
Remember me






Using the most recent DHS from 21 SSA countries, which was conducted between 2015 and 2022, a cross-sectional pooled dataset was used. Angola (2015–16), Benin (2017–18), Burundi (2016–17), Cameroon (2022), Ethiopia (2016), Gabon (2019–21), Gambia (2019–20), Guinea (2018), Kenya (2022), Liberia (2019–20), Mali (2018), Malawi (2015–16), Nigeria (2018), Rwanda (2019–20), Sierra Leone (2019), Senegal (2019), Tanzania (2022), Uganda (2016), South Africa (2016), Zambia (2018), and Zimbabwe (2015) were among the 21 SSA countries whose DHSs were utilized. In order to determine the pooled prevalence of CBF and the factors that are associated with it in the SSA countries, the data were appended. Each country’s survey has different datasets, such as those for males, females, children, births, and households. The kid’s record (KR) file was employed in this investigation. The DHS is a national survey that is often conducted in low- and middle-income nations every five years. Each country’s survey has different datasets, such as those for males, females, children, births, and households. The kid’s record (KR) file was employed in this investigation. The DHS is a national survey that is often conducted in low- and middle-income nations every five years. By using common methods for sampling, questionnaires, data collection, cleaning, coding, and analysis, it enables cross-national comparison [28].
The study comprised a weighted sample of 44,423 children between the ages of 12 and 23 months (Table 1). The DHS uses a two-stage, stratified sampling method [29]. The first step is creating a sample frame, which is a list of enumeration areas (EAs) or primary sampling units (PSUs) that encompass the entire nation. This list is typically created using the most recent national census that is available. The systematic sampling of the homes included in each cluster, or EA, is the second step. More details on survey sample techniques are available in the DHS guidelines [30].
Table 1 Sample size for continued breastfeeding and its associated factors among children aged 12 to 23 months in sub-Saharan African countriesVariables of the study Outcome variablethe outcome variable was continued breastfeeding, and it is the percentage of children 12–23 months of age who were fed breast milk during the previous day [27]. It was measured based on the maternal report and coded as 1 “if the child fed breast milk during the previous day” and 0 “otherwise.”
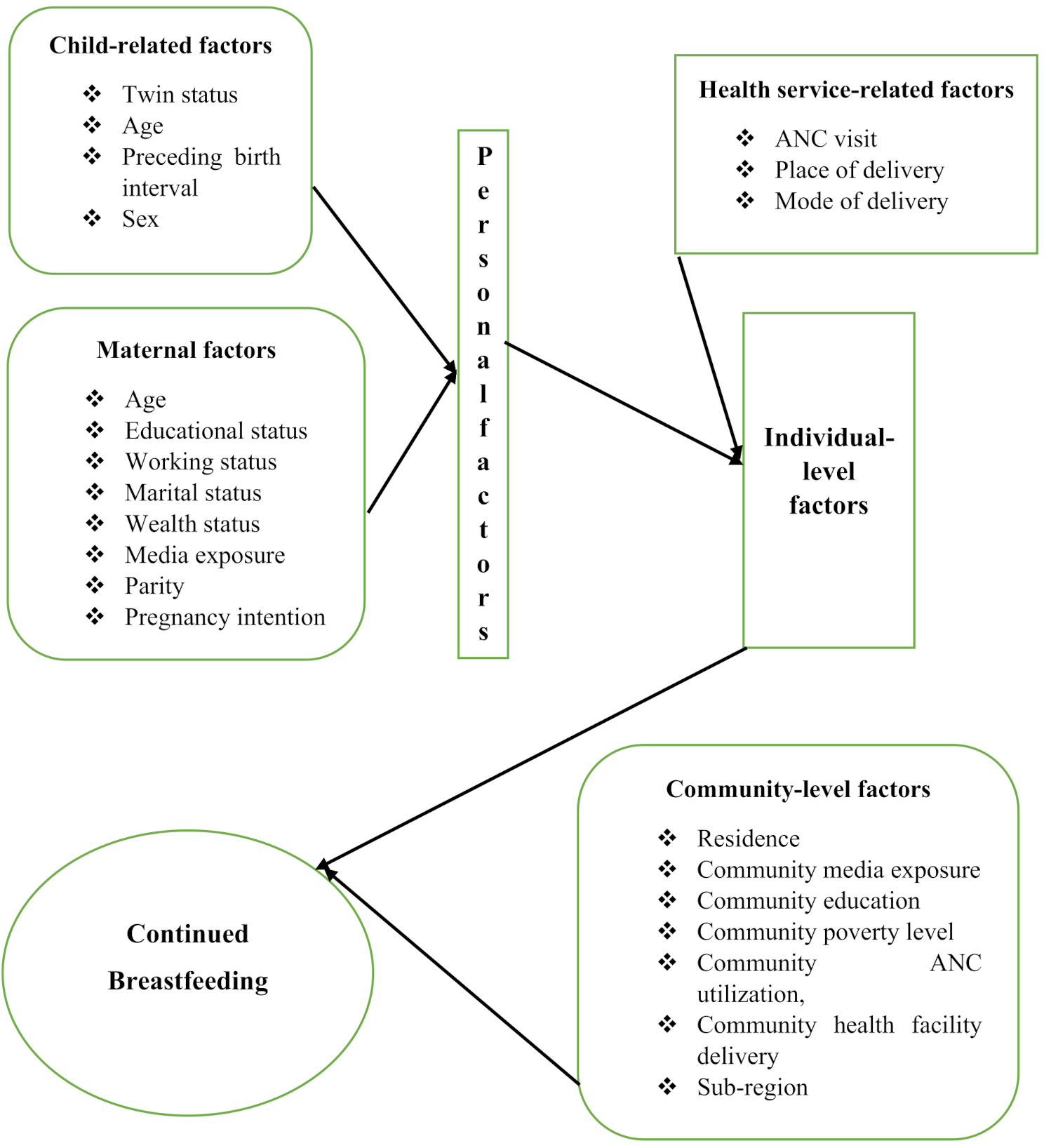
Explanatory variablesboth individual and community-level variables were considered in this study. Individual-level factors: maternal age, maternal education, paternal education, maternal working status, marital status, household wealth status, media exposure, parity, pregnancy intention, ANC visit, place of delivery, mode of delivery, twin status of the child, age of the child, preceding birth interval, and sex of the child. Community-level factors: place of residence, community-level media exposure, community-level education, community poverty level, community level of ANC utilization, community level of delivery at a health facility, and sub-region (Fig. 1). These factors were created by aggregating individual-level factors, as these factors were not directly accessible from DHS data (Table 2).
Fig. 1
Conceptual framework for factors associated with continued breastfeeding among children aged 12 to 23 months in sub-Saharan African countries
Table 2 Description and categorization of independent variablesData management and analysisSTATA/SE version 14.0 statistical software was used to clean, recode, and analyze data that was taken from the most recent DHS data sets. To control for non-responses and sampling errors, a sample weight was used. After categorizing continuous variables, categorical variables underwent additional reclassification. The results were presented in frequencies and percentages using descriptive analysis. Descriptive statistical methods were used to portray the variables at the individual and community levels. The variables in the DHS data were arranged into clusters; homes were nested within 1692 clusters, and 44,423 children are nested within households. In order to use the conventional logistic regression model, the presumptions of independent observations and equal variance across clusters were broken. This suggests that accounting for between-cluster effects requires the use of a complex model. To ascertain the factors associated with CBF, multilevel mixed-effects logistic regression was employed. The null model (outcome variable only), model I (only individual-level variables), model II (only community-level variables), and model III (both individual and community-level variables) are the four models that multilevel logistic regression uses. The null model, which is the model devoid of independent variables, was employed to examine the CBF variability throughout the cluster. Evaluations were conducted on the relationships between the outcome variable and the factors at the individual (Model I) and community levels (Model II). The link between the community-level and individual-level factors was fitted alongside the outcome variable (CBF) in the final model, or Model III. Missing data on breastfeeding is treated as not currently breastfeeding in the numerator and included in the denominator.
Through the use of the intra-class correlation coefficient (ICC) and proportionate change in variance (PCV), the magnitude of the clustering effect and the extent to which community-level factors explain the unexplained variance of the null model were assessed. The best-fitting model was determined to be the one with the lowest deviation. Ultimately, factors were deemed statistically significant when they had a p-value of less than 0.05 and an adjusted odds ratio (AOR) with a 95% confidence interval (CI) associated with CBF. A variance inflation factor (VIF) lying within acceptable bounds of 1–10 was used to test for multicollinearity amongst covariates, demonstrating the lack of significant collinearity among independent variables.
Random-effect resultsThe methods of estimating random effects or measures of variation of the outcome variable were the PCV, ICC, and median odds ratio (MOR). The ICC and PCV were used to measure the variation between clusters. Using clusters as a random variable, the ICC reveals that the variation of CBF between clusters is computed as ICC = VC/(VC + 3.29) × 100%. When two clusters are randomly chosen using clusters as a random variable, the MOR is the median value of the odds ratio between the area of the highest risk and the area of the lowest risk for CBF; MOR = ? 0.95√VC. Furthermore, the PCV illustrates the variation in the CBF prevalence that may be attributed to variables. It is calculated using the following formula: PCV = (Vnull-VC)/Vnull × 100%, where Vnull represents the null model variance and VC stands for cluster-level variance [31]. The relationship between the probability of CBF and independent variables at the individual and community levels was estimated using fixed effects.
Comments (0)