
Remember me
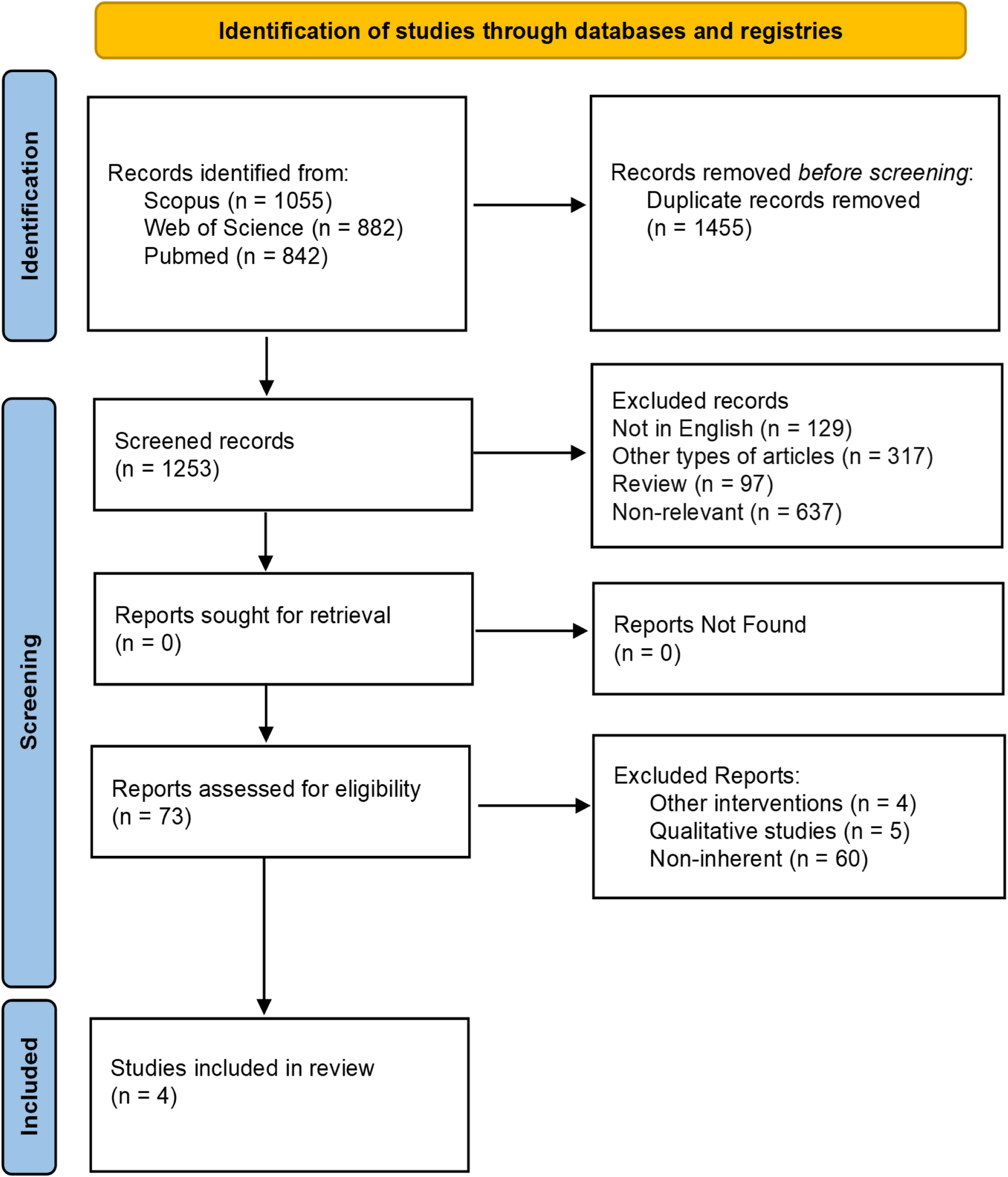
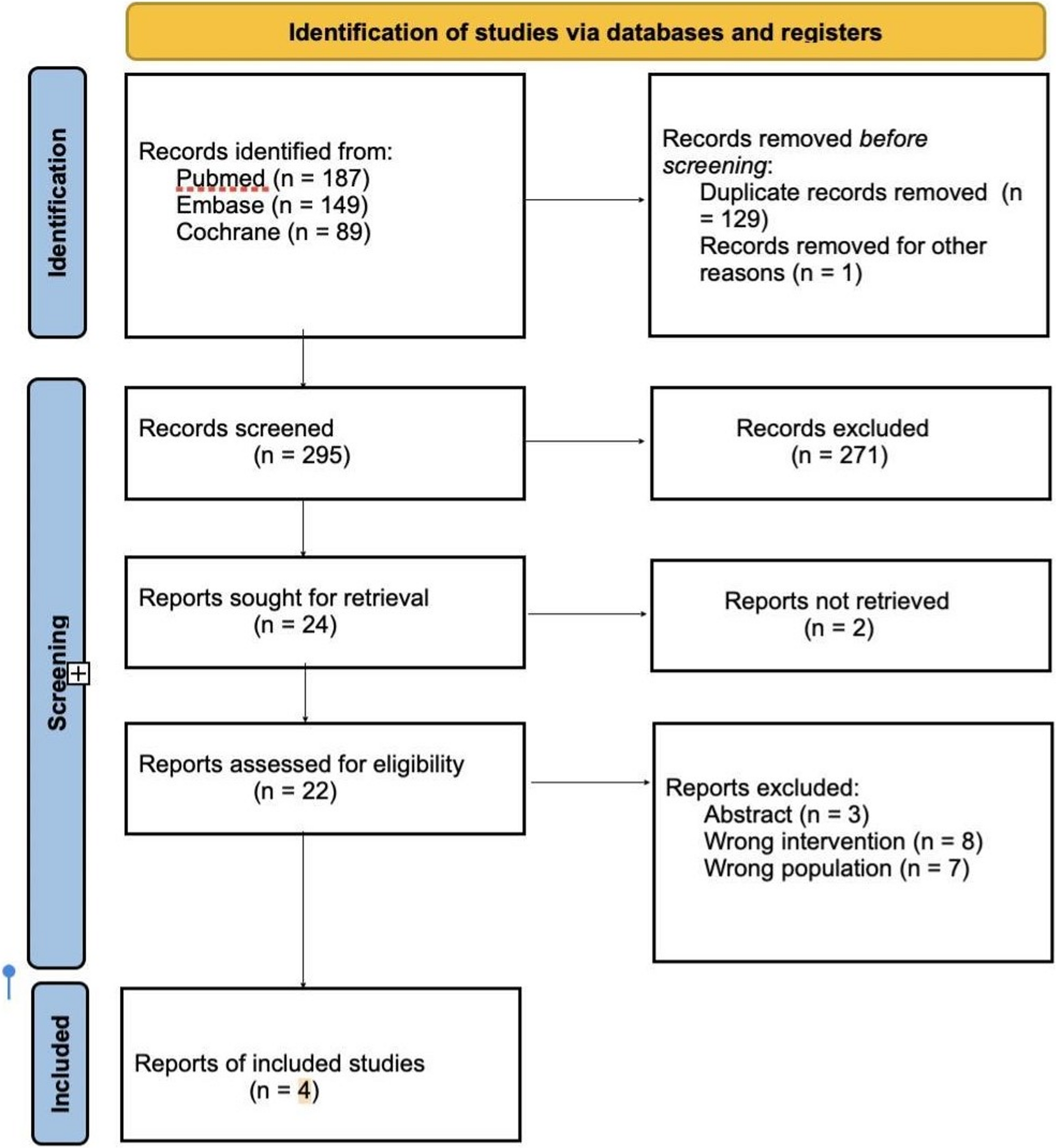
The search identified 5510 records, of which 1047 were duplicates. A total of 4463 titles were screened and 404 abstracts. The percentage agreement was 97% for title screening and 98% for abstract screening. Full texts of 72 papers were assessed and thirteen papers met the inclusion criteria (Fig. 1). Agreement was 100% for full-text screening between both reviewers. Following the completion of quality assessment, a decision was made to undertake a narrative synthesis rather than a meta-analysis due to the heterogeneity of the included papers. Specifically, the papers varied significantly in terms of their sample size and the timing of when paternal exposures were recorded. Additionally, the studies examined outcome at different time points.
Fig. 1
Study characteristics of the included studies, including exposure and outcome measurement are presented in Table 1. Of the thirteen studies included in this systematic review, 12 were prospective cohort studies [16,17,18,19, 21,22,23,24,25,26,27,28] and one was a case-control study [20]. The sample size ranged from 509 participants [20] to 29,216 participants [22]. Six studies assessed paternal smoking [16,17,18,19,20,21], seven assessed paternal overweight/obesity [22,23,24,25,26,27,28], and two considered both exposures [20, 27]. The outcome of childhood overweight/obesity was assessed at different ages, from birth to 11 years. Three papers were based on the same population [16, 17, 21], the Generation R study in the Netherlands. Eight of the papers recorded the paternal exposures antenatally [16,17,18,19,20,21,22, 25], whilst five recorded postnatally [23, 24, 26,27,28]. The timing of participant recruitment in relation to birth of the child varied amongst the studies. Six papers included cohorts which recruited antenatally [16, 17, 21,22,23, 25] whilst the other seven recruited postnatally [18,19,20, 24, 26,27,28]. Three papers used a population from the Netherlands [16, 17, 21], two in the UK [26, 28] and one each was in Germany [18], Hong Kong [19], Iran [20], Norway [22], USA [23], China [24], Australia [25] and Sweden [27].
Table 1 Characteristics of included studiesTable 2 Study findings and quality assessmentTable 3 Summary of findings ( + = positive association) and confounders adjusted for in the included studiesPaternal Overweight/Obesity and Childhood Overweight/ObesityAll studies [20, 22,23,24,25,26,27,28] found a positive association between paternal overweight/obesity and childhood overweight/obesity, with paternal BMI used as the measure. Two studies [22, 23] adjusted for paternal smoking, while five did not [24,25,26,27,28]. Seven studies adjusted for maternal BMI [22,23,24,25,26,27,28]. One study, where the main exposure was paternal smoking, did not consider paternal BMI in multivariate analysis due to multiple linear correlations with high weight at birth and its prominent impact [20]. Two studies recorded fathers with overweight/obesity antenatally [22, 25] whilst five recorded postnatally [23, 24, 26,27,28], all within the 1-year inclusion period. Three studies measured overweight/obesity in children at multiple time points but found no significant association beyond early childhood [23, 24, 27]. None examined gender-based subgroup analysis.
Quality assessments of each paper can be found in Table 2. Six studies were rated as fair and one as poor. The study that was assessed as poor relied on maternal self-report of child BMI which could cause non-differential information bias in outcome measurement [22]. One study measured paternal exposure using weight and height values recorded at different times, height at the first month home visit post-birth and weight during pregnancy. This discrepancy in measurement times means that any changes in weight during this period was not captured [24]. The risk of selection bias was increased in one study due to not all children being clinically assessed due to funding issues towards the latter part of the study follow-up and thus being excluded from the analysis [25].
Additionally, one study excluded participants with missing data, measurements outside the specified age ranges, and preterm births; excluded children had lower birth weights than those included (3495 g versus 3580 g), introducing possible bias [27]. This study only included factors with significant associations (p < 0.05) in the initial univariable analysis in the subsequent multivariable models [27]. One study employed a stratified sampling design to over-represent children living in disadvantaged areas and from ethnic minority groups improving generalizability of the study [28].
Paternal Smoking and Childhood Overweight and ObesityFive out of six papers found an association between paternal smoking during pregnancy and the first year of life with childhood overweight/obesity [17,18,19,20,21]. However, the findings from two papers may be biased due to lack of adjustment for relevant confounding factors [19,
Comments (0)