In this nationally representative sample of U.S. adults, we found a significant positive association between Overactive Bladder (OAB) and the Magnesium Deficiency Score (MDS). This association remained significant in models adjusted for multiple covariates, regardless of baseline characteristics, and was particularly pronounced in individuals with MDS scores greater than 3.
In a urodynamic evaluation, urinary pH was found to be significantly negatively correlated with detrusor pressure [27]. This implies a significant association between acidic urine and OAB, potentially due to acidic urine stimulating the nerve fibers in the bladder epithelium, leading to overactivity. Intake of magnesium salts can enhance citrate excretion and increase urinary pH, thereby alkalinizing the urine. This not only improves lower urinary tract symptoms [28] but also prevents the formation of crystals in the urinary system, reducing the risk of urolithiasis [29].
Magnesium possesses unique antioxidant and anti-inflammatory properties. It has been found to inhibit the activation of NF-kB, potentially reducing inflammation. Oral magnesium supplementation can effectively lower serum CRP (a marker of inflammation), suggesting its significant role in alleviating chronic systemic inflammation [30]. Chronic inflammation can lead to functional changes and increased sensitivity of the bladder, resulting in OAB symptoms. A prospective study indicated that chronic inflammation is associated with Overactive Bladder (OAB) syndrome [31]. Additionally, research has shown elevated cytokine levels in the urine of OAB patients [32]. These findings suggest that the release of inflammatory cells and mediators leads to poor bladder perfusion and an inflammatory response in bladder tissue, triggering OAB symptoms. Therefore, oral magnesium supplementation may reduce inflammatory responses and effectively alleviate symptoms in OAB patients.
As age increases, changes in magnesium metabolism occur in the body, including reduced intake and increased excretion, ultimately leading to magnesium deficiency. Mild magnesium deficiency is common in older adults and is associated with sleep disorders, mood disorders such as depression and anxiety, and cognitive impairment. Research indicates that many human diseases are related to magnesium deficiency, including cardiovascular diseases, hypertension, osteoporosis, metabolic syndrome (MetS), type 2 diabetes, and mental disorders. Additionally, magnesium deficiency is linked to mitochondrial dysfunction and oxidative stress markers [33]. It is well known that aging is accompanied by an increase in urinary disorders, which also contribute to the fibrosis of the bladder detrusor muscle, and exacerbates bladder ischemia and hypoxia. This can increase the production of free radicals, leading to oxidative stress and the activation of inflammatory responses, ultimately resulting in reduced bladder compliance and overactivity [34]. All these factors are risk factors for the symptoms experienced by OAB patients.
Studies have found that magnesium supplementation at certain doses can help improve these chronic conditions. Magnesium can enhance sleep by regulating a brain chemical called GABA, which is crucial for sleep. It is also suggested as an adjunct treatment for insomnia, as it helps relax muscles and regulate the nervous system. Good sleep can alleviate OAB symptoms. Magnesium plays a significant role in the occurrence and development of Metabolic Syndrome (MetS). Oral magnesium supplements can improve MetS events, significantly reducing hypertension, hyperglycemia, and hypertriglyceridemia. Lowering the incidence of MetS events can help reduce the prevalence of OAB [35]. In a prospective, randomized, double-blind, placebo-controlled study, women who took magnesium supplements experienced a reduction in nighttime awakenings to urinate and improved bladder control during the day [36]. The exact etiology of OAB remains unclear, and current pharmacological treatments mainly involve anticholinergic drugs, which have side effects such as dry mouth and constipation. However, magnesium supplementation can potentially prevent and treat OAB, avoiding these adverse drug reactions.
This study reveals a significant positive correlation between MDS and the prevalence of OAB, suggesting that magnesium deficiency may play an important role in the onset and progression of OAB. Magnesium, as a key physiological regulator, is involved in nerve conduction, muscle contraction, and smooth muscle function regulation [37]. In the nervous system, magnesium stabilizes neurotransmitter release and modulates neuronal excitability [38]. Magnesium deficiency may enhance neuronal excitability, leading to bladder overactivity. Additionally, the impact of magnesium on bladder smooth muscle cannot be ignored. Research indicates that magnesium deficiency can promote excessive smooth muscle contraction by altering intracellular calcium ion concentrations [39], which exacerbates OAB symptoms. On the other hand, magnesium has significant anti-inflammatory effects [40]. Magnesium deficiency may lead to an increase in chronic low-grade inflammation, further activating inflammatory factors such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), which play crucial roles in bladder tissue damage and dysfunction. Therefore, magnesium affects bladder function through multiple pathways, and maintaining appropriate magnesium levels may offer new approaches for the prevention and treatment of OAB.
Insufficient magnesium intake is the primary cause of magnesium deficiency, influenced by various factors such as unbalanced dietary patterns and excessive softening or purification of drinking water or seawater. Additionally, gastrointestinal malabsorption, alcohol consumption, the use of diuretics, PPIs, and other causes of excessive urinary magnesium excretion can also contribute to magnesium deficiency. Surveys indicate that a significant portion of the U.S. population has inadequate dietary magnesium intake, well below the recommended daily allowance [41]. This is attributed to the unbalanced food intake typical of Western diets, characterized by excessive consumption of high-fat meats and processed foods, and insufficient intake of whole grains and green vegetables. The 2020–2025 Dietary Guidelines for Americans have refined recommendations for a healthy eating pattern, suggesting a daily intake of approximately 170 g of grains, with at least half being whole grains [42]. This highlights the nutritional community’s emphasis on whole grain consumption. Additionally, cooking and refining processes can significantly reduce the magnesium content in foods, as a substantial amount of magnesium is lost during these processes. Over-softening or purification of drinking water or seawater also contributes to insufficient magnesium intake. The World Health Organization (WHO) has not specified a recommended magnesium content for drinking water in its guidelines [43]. Excessive urinary magnesium excretion often results from alcohol consumption and the use of loop diuretics, leading to a negative magnesium balance. Inhibition of gastric acid secretion has been shown to increase the pH levels of the small intestine and colon. This increase in pH reduces the solubility of Mg2+, leading to decreased paracellular absorption of Mg2+ in the small intestine [44].
Given the numerous potential benefits of magnesium and its association with many chronic diseases, maintaining adequate magnesium levels in the body should be an important public health goal. There is a need to address insufficient magnesium intake, accurately evaluate recommended magnesium intake levels for the population, and promote magnesium supplementation through food. This includes reducing the refinement of grains, advocating for the consumption of whole grains and dark green vegetables rich in magnesium, and minimizing the over-purification or softening of drinking water. In the context of an aging population, maintaining optimal magnesium balance throughout life could help prevent related chronic diseases and may become a cost-effective and safe health strategy. This requires significant attention from the medical, nutritional, and social sectors.
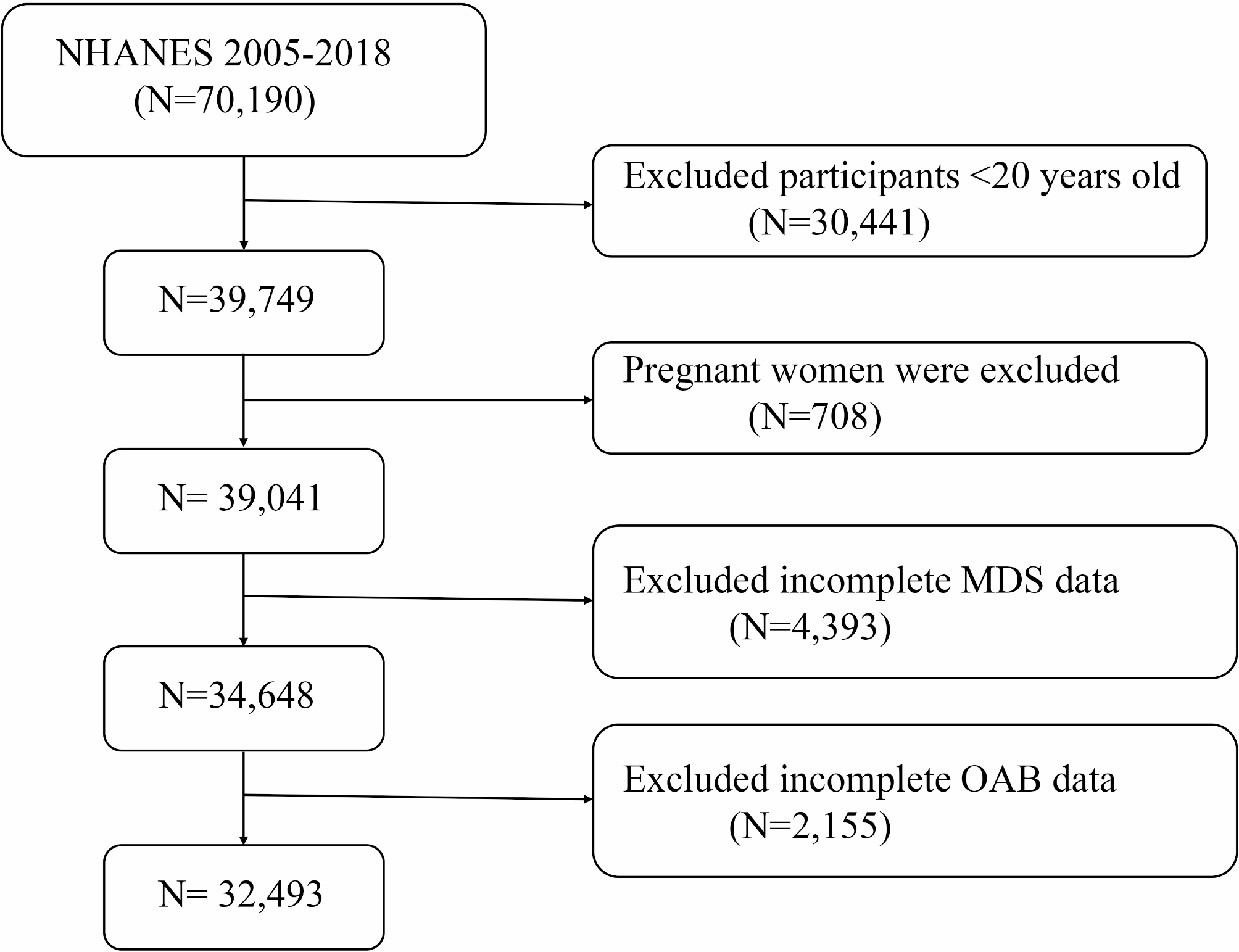
Our study has several strengths. First, we utilized the NHANES database, which provides a large, multiethnic sample, ensuring the representativeness of our sample size. We carefully adjusted for covariates such as age, gender, race, and comorbidities, and assessed their stability across various statistical models. Second, the diagnosis of OAB was based on a scoring system rather than self-report, which helps reduce recall and subjective biases. We also performed sensitivity analyses, including subgroup analysis, to validate the robustness of our findings.
However, certain limitations must be acknowledged. As a cross-sectional study, despite adjustments for numerous confounding factors, we cannot entirely rule out the presence of unmeasured confounders and cannot establish causal relationships between variables. Although our study identifies a significant association between a higher MDS and increased OAB prevalence, the cross-sectional design precludes causal inferences. Future longitudinal or interventional studies are needed to determine whether improving magnesium levels can effectively alleviate OAB symptoms. Additionally, Future studies could consider clinical intervention trials, bladder histological assessments, and the detection of relevant molecular biomarkers to provide stronger evidence for the potential role of magnesium in OAB treatment.





Comments (0)