported by authentic standards, are essential to accurately pinpoint the biomarkers specific to silicosis. This step is critical to confirm the findings and enhance the reliability of these potential diagnostic markers. Future studies should aim to address these gaps to refine the diagnostic utility of the identified biomarkers for silicosis.
This study provides early evidence for the potential of exhaled breath analysis using APCI-MS as a rapid, non-invasive diagnostic tool for silicosis. The VOC measurement takes less than two minutes per sample and does not require a preconcentration sample processing step, making it a promising candidate for large population screening, offering a significant advantage over methods that are invasive and time-consuming particularly in at-risk occupational groups. The interpretability of the ML models, made possible through SHAP provides a transparent way to understand how each feature contributes to the model's predictions, ensuring that the diagnostic results can be interpreted. For example, the analysis identified the m/z 442 feature as a significant predictor across multiple ML models, which potentially corresponds to leukotriene-E3, a molecule from a class that has been previously linked to lung inflammation. This finding suggests that the m/z 442 feature could serve as a biomarker for silicosis, although further validation is required to confirm its role. This research highlights the potential of breath-based diagnostics, particularly when combined with interpretable ML, to advance silicosis diagnosis and potentially improve patient outcomes.
This work
Comments (0)