
Remember me






A randomized crossover design with counterbalanced treatment conditions was used. One condition provided the participant with a commercially available low-carbohydrate shake to initiate the fast. The other intervention provided the participant with a commercially available high-carbohydrate, yet isocaloric, shake to initiate the fast. The effects of these conditions on markers of glycemic control were assessed. These two conditions involved a 24-hour water-only fast beginning at 8:00 am and ending at 8:00 am the following day. A final assessment 24 h after participants broke their fast took place the next day. Approval from the University’s Institutional Review Board was obtained prior to initiating any aspect of this study and can be found in OpenScience Framework https://doi.org/10.17605/OSF.IO/9N7BU.
Participants completed both fasting conditions outside of the lab with a 7-day washout between each session. Using randomizer.org, condition order was randomly assigned to participant numbers prior to the study. Participants were assigned numbers chronologically based on when they joined the study.
Prior to each laboratory session, participants were screened for contraindications to participation as outlined in the section below. The following outcome variables were measured: Body Mass Index (BMI), fat mass, percent body fat, visceral adipose tissue, capillary BHB, continuous subcutaneous glucose monitoring, and plasma concentrations of insulin, glucagon, GLP-1, and GIP.
ParticipantsTwenty-four adults (11 female and 13 male) were recruited by word of mouth, advertisements, and fliers in the local community. Participants were 50 years of age or older with a BMI > 27, who did not participate in more than 150 min of physical activity per week [26]. This population was selected because older adults with obesity are at the highest risk of metabolic complications and may benefit from periodic fasting [27]. Participants diagnosed with chronic or metabolic diseases, eating disorders, or food allergies were excluded from the study. Additionally, participants were excluded who were taking medications that alter metabolism, appetite, or neurological function [28]; habitually consuming 60 mg or more of caffeine daily [29]; participating in calorie or carbohydrate-restricted diets; fasting more than once per week; or having irregular sleep patterns. Women were also excluded if they were pregnant or lactating [30].
Potential participants for the study completed an online qualification survey. As part of the online survey, participants were asked to report any food allergies. Qualifying candidates were invited to participate in the study and all interested participants gave written informed consent prior to participation in any aspect of the study. Participants were also instructed to avoid caffeine consumption and other stimulants on testing days as well as to refrain from vigorous physical activity for the 24-hour period prior to testing. Adherence to pre-test day protocols was assessed at the beginning of each session. If pre-test protocols were not followed, the participant was rescheduled.
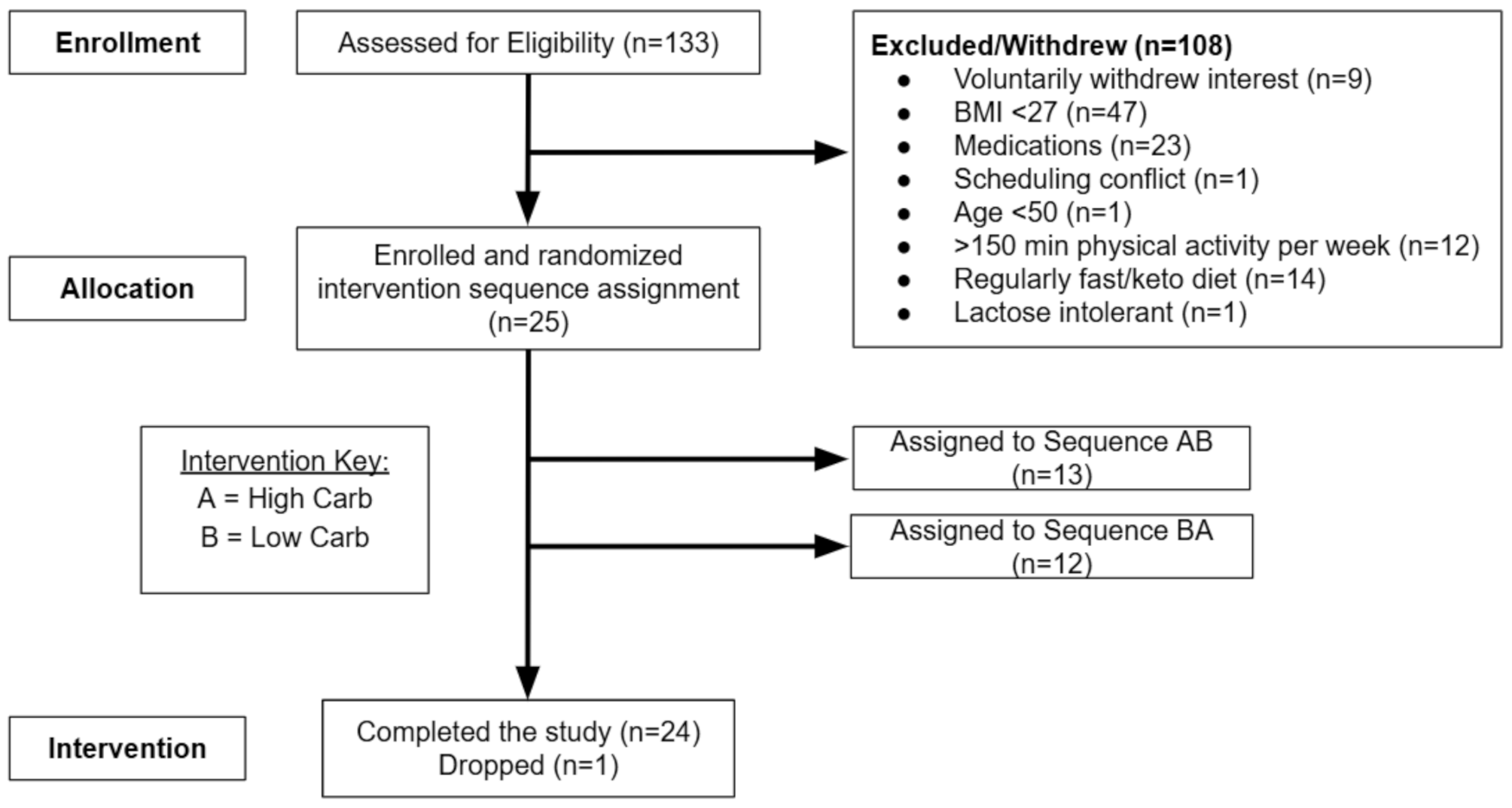
One hundred and thirty-three individuals were assessed for eligibility for the study as outlined in Fig. 1. Most were excluded due to low BMI, medications, or high amounts of physical activity. Of these individuals, twenty-five qualified and subsequently enrolled in the study. Twenty-four individuals completed all aspects of the study, and one participant chose to no longer participate due to an inability to tolerate the blood draws.
Fig. 1 Treatment sessions
Treatment sessionsParticipants reported to the Research Lab at the University for each assessment. Each participant was informed of the main purpose of the study and familiarized with the testing procedures. Training for proper portable ketone meter use took place in accordance with manufacturer guidelines (Abbott Laboratories, Abington, UK), and participants were given a copy of these testing instructions.
Before the first treatment condition, weight was measured using a digital scale (Seca, Hamburg, Germany) accurate to ± 0.1 kg, and height was measured by a stadiometer accurate to ± 0.1 cm (Seca, Hamburg, Germany). Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m2). Participants then received a whole-body dual-energy X-ray absorptiometry (DXA) scan to assess body composition, including fat mass, percent body fat, and visceral adipose tissue [31,32,33]. The scan was performed using a GE iDXA (GE, Fairfield, CT) which was calibrated at the beginning of each day of use using a manufacturer-provided calibration block. Encore software version 17 was used to analyze each scan, and visceral adipose tissue was calculated using the Core Scan application of the machine [34, 35].
Subjects were then provided with a continuous glucose monitor (CGM) (“Freestyle Libre” by Abbott) which was attached to the back of the non-dominant arm by the research team in accordance with manufacturer’s guidelines. Participants were asked to eat normally leading up to the fast but to abstain from food after 8:00 pm the night before the fast to normalize measured blood markers.
Shortly before 8:00 am the next day, participants reported to the lab for a baseline blood draw and finger prick. They also completed a survey on Qualtrics’s online survey software (Qualtrics.com), where they logged their own capillary BHB levels. Based on random assignment, participants then consumed either the HC/LF or LC/HF shake within a 5-minute window. The standardized shake was consumed by 8:00 am, initiating the 24-hour fast. Another blood draw, finger prick, and survey were taken an hour after shake consumption. Participants then proceeded with their normal daily routine with the exception of pricking their finger and logging their own capillary BHB levels at 12:00 pm, 4:00 pm, and 8:00 pm. Participants were reminded via automated text message to take and record these measurements both two hours prior to each appointment and immediately before they needed to take a capillary ketone reading.
Participants were asked to go about their normal activities of daily living during the testing period, though they were asked to avoid strenuous activity including strength or cardiovascular training, yard work, hiking, or other moderate activity during the fasting period and the 24-hours prior. Participants were asked to maintain their normal sleeping patterns. Each fast was a water-only fast, meaning no other food or beverages were consumed during the fasting period besides water. Participants were instructed to stay hydrated throughout the fast. Non-caloric, electrolyte, and caffeinated beverages/additives were not allowed. Gum chewing was also prohibited.
Participants returned to the lab at 8:00 am the next day (24 h) for a blood draw, finger prick, and survey. Following this visit, participants were permitted to break their fast with their own meal and resume their regular activity and diet. Participants reported to the lab the following day at 8:00 am (48 h) for a final blood draw in an overnight fasted state (12 h) before eating their first meal of the day. Between the 24-hr visit and 48-hr visit normal unsupervised eating and activity patterns were practiced. See Fig. 2 for a complete visual of protocols.
Fig. 2
Protocol timeline of all measurements taken
DXA = dual-energy X-ray absorptiometry. CGM = continuous glucose monitor. LC/HF = low carbohydrate/high fat/moderate protein. HC/LF = high carbohydrate/low fat/moderate protein
Standardized shakeParticipants were given a standardized shake to initiate each fast. The energy needs for each participant were estimated using equations validated by Hall et al. used by the National Institutes of Health [36]. This equation uses height (cm), weight (kg), age (years), and sex to predict basal metabolic rates (BMR) and has been validated for accuracy and reliability. An activity factor of 1.4 was used to estimate total daily energy requirements. Participants were given 25% (BMR x 1.40 × 0.25) of their daily caloric requirements in the standardized shake in each fast, though the macronutrient composition differed between shake conditions. The commercially available LC/HF shake– HlthCode® Chocolate Macadamia flavor– was consisted of the following macronutrient calorie breakdown: carbohydrates = 4.36% (nutrose), Fat = 66.21% (blend of saturated, monounsaturated, and polyunsaturated fats from coconut oil, olive oil, medium chain triglycerides, flaxseed, cocoa butter fat, and ghee), and Protein = 29.43% (whey protein concentrate, collagen, egg whites). The commercially available HC/LF shake– Carnation Breakfast Essentials® High protein– consisted of the following macronutrient calorie breakdown: carbohydrates = 56.78% (sucrose, maltodextrin, and lactose), Fat = 13.15% (blend of saturated, monounsaturated, and polyunsaturated fats from milk), and Protein = 30.06% (whey protein isolate and whey and casein from milk). Shake volume in each condition was matched within subjects and was computed using a protected spreadsheet calculator that mixed the shakes in volumes of water (LC/HF) or milk (HC/LF) to meet manufacturer recommendations. The calculation for macronutrient and total caloric composition for the HC/LF shake included the nutrition from the 2% milk that the shakes were made with to ensure that the shakes were isovolumetric and isocaloric in both conditions. Consumption adherence was assessed in each session by direct observation by the researchers.
Plasma processingWithin 5 min of phlebotomy, whole blood samples were centrifuged at 1500 x g for 10 min to separate the plasma. 40µL of a protease inhibitor cocktail (Halt™ Protease Inhibitor Cocktail 100x, Thermo Fisher Scientific, Inc.) was added to the plasma sample which was then vortexed and separated into three cryovials for subsequent storage at -80 °F. Fluorescence values for insulin, glucagon, GLP-1, and GIP were obtained using the Human Metabolic Hormone Magnetic Bead Panel multiplex kit (Millipore Sigma, Cat. #HMHEMAG-34 K) and a MAGPIX™ Multiplex Reader (Luminex Corporation, Austin, Texas, USA). Standard curves were created from the diluted standard fluorescence values and concentrations for each plasma sample value were interpolated.
Assay precision and variabilityTo assess assay precision, intra-assay and inter-assay coefficient of variation (CV) values were calculated for insulin, glucagon, GIP, and GLP-1. Intra-assay CV was determined by calculating the mean and standard deviation of duplicate wells for each sample, while inter-assay CV, reflecting variability across different assay runs, was calculated from quality control samples measured across six plates. The intra-assay CV for all analytes ranged from 6.0 to 8.4%, and the inter-assay CV ranged from 4.5 to 13.4%, consistent with the manufacturer’s reported assay performance.
Statistical analysisThe a priori sample size for this study was calculated to detect a 25% difference in the area under the BHB concentration curve between conditions. Based on an alpha of 0.05, a power of 85%, and a moderate effect size of 0.66, we determined that 24 participants were needed for adequate statistical power. The statistical software package R was used to calculate the sample size for the study based on the above parameters. An effect size of 0.66 is considered moderate, which is typical for human randomized crossover trials in this field [37]. Participants were recruited until 24 individuals completed the entire study.
Data are presented as means with standard deviations. Prior to analysis, each variable was assessed for normality using the Proc Univariate procedure in SAS to determine both skewedness and kurtosis. All variables were normally distributed except for GIP and glucagon, which exhibited positive skewness. To address this skewness, we conducted analyses both with and without log transformation and compared the results. Log transformation diminished the skewness of the data but did not alter the interpretation of the results compared to the non-log transformed data. Therefore, for ease of interpretation, we present the results from the non-log transformed data in this paper.
To assess differences in the area under the glucose and BHB curves, a linear mixed model for repeated measures using Proc Mixed in SAS was employed. The trapezoidal rule was applied to calculate the area under the curve (AUC) for each treatment, with AUC serving as the dependent variable to represent the overall intensity of the response. The AUC for glucose was calculated over two separate intervals: the first three hours following the administration of the pre-fast snack, and then for the entire 24-hour fasting period.
A linear mixed model for repeated measures using Proc Mixed in SAS was also utilized to evaluate both the main and interactive effects of condition and time across the 24-hour fast. This analysis was repeated to assess the main and interactive effects of condition and time from baseline to 24 hours post-fasting (t = 48) for both fasting conditions. The latter analysis aimed to investigate the residual effects of the two different fasting protocols on all variables of interest under similar conditions (ad libitum feeding followed by an overnight fast). In the model, ‘participant’ was included as random effects, allowing us to examine mean differences between conditions (as fixed effects) while also accounting for the variability or correlation structure among repeated measures within subjects (as random effects). A compound symmetry variance structure was used, and we applied the Kenward-Rogers degrees of freedom adjustment to correct for heterogeneity in variances and correlations. In this analysis, glucose levels were measured every 15 min, resulting in 96 total observations over the 24-hour period. In contrast, beta-hydroxybutyrate (BHB) was measured at six time points (baseline, 1, 4, 8, 12, and 24 h), and GLP-1, GIP, insulin, and glucagon were assessed at three time points (0, 1, and 24 h) and at two time points in an additional analysis (0, and 48 h).
Significant effects (p ≤ 0.05) were further evaluated using the least squared means method to obtain post-hoc pairwise comparisons using a Tukey adjustment to control for familywise error rate. F-values represent the overall main and interactive effects, while t-values reflect post-hoc pairwise comparisons. All statistical analyses were conducted using SAS software version 9.4 for Windows.
Comments (0)