
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Remember me
Early detection is critical for lung cancer patients. One lung cancer detection method under study is using sniffer dogs. This study aimed to evaluate, retrospectively, the sensitivity and specificity of the Cancer Detection Dog Collective (CDDC®) method under training conditions. A team of five trained sniffer dogs analyzed breath samples from lung cancer patients and cancer-free volunteers, and a cancer sample is positive if at least three dogs indicate it. Dog handlers and experimental observers were blinded to sample identity, and detection accuracy was assessed. Primary endpoint was sensitivity, and specificity and confounding factors were also assessed. Samples were collected in 2024 from 824 volunteers, including 111 with a confirmed diagnosis of lung cancer (mean age 60, range 34–80, 18% early-stage cancer, 46% not yet oncological treated). A total of 11 900 breath samples were tested with 125 test runs per dog. Each of the five dogs demonstrated a detection performance with a sensitivity between 82% and 89%, a specificity over 95%, and an accuracy over 94%. The CDDC® dog team’s corporate decision revealed a sensitivity of at least 95.5%. The cancer-free volunteers were primarily young, healthy individuals. According to the CDDC® decision rules, none of these control samples were identified as false positives by more than two dogs. Analysis of potential confounding factors revealed that weather conditions and supervisor skills were associated with the dogs’ performance. The CDDC® method showed high consistency in training scenarios. Further studies should evaluate this method in a controlled clinical study alongside lung cancer screening.
Export citation and abstractBibTeXRIS
Lung cancer is still the leading cause of cancer death worldwide. Late detection contributes to poor treatment outcomes, and the early detection of lung cancer continues to be a challenge [1]. Studies have shown that lifestyle changes, such as quitting smoking, can significantly reduce cancer-specific mortality in lung cancer survivors [2]. For smokers, quitting remains the most effective way to prevent cancer and cardiovascular disease [3]. Reducing the lung cancer mortality rate may be possible through the early detection of the cancer in high-risk individuals using low-dose computed tomography (LDCT). Many countries are making progress in establishing national screening programs [4]. However, lung cancer screening with LDCT can result in false positive (FP) test results, leading to stressful examinations for screened individuals [5]. Another innovative approach is training animals to detect cancer. This method has demonstrated promising results [6]. The use of the dog’s sense of smell is well known, researched, and published [7–9]. Published studies have reported a sensitivity of 78% and a specificity of 71.5% for the detection of lung cancer by sniffer dogs in breath and urine samples [10–13]. The exact chemical compounds or combinations of compounds that dogs sniff that indicate lung cancer have not been determined. It has also not yet been confirmed whether dogs can detect early, preclinical stages of cancer with comparable accuracy to already diagnosed cases [9]. A total of 62 studies were analyzed in a meta-analysis review [14], but the available studies showed a very heterogeneous picture with regard to study quality. The risk of bias in the studies was often high, resulting in low-quality evidence. In a double-blind clinical study using breath and urine samples, the dogs identified 40 of 41 lung cancer samples from a total of 246 patients, corresponding to an overall detection rate of 97.6% [15]. Another study found that using exhaled breath for training sniffer dogs is more sensitive and specific than using urine or tissue samples [16]. This training method had a 91.7% sensitivity and an 85.1% specificity [16]. In another review, it was concluded that medical scent canines could be comparable in sensitivity to LDCT lung cancer screening, and may even have a high specificity [17]. Further refinement of this research could eventually result in the implementation of this sniffer dog method for early lung cancer detection in the future.
In present evaluation, a newly refined Cancer Detection Dog Collective (CDDC®) method was evaluated, with the aim of optimizing breath sampling for ease of use and reproducibility. To increase the detection rate, the results of previously published methods [10, 11] were considered and optimized so that the CDDC® method includes five independent test runs with five different dogs.
The aim of this retrospective evaluation was to determine the sensitivity and specificity of the CDDC® test under training conditions.
2.1. Study designThis was a retrospective evaluation of a dog-based cancer detection procedure. Positive breath samples from lung cancer patients and negative breath samples from presumably healthy persons were used for all the training runs. Lung cancer patients were recruited from various hospitals in Germany. Written informed consent was obtained from all subjects, who provided clinical lung cancer diagnoses and breath samples for research purposes. No compensation was given to the subjects who provided breath samples. All animal-training and -handling methods were designed in consultation with veterinarians, dog trainers, and dog owners. All procedures were carried out by Dogscan GmbH in Erkelenz, Germany (Dogscan-deutschland.de). Ethical approval for the retrospective evaluation and analysis of the anonymized data was obtained from the ethics committee of Charité—Universitätsmedizin Berlin (EA1/111/25) on 22.05.2025.
2.2. Sample collectionBetween January and September 2024, breath samples of 824 volunteers were collected at multiple locations in Germany. The breath samples from lung cancer patients were clinically confirmed and provided by lung cancer centers and hospitals, including Luisenhospital Aachen and Elisabeth-Hospital of the Städtische Kliniken Mönchengladbach, as well as other oncology or pulmonology specialist practices in Germany. Volunteers without lung cancer were recruited from among students, as well as from people with preexisting respiratory diseases for whom lung cancer had been ruled out by clinical examination. All participants signed a consent form agreeing to provide breath samples and make their data available. The use of fleece masks for sampling exhaled volatile organic compounds has been recommended for canine scent tests [18]. Here, we used certified (Article 2, No. 3 of Regulation (EU) 2017/746 (IVDR)) breathing masks (100% cotton, OEKO-TEX® Standard 100, Product Class I (Baby Class), with integrated absorbers (100% cotton) for aerosols. Each participant was instructed to wear the mask for five consecutive minutes, breathing out exclusively through their mouth. All breath samples were collected outdoors, away from medical treatment rooms, and in a non-sterile environment with ambient odors. Afterwards, the masks were immediately sealed in an airtight foil bag and shipped individually via regular mail to the testing facility. There, the breath samples were stored at an ambient temperature between 10 °C and 30 °C. The masks were analyzed within a maximum of three weeks of being worn.
2.3. The CDDC® decision rulesHit rates vary among dogs, so a ‘corporate decision’ strategy involving multiple dogs was proposed to improve sensitivity [11]. The CDDC® method involves conducting the test runs in five separate rounds, each with a different trained sniffer dog. After the five test runs, the results are evaluated according to the following decision rules. The first CDDC® decision rule states that at least three out of five dogs must identify the breath sample as a true positive (TP). The second CDDC® decision rule, to reduce FPs, requires all five dogs to identify negative samples as true negatives (TNs). The third CDDC® decision rule is that if the dogs disagree and only one or two indicate the breath sample as positive, then the result is inconclusive and a new breath sample must be taken until a conclusive classification can be made.
2.4. Dog training, testing and detection procedureFamily dogs were trained by professional dog trainers with experience in scent detection. Sniffer dog training protocols were adapted from other studies [10] and optimized for the present setting. Similar to what is described by others [10, 15–17], young puppies were trained in several stages to recognize and indicate breath samples from lung cancer patients. From the start of their training, the dogs are trained and tested using control samples with strong, distracting odors, such as food, smoke, or cosmetics, to ensure they can detect the target odor specifically. During the last stage, training focuses on preventing the dogs from developing recognizable patterns. This is achieved by varying the positions of the target samples, the ratio of positive to negative samples, the use of multiple fresh samples from different donors, sampled at various locations, and the use of different misleading masks to prevent misconditioning. Positive breath samples from lung cancer patients with clinically confirmed diagnoses (various stages, histologies, and molecular pathologies) were also used for the training and education of the sniffer dogs. Methodological standards for olfactory detection trials were followed as recommended [9] and the performance of the dogs was verified by a rigorous double-blind (dog and dog handler) procedure. All of the sniffer dogs used here undergo extensive training and must have at least 12 months of experience in detecting lung cancer breath samples. The sniffer dogs must regularly demonstrate their detection performance and sniff out a cumulative total of 2500 samples, including 100 breath samples from individuals with a confirmed lung cancer diagnosis. The detection performance is monitored by an independent body, and the minimum requirements are sensitivity of 90% and specificity of 99.13%.
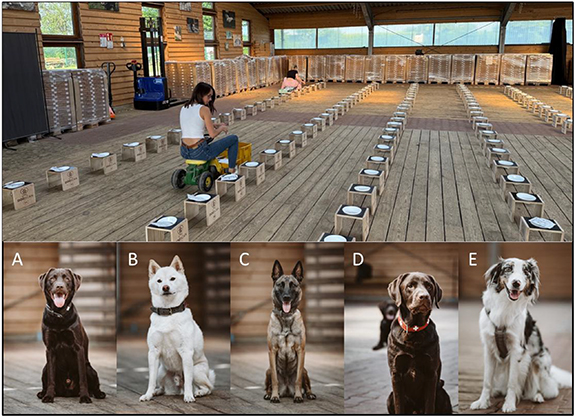
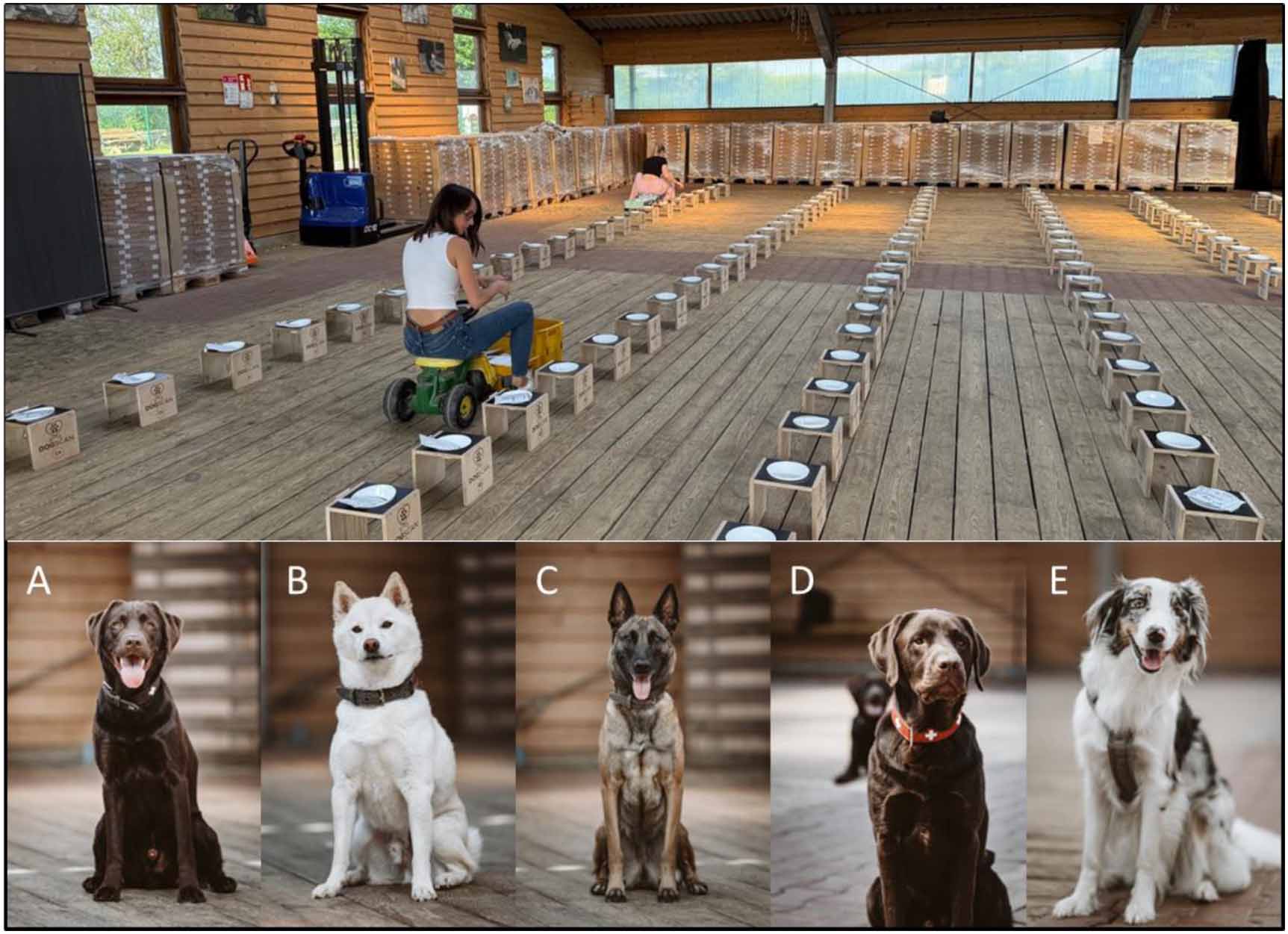
In this study, five trained sniffer dogs were used see figure 1, three of which were male and two females, with ages ranging from two to seven years. Dog training was performed in a specialized facility equipped with standardized search boards as shown in figure 1 above. Unlike previous test procedures conducted under controlled laboratory conditions, sterile search containers were not used here. Instead, numerous search boards, up to 200 were set up in a natural environment with foreign odors. The number of search boards and arrangement of samples was determined by a computer-assisted randomization algorithm (Ninox Enterprise, Customized Programming, Germany). The supervisor, who was independent of the experimental observers and dog handlers, was responsible for preparing the search layout and placing the samples. All observers and dog handlers were blinded, and the supervisor was the only person who knew where the positive and negative masks were placed. The supervisor remained at a constant distance of 8–12 m from the search boards during the search runs, standing in the same position to avoid position-related stimuli. If the searching dog indicates a mask, the respective dog handler says ‘indication,’ and if it is a positive mask the supervisor answers ‘Proband’ and the dog receives a reward. If the dog indicates a negative mask, the supervisor answers ‘misleading’ and the dog handler leads the dog on without giving a reward. In the case of an unknown evaluation sample, if the dog indicates, this is noted, the supervisor responds ‘Customer,’ and the dog handler leads the dog on without giving a reward. The supervisor documents all displayed search board numbers in the system log. Dog handlers were unaware of sample placement and the independent observers were blinded to sample status throughout the trial. For each search run, 25–200 search boards equipped with different breathing masks are set up in the test facility as shown in figure 1.
Figure 1. The Cancer Detection Dog Collective team. The test facility with search boards is shown above. Below are the five sniffer dogs used: (A) male Labrador, 2 years, (B) male, Shiba Inu, 7 years, (C) female, Belge Malinois, 4 years, (D) male, Labrador 3 years, (E) female Australian Shepherd, 3 years.
Download figure:
Standard image High-resolution imageA typical search run consists of 100 search boards, five of which are populated with lung cancer breath samples (P) and 95 of which are populated with masks from non-cancer subjects (N). A positive indication of lung cancer was defined as the dog stopping in front of a sample. A negative indication was defined as the dog running past a sample. A typical test run with 100 search boards, including five positive samples, takes about eight minutes per dog. At least two independent observers recorded and scored each dog’s indications and documented the numbers of TP, TN, FP, and false negative (FN) per run. All sniffer dogs undergo regular training, with ten to fifteen test runs each month. Fresh samples are used in these searches, and the dogs’ performance is evaluated and documented.
2.5. Statistical analysisAll statistical analyses were conducted using Python (version 3.11.3) with the following libraries: pandas, numpy, scikit-learn, statsmodels, and matplotlib. A significance threshold of p < 0.05 was applied throughout the analysis. Participant characteristics and sample distributions were summarized using descriptive statistics.
For each test run and dog, we counted TP, FPs, TN, and FN responses and performance metrics were estimated. Sensitivity is calculated as TP/P, specificity as TN/N, accuracy as (TP + TN)/(P + N), positive predicted values (PPVs) as TP/(TP + FP), and negative predicted value (NPV) as TN/(TN + FN). Exact 95% confidence intervals (CIs) for detection metrics were estimated using the Wilson score method, and corresponding confusion matrices and classification distributions were generated. Since repetitive samples from the same donors were used, corrected metrics were calculated to account for potential pseudoreplication bias. The number of FN and FP values were counted as before. The corrected sensitivity and specificity were recalculated using the number of unique subjects. P= unique number of P; N = unique number of N; Sensitivity = (P−FN)/P, Specificity = (N−FP)/N, accuracy = (P−FN + N−TN)/(P + N), PPV = (P−FN)/(P−FN + FP), and NPV = (N−FP)/(N−FP + FN).
To assess the robustness of the ensemble decision process, a simulation-based resampling procedure was implemented using a mask-by-dog detection outcome matrix. For each mask, individual dog responses were represented as binary indications (positive vs negative). For each scenario (e.g. using 2, 3, 4 or 5 dogs), subsets of dogs were randomly sampled without replacement from the observed five-dog panel. Predefined collective decision rules were then applied (e.g. mask classified as positive if ⩾ 1 of 2, ⩾ 2 of 3, or ⩾ 3 of 4 dogs indicate it). This process was repeated 5000 times per scenario. Across iterations, sensitivity, specificity, and accuracy were calculated to evaluate the stability of detection performance under different dog-team configurations.
To evaluate potential confounding variables, we fitted a generalized estimating equations (GEE) logistic regression model with a binomial family and robust standard errors. Because environmental and contextual variables (weather, ambient temperature, supervisor identity, and dog mood) were recorded once per test day and were constant across all mask evaluations within that day, the unit of analysis was defined at the dog-day level.
Individual mask-level outcomes (TP, TN, FP, FN) were first classified as correct (TP or TN) or incorrect (FP or FN). These were then aggregated for each dog and test day to calculate the proportion of correct classifications. A binary outcome variable was defined, where a dog-day was considered successful if ⩾90% of classifications were correct. The GEE model estimated the probability of a successful dog-day as a function of dog mood, weather conditions, ambient temperature, and supervisor identity, while accounting for repeated observations within dogs by clustering on dog.
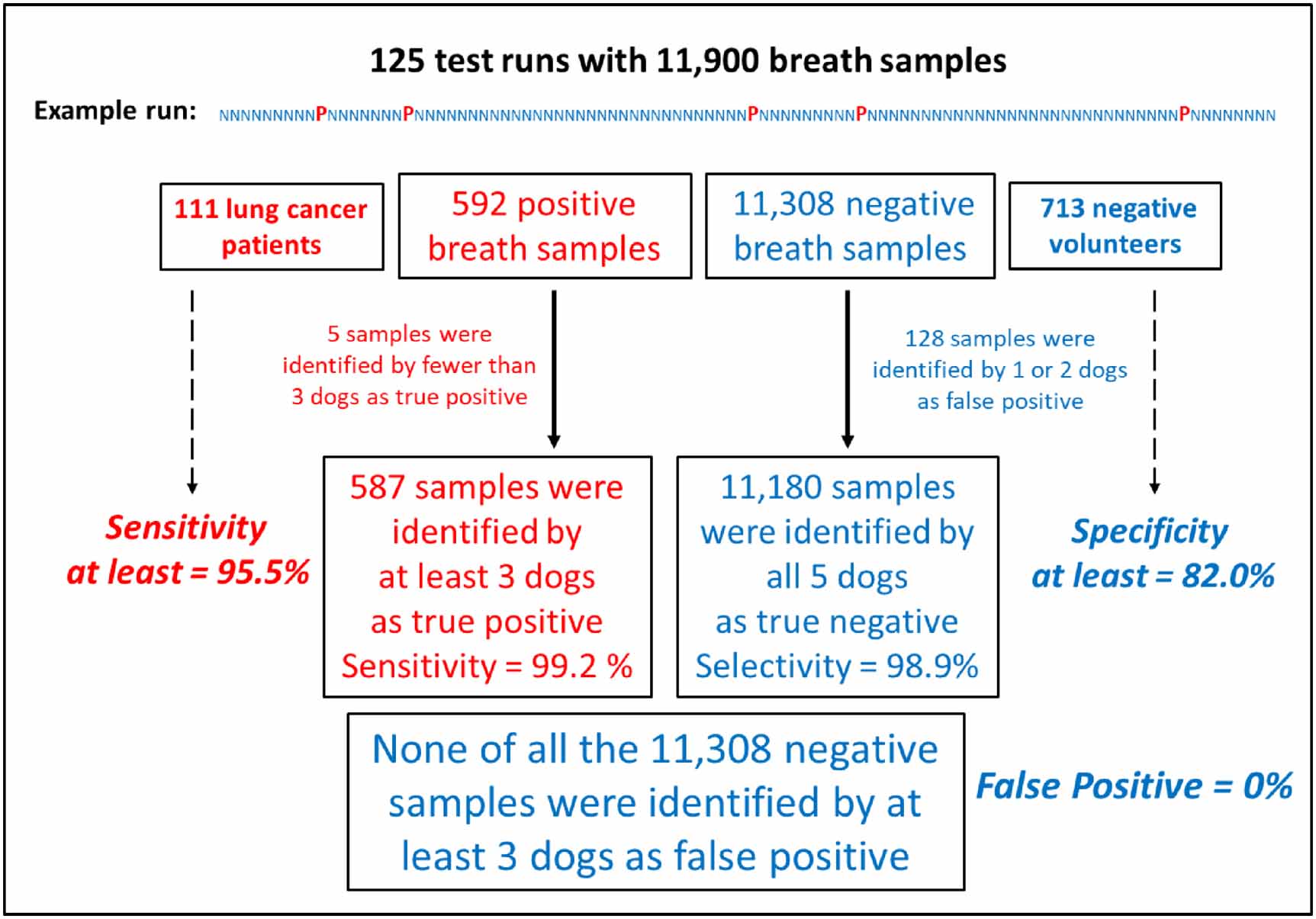
Between January and September 2024 breath samples from a total of 824 subjects, including 111 individuals with a histologically confirmed lung cancer and 713 volunteers with no prior lung cancer history were included in the evaluation. The characteristics of the donors of breath samples included in the study are presented in table 1.
Table 1. Characteristics of the patient collective.
Ten percent of the lung cancer patients recruited were classified as Union for International Cancer Control stage I, and 8% were classified as stage II. This indicates that 18% of the patients were in the early stages of lung cancer. Forty-six percent of the lung cancer patients had not undergone oncological treatment prior to donating positive breath samples (table 1). The majority of volunteers who provided negative breath samples were between 18 and 23 years old, in good health, and free of known diseases. The 713 control subjects can be grouped into two cohorts: The first is the ‘student cohort,’ which consists of 528 healthy control subjects who are mostly young. The second is the ‘chronic disease cohort’ (26%), which consists of 185 non-cancer patients with confirmed chronic diseases (See table 1). 59 patients of the chronic disease cohort suffered from chronic respiratory diseases and in further 126 cases from other chronic diseases but not from cancer (table 1).
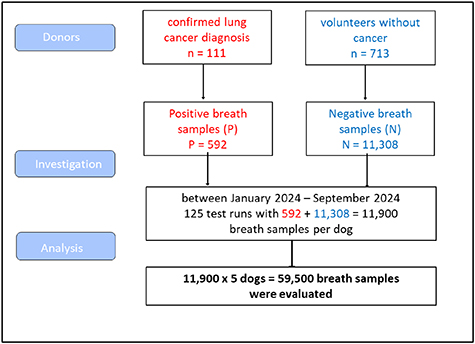
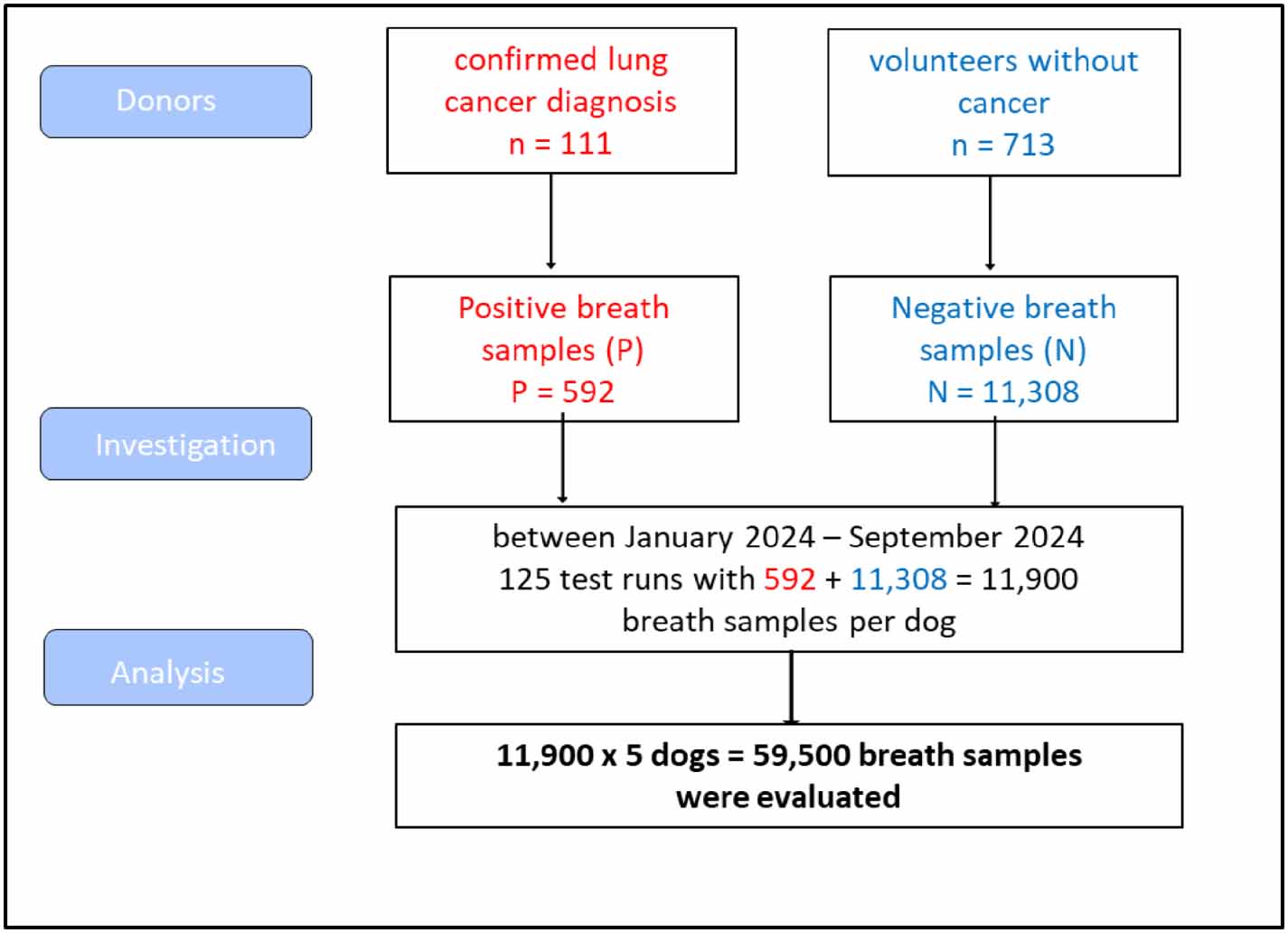
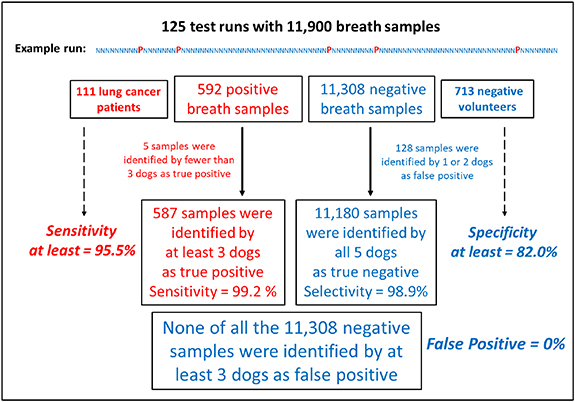
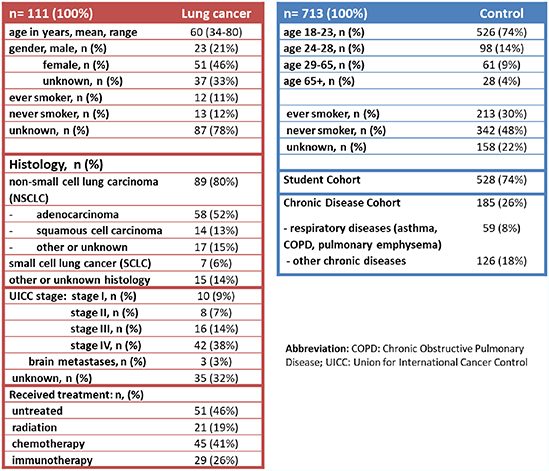
3.1. Dogs’ detection performanceEach dog conducted 125 search runs with in total 592 positive and 11 308 negative samples. Figure 2 shows an overview diagram of the number of included breath masks, test boards, and dog evaluations. A total of 592 positive (P) and 11 308 negative (N) masks were tested per dog in parallel. A total of 125 test runs per dog were carried out within nine months. The tests were carried out by five dogs (A)–(E) in figure 1, resulting in a total of 625 test runs and 59 500 mask evaluations as shown in figure 2.
Figure 2. Overview of included breath samples and dog evaluations.
Download figure:
Standard image High-resolution imageThe performance metrics were calculated separately for each dog based on standard diagnostic categories with 95% CI using the Wilson score method. A total of 625 independent test runs were performed and in summary the following results were obtained (table 2). All five dogs demonstrated comparable detection performance, sniffing out a total of 11 900 breath samples each, with a sensitivity of above 96% and a specificity of above 99%.
Table 2. Dogs’ individual detection performance.
Sensitivity (95%CIa) SensitivitySpecificity (95% CI) SpecificityDog(P = 592)FN(P = 111)(N = 11,308)FP(N = 713)A0.971 (0.954–0.982)1784.7%0.998 (0.997–0.998)2296.9%B0.975 (0.959–0.985)1586.5%0.997 (0.996–0.998)3495.2%C0.966 (0.948–0.978)2082.0%0.998 (0.997–0.999)2396.8%D0.980 (0.965–0.988)1289.2%0.997 (0.996–0.998)3495.2%E0.968 (0.950–0.979)1983.0%0.998 (0.997–0.998)2296.9%aCI, Confidence interval.
Since repeated breath samples were tested from the same subjects, the calculations were adjusted to individual measurements per subject. The recalculated performance metrics for the five dogs, based on the number of unique subjects (P = 111; N = 713), resulted in sensitivities ranging from 82% to 89%, specificities > 95% (table 2), accuracy > 94%, PPV> 80%, and NPV > 97%. The resulting FP rate was below 5% per dog.
3.2. Dogs’ detection performanceA bootstrap resampling analysis was performed with 10 000 iterations per configuration. For each iteration, subsets of two, three, or four dogs were randomly selected from the 625 test runs (see table 3). All simulated dog team sizes demonstrated robust sensitivities (table 3).
Table 3. Detection performance for different dog team sizes.
Dog teamSensitivity Sensitivitysetup(95% CIa) (P = 592)FN(P = 111)2 dogs (cutoff ⩾1)0.994 (0.990–0.997)496.4%3 dogs (cutoff ⩾2)0.990 (0.986–0.995)694.6%4 dogs (cutoff ⩾3)0.985 (0.981–0.990)991.9%5 dogs (cutoff ⩾3)0.992 (0.992–0.992)595.5%aCI, Confidence interval.
Figure 3 provides a summary of the combined results according to the CDDC® decision rules (see Materials and Methods 2.3). The evaluation of all 125 independent test runs was calculated using the number of unique breath sample donors, 111 positive (P) and 713 negatives (N). The results according to the CDDC® decision rules were zero FP, two FNs, and 131 inconclusive results (one or two dogs indicated the sample) from 11 900 breath samples. Based on unique subjects (N + P = 824), inconclusive results occurred for less than 16% of subjects. Five cancer breath samples were identified as TP by fewer than three dogs. Accordingly, the five dogs CDDC® test achieved at least a sensitivity of 95.5%. In accordance with the CDDC® decision rules, all five dogs must identify the negative mask as a TN. In 128 cases one or two of the five dogs indicated a control sample as FP, thus the specificity for that control samples were recognized as TNs by all five dogs was at least 82%. Following the CDDC® decision rules, none of the 11 308 negative samples were classified as FP by more than two dogs.
Figure 3. Summary of the five dogs’ evaluation according to the CDDC® decision rules.
Download figure:
Standard image High-resolution image 3.3. Model assumption for preexisting comorbidities (explorative sensitivity analysis)Twenty-six percent of the control subjects had pre-existing chronic comorbidities, while most of the negative donors in the student cohort were young and healthy (see table 1). The Chronic Disease Cohort (N = 185) represents a more suitable control group. Therefore, a subgroup analysis limited to this cohort was performed. For this purpose, all counted FPs were assigned to the subjects of the Chronic Disease Cohort (N = 185). Thus, the specificities for the dogs’ individual detection performance, as displayed in table 2, were calculated as (185—FP)/185. This would result in individual specificities ranging from 81.6% to 88% for the five dogs, and accuracy > 84%, PPV> 80%, and NPV > 91%. Regarding the CDDC® decision rules (see figure 3), it remains the case that no breath sample worn by a chronically ill person was classified as a FP by more than two dogs.
3.4. Analysis for potential confounders on dogs’ detection performanceTo evaluate potential predictors and confounding influences on detection performance, we fitted GEEs models (table 4). The model incorporated dog mood, weather conditions, ambient temperature, and the identity of the supervising person as independent variables. The analysis was based on each dog’s detection performance per trial day, yielding a total of 625 dog-day observations across 125 trial days.
Table 4. Association factors for detection performance.
125 search runs × 5 dogs- n = 625 (100%)PredictorCoefficient (β)95% CIap-valueDog moodReference: balanced mood, n = 538 (86%)Motivated, n = 52 (8%)0.776(−0.169, 1.722)0.108Overly motivated, n = 35 (6%)−0.203(−0.897, 0.491)0.566WeatherReference: sunny, n = 185 (30%)Cloudy, n = 100 (16%)−0.947(−1.490, −0.403)0.001bRainy, n = 340 (54%)−0.008(−0.595, 0.578)0.978Temperature range 4 °C–32 °C; mean 15.4 °C0.0004(−0.031, 0.031)0.981SupervisorReference: Person 1; n = 275 (44%)Person 2, n = 45 (7%)−0.324(−0.597, −0.052)0.020bPerson 3, n = 85 (14%)−0.071(−0.582, 0.439)0.439Person 4, n = 100 (16%)−0.223(−0.599, 0.153)0.245Person 5, n = 10 (2%)−1.345(−2.409, −0.282)0.013bPerson 6, n = 35 (6%)0.966(0.088, 1.843)0.031bPerson 7, n = 20 (3%)0.425(−0.967, 1.816)0.550Person 8, n = 15 (2%)−0.596(−0.951, −0.240)0.001bPerson 9, n = 20 (3%)0.025(−1.02, 1.07)0.962Person 10, n = 20 (3%)1.570(−0.529, 3.669)0.143aCI, Confidence interval; n, number of search runs. Negative coefficient β indicate an association with lower detection performance, while positive coefficient β indicate an association with better performance.bSignificant p-values p < 0.05 are indicated.
Under reference conditions, balanced dog mood, sunny weather, and average ambient temperature of 15.35 °C, and supervisor person 1, the model intercept was significantly positive (β = 1.291, p < .001), reflecting high baseline detection accuracy. The dog’s mood, as reported by the handler, and the ambient temperature do not appear to have a significant impact on the dogs’ detection performance, while cloudy in relation to sunny weather appears to significantly reduce detection performance (β = − 0.95, p = .001). A discernible variation in the dogs’ detection performance was observed with regard to the different supervisors of the search runs. Person 2 who supervised 7% of the search runs, was associated with reduced detection performance (β = − 0.324, p = .020). Similarly, persons 5 and 8, who each supervised only 2% of the trials, were significantly negatively associated with detection performance (β = − 1.345, p = .013 and β = − 0.596, p = .001, respectively). In contrary, person 6 was associated with improved performance (β = 0.966, p = .031). No statistically significant differences in detection performance were found among the other supervisors.
Under training conditions, detecting lung cancer from breath samples using the CDDC® method with five dogs appears feasible, with at least 95.5% sensitivity. The minimum requirement for trained sniffer dogs is a sensitivity of at least 90%. Previous and more recent studies involving sniffer dogs have shown that dogs are generally capable of detecting lung cancer breath samples with high sensitivity and specificity [10, 12, 15–17, 19]. Ehmann et al proposed using a ‘corporate decision’ strategy with multiple dogs to improve sensitivity since hit rates vary among individual dogs. We were indeed able to demonstrate that the CDDC® decision rule that at least three out of five dogs must identify the mask as TP increases sensitivity. Furthermore, the second CDDC® decision rule—which stipulates that a sample is considered a TN only if all five dogs reach this conclusion unanimously—ensures that suspicious positive or FP results can be clarified through repeat testing, if necessary. In a few cases (less than 2%), the breath samples were indicated as positive by only one or two dogs, resulting in inconclusive results. If an inconclusive result is obtained during a clinical examination, the donor of the respective sample must provide a repeated breath sample, and a new test must be performed. Given the repetitive testing of volunteers during these training runs, based on unique subjects, the inconclusive rate was maximal 16%. Since TNs are defined by agreement among all five dogs, the resulting CDDC® specificity, based on unique control subjects, was at least 82%.
Nonetheless, maintaining this level of accuracy over long periods of time is difficult since dogs are living beings, not machines. This requires thoroughly thought-out and carefully structured training of the dogs. Notably, in present evaluation, the analysis of potential confounding factors revealed that neither the dogs’ mood nor temperature had a significant influence on the dogs’ detection performance. Despite belonging to different breeds (see figure 1), the dogs showed no significant differences in terms of their accuracy in their detection performance (table 2). However, a significant association between cloudy weather and reduced performance was identified (table 4). Additionally, significant associations were identified between the dogs’ detection performance and the individual supervisors responsible for coordinating the search runs (see table 4). The supervisor’s tasks are complex and require experience and routine to achieve a reliably high sensitivity value. For instance, Persons 2, 5, and 8, which coordinated only 2%–7% of the search runs, were associated with significantly lower detection performance. On the other hand, with Person 6 in charge of supervision, seemed to be associated with the most accurate detection performance (see table 4). The dogs’ detection performance partly depends on the supervisors’ communication skills, so the search runs’ optimization is possible. Interestingly, another study [19] recently demonstrated the high-performance skills of sniffer dogs in detecting cancer samples. Unlike in our study, they used samples of different types of cancer and analyzed the probes by combining trained detection canines with artificial intelligence (AI) tools. In a special detection room, the dogs were allowed to identify six samples one by one. The dogs’ reactions were monitored and analyzed with the help of AI. Notably, the results showed that incorporating AI increased sensitivity from 64.4% to 94.8%. The analyses of potential confounders performed here suggest that dog searches should be directed by an experienced supervisor and avoided in cloudy weather.
In another approach, Vadala et al [20] reviewed electronic nose (eNose) devices, which are emerging as promising tools for noninvasive lung cancer detection. By analyzing exhaled breath for volatile organic compounds, eNoses can discriminate lung cancer from non-lung cancer and other respiratory diseases with over 80% accuracy [20].
The CDDC® method demonstrated high consistency in the training scenarios evaluated here and enables the simultaneous analysis of numerous samples. It is not yet possible to generalize the performance of the CDDC® method for lung cancer screening because the current training cohort consisted mainly of young, healthy individuals and lacked individuals with high-risk or suspected lung cancer. In the context of planned future screenings using authentic samples of suspected cancer, further improvements and quality control are required. When training sniffer dogs, it is important to avoid establishing recognizable patterns. The dogs should not be conditioned to recognize typical hospital odors. Therefore, all breath samples, including those from lung cancer patients, must be collected in a neutral environment, such as outdoors. Training and education of the dogs will also be further improved. The dogs’ well-being will be prioritized in the future development of this method, ensuring detection in natural, stress-free conditions. To ensure quality control, process optimization with regular monitoring is planned. Temperature, humidity, and air pressure affect the volatility, release, and dispersion of odors. Approaching rain can also activate the release of aromas from the environment, which can interfere with accurate detection. In order to limit the dependence of the accuracy of search runs on weather conditions, constructive measures should be taken at the facility. In addition to early detection, smoking cessation is an important way to reduce the risk of cancer, and is a mandatory component of lung cancer screening programs [21], and should not be overlooked in the future.
This study has numerous limitations. A major limitation of this study is its retrospective study design and the fact that the control group consisted largely of healthy individuals and was not age-matched. Additionally, complete demographic data and information on smoking status was unavailable for all subjects. Only breath samples from patients with confirmed lung cancer diagnoses were used for training and cases of suspicious lung cancer were not tested. Until we have samples from patients with suspected lung cancer, we cannot determine the sensitivity and specificity with which this sniffer dog method will likely work in a real-world lung cancer screening setting and clinical applicability remains limited. Furthermore, there are potential sources of variation in the data, including pseudoreplication, which can arise from multiple sample donations or repeated testing of the same sample. However, we recalculated all performance metrics based on the number of unique subjects. Additionally, an exploratory sensitivity analysis, demonstrated reasonable detection accuracy, even when considering solely subjects afflicted with chronic respiratory diseases, such as asthma or COPD, but not cancer.
Although sniffer dogs have superior olfactory organs, direct comparative studies have shown that the eNose has a better detection performance than dog teams because eNoses are less susceptible to interference and better reproducible [18]. It is still unclear whether the dogs can detect suspected cases or early-stage lung cancer within a lung cancer screening program when positive samples are provided only occasionally and irregularly [22]. Sniffer dogs are limited in their use due to their inherent nature and the many factors that can influence their performance. Therefore, doubts have been raised about their suitability for reliable use in clinical practice [14]. Many of these uncertainties were here identified, managed, and had been optimized during the rigorous development of the CDDC® method’s training and implementation protocol. At present, both the use of detection dogs and eNose analysis technologies show great promise. However, more controlled clinical trials with larger sample sizes are needed to justify using them as diagnostic tests in routine clinical practice. Even if this dog scent method for the direct early detection of lung cancer as part of a screening program, is not yet fully established, it holds potential in the confirmation of suspected cases of lung cancer. Further possible applications, such as monitoring during the course of anticancer treatment or monitoring for recurrences, also appear conceivable.
The reduction in lung cancer mortality may be achieved through screening of high-risk individuals, and accordingly, national screening programs with LDCT are in progress in many countries [4]. As a possible additional lung cancer screening method, this sniffer dog method described here could offer several merits. It is non-invasive and has no adverse effects. Breath sampling, storage, and testing are relatively simple, as is evaluating the results. Labradors, Retrievers, and German Shepherds seem to be particularly good at scent detection [8], so these dogs have been trained here. This method differs considerably from other canine detection methods. First, living with dogs as family members means that dog and dog owner always work together as a unit. Second, they work in a ‘naturally contaminated’ environment filled with foreign odors, rather than in clean, sterile rooms. Third, they examine 100 samples in a single scan instead of just few samples in sterile boxes. Fourth, each search run is guaranteed to have quality assurance with accompanying positive and negative control masks. Fifth, in the event of inconclusive test results, a decision may be reached by repeating the breath sampling and testing again. However, in the present retrospective evaluation, only breath samples were included that were clearly positive or negative, and only a small number of suitable control subjects without lung cancer were examined. Consequently, it remains entirely unclear whether dogs can detect suspected lung cancer cases. In order to validate this sniffer dog method, it is therefore essential to prospectively evaluate a real lung cancer screening population in a controlled clinical study that allows for a direct comparison with parallel LDCT examinations. In consideration of the established guidelines for the detection of lung cancer [23] and the recently published White Paper on Assessment of Potential Participants in Lung Cancer Screening in Germany [24], this sniffer dog method will now be evaluated prospectively in a planned proof-of-principle study.
We would like to thank the whole team at Docscan GmbH in Erkelenz Germany, the dog trainers, and the dog owners for their excellent support in providing data. Special thanks go to the scent dogs, Aaron, Aki, Biest, Loki, and Lu. We would also like to thank all the volunteers who supported this study by donating their breath samples. The authors have confirmed that any identifiable participants in this study have given their consent for publication.
All data that support the findings of this study are included within the article (and any supplementary files).
This study was supported via the institutional budget of the Research Institute Havelhöhe and partially funded by unrestricted research grants from Dogscan GmbH in Erkelenz, Germany. The investigators were contractually independent of the funders. The funders had no role in study design, data analysis, preparation of the manuscript and the decision to publish this study.
The study was conducted in accordance with the Declaration of Helsinki, and the retrospective evaluation of this analysis was approved by the ethics committee of Charité—Universitätsmedizin Berlin (EA1/111/25) on 22.05.2025.
C. Grah reports grant support from AstraZeneca, Takeda, Novartis, Chiesi, Iscador, outside the submitted work. H. Wüstefeld reports grant support from AstraZeneca and Berlin-Chemie outside the submitted work. J. Kalinka-Grafe reports grant support from AstraZeneca outside the submitted work. The other authors have no conflicts of interest to declare.
Comments (0)