
Remember me

Most patients with HIES have a previous occurrence of a rash that appears in newborns, which typically starts during the first month after birth [8]. About 67% of these patients develop a rash consisting of papules and pustules before they turn two months old, and around 71% of them develop a rash within two weeks after birth [10].
The histological examination of the affected skin in patients with HIES reveals the presence of eosinophilic spongiotic dermatitis, eosinophilic folliculitis, and perivascular dermatitis with a significant number of eosinophils observed in the superficial and deep layers [9].
Initially, many of these patients with HIES were misdiagnosed with neonatal acne because the papules and pustules started on the face and scalp, similar to neonatal acne. However, unlike neonatal acne, the rash gradually affects the entire upper body [8]. Neonatal acne is a term that is commonly used interchangeably with neonatal cephalic pustulosis [32]. It is essential to differentiate between HIES rash and neonatal acne because of the different courses of the rash. Sometimes, the rash associated with HIES develops into eczema and can have a prolonged course [32]. However, in some patients with HIES rash, treatment with oral antibiotics or topical corticosteroids can improve or resolve the rash [13].
The appearance of the rash and its distribution on the skin of newborns with HIES is also comparable to a skin condition known as eosinophilic pustular folliculitis of infancy [32]. The onset is usually older in eosinophilic pustular folliculitis, with most cases occurring between ages 5 and 10 months rather than in the first month [33]. It does not usually improve with antibiotics. However, it does improve with topical steroid treatment [34].
Other conditions, such as transient pustular melanosis and erythema toxicum neonatorum, should also be considered regarding pustules during the newborn period [32].
Compared to HIES, the pustules observed in transient pustular melanosis are typically more shallow and soft and usually disappear with the formation of erythematous macules [35].
The appearance, onset age, distribution, and histological features of erythema toxicum neonatorum can resemble the newborn rash observed in HIES. It typically manifests within the initial two days of life and resolves within five days. In some cases, mild reoccurrences may occur within 5 to 10 days after the initial outbreak [36]. Similar to the newborn rash of HIES, erythema toxicum neonatorum can be present at birth [36].
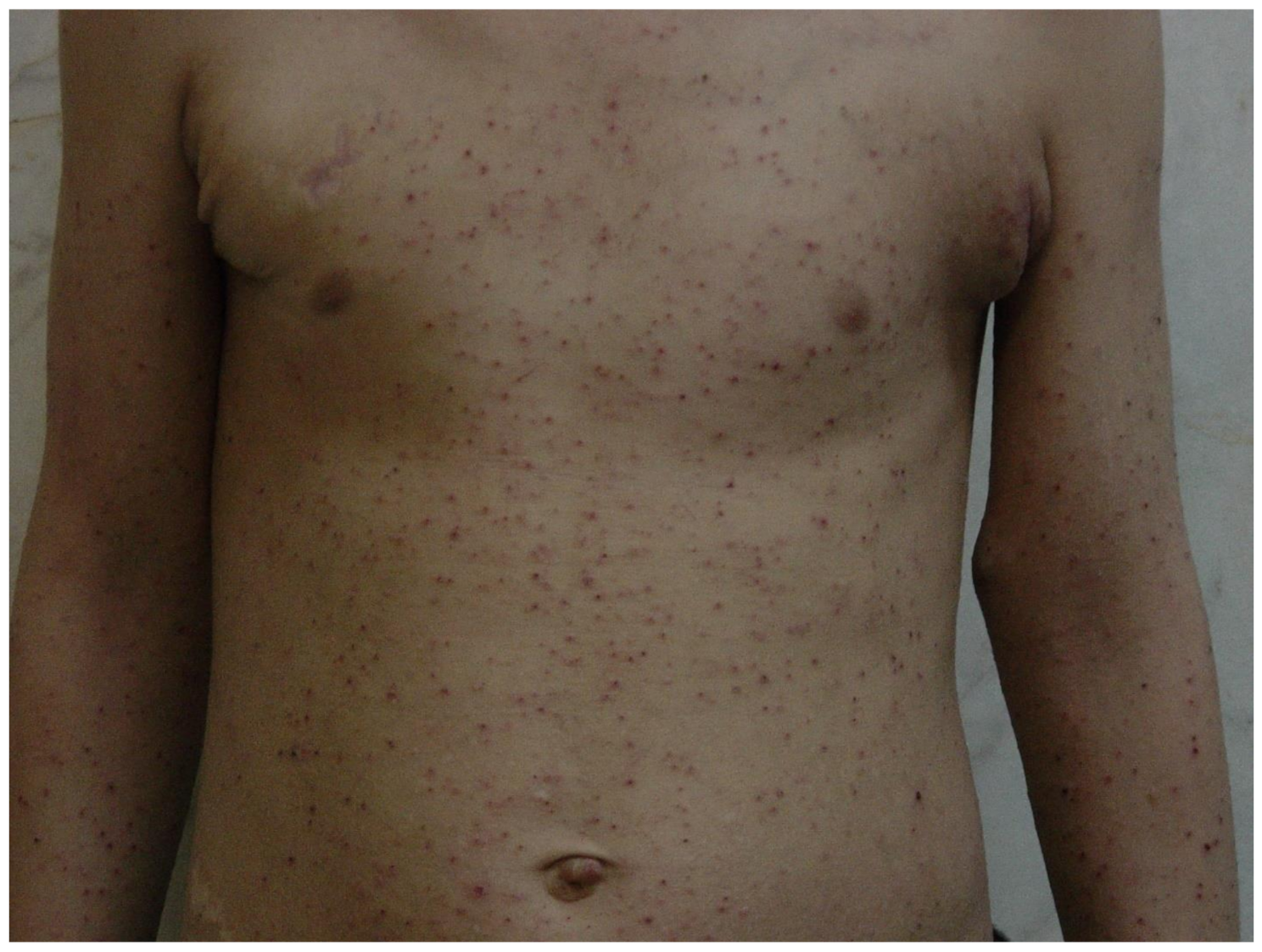
Most people with HIES commonly experience symptoms within the spectrum of a papulopustular rash and eczematous dermatitis (Fig. 1) [10]. Research indicates that approximately 65% of individuals diagnosed with HIES fulfill the criteria for atopic dermatitis, a common form of eczema. Furthermore, HIES and atopic dermatitis typically involve the presence of itching (pruritus) as a shared symptom [8, 9]. Individuals affected by HIES typically do not exhibit additional symptoms, which are commonly associated with allergies, such as hay fever or asthma. Moreover, they usually do not have a family history of atopy, defined as a predisposition to allergic conditions [37].
Fig. 1
Generalized erythematous and excoriated papules suggesting an eczematous dermatitis in a 10-year-old boy with HIES
The neonatal rash is a critical symptom that appears in most individuals with HIES. Given that the distribution, appearance, and histologic characteristics of the neonatal rash in HIES are similar to other skin conditions, it is crucial to differentiate HIES from similar conditions for an accurate diagnosis and appropriate treatment. Therefore, healthcare professionals should be aware of the distinct features of neonatal rash in HIES to provide adequate care for affected individuals.
Mucocutaneous candidiasisCandida species, particularly Candida albicans, are fungi that commonly inhabit the skin and mucous membranes of the gastrointestinal and genitourinary tracts in a significant portion (around 30–50%) of healthy individuals within a given population at any given time. Most individuals experience colonization by Candida at some point in their lives. The human body’s natural defense mechanisms normally prevent this fungus from causing illness; however, if there is a breakdown in the skin or mucosal barriers, imbalances in the microbiome, or defects in the immune system, the risk of developing severe candidiasis, either on the skin or mucous membranes, or invasive candidiasis increases [38].
Superficial candidiasis which affects the mucous membranes and skin is very common. It can occur in individuals with weakened immune systems and those with a healthy immune system. In most cases, these Candida infections that affect the skin, nails, oropharyngeal mucosa, esophagus, and genital tract are sporadic and not severe [39].
Approximately 60% of individuals with HIES suffer from chronic mucocutaneous candidiasis, characterized by recurring fungal infections in the mucous membranes and skin. This symptom can be effectively controlled by employing a combination of antifungal medications administered orally and topically [10].
A significant reduction in the production of Th17 cells has been consistently observed in patients diagnosed with HIES [40, 41, 42]. More recent reports have highlighted that individuals experiencing recurrent mucocutaneous candidiasis, accompanied by decreased Th17 cell production, can be attributed to CARD9 [32] and DECTIN1 [33] gene mutations.
PsoriasisPsoriasis is uncommon in pediatric patients with HIES. While the association between psoriasis and HIES has been rarely reported, it is believed that the autoimmune nature of psoriasis can lead to its manifestation in individuals with immunodeficiency diseases [43].
The immune microenvironment in HIES lesions appears to be disrupted, leading to an imbalance of Th1/Th2 cytokines [6]. This imbalance can have effects beyond eczema dermatitis and may contribute to the development of additional changes. Psoriasiform lesions observed in HIES patients could be attributed to this dysregulation. Additionally, the recurrent infections commonly experienced by individuals with HIES can also be a potential contributing factor to the occurrence of psoriasiform lesions in these patients [43]. Further research is needed to fully understand the underlying mechanisms and relationship between immune dysregulation, recurrent infections, and the development of psoriasiform lesions in HIES.
There have been two reported cases of psoriasis and psoriasiform lesions occurring in patients with HIES. The first case was a 17-year-old boy with a history of recurrent skin inflammation and boils, who presented with severe and persistent erythroderma. The skin biopsy findings indicated thickened epidermis, increased production of skin cells, and the presence of neutrophils, Munro’s microabscesses, and immune cell infiltration, resembling the histological features of psoriasis [43].
The second case was a 16-year-old Iranian boy, who presented with a one-year history of white scaling papules on his knees and elbows, which were diagnosed as psoriasis based on a skin biopsy. Laboratory tests did not identify any genetic or molecular defects. Treatment included inhaled corticosteroids, bronchodilators, antibiotic prophylaxis, and occasional intravenous immune globulin (IVIG). The biopsy showed hyperkeratosis, parakeratosis, and elongated rete ridges in the epidermis, confirming the psoriasis diagnosis [44].
In conclusion, psoriasis is a noteworthy manifestation in the pediatric population with HIES, albeit a rare occurrence. Additional studies are needed to understand the connection between psoriasis and HIES in order to shed more light on the underlying mechanisms and potential treatment approaches for this unique patient population.
AbscessesCold abscess in considered an important clue for diagnosis of HIES. Cold abscesses can often be mistaken for cysts or benign tumors. Although these abscesses may not show typical signs of inflammation, they can be large and are usually caused by S. aureus [45]. Fortunately, the incidence of cold abscesses in HIES patients has decreased due to early administration of antibiotics and prophylactic anti-staphylococcal antibiotics [32].
Patients with HIES have been found to have diminished acute-phase responses, such as decreased serum levels of C-reactive protein during infections. This could be due to defective signaling of IL-6, as the protein STAT3, which is involved in IL-6 signaling, is important in producing acute-phase proteins. This phenomenon’s exact molecular mechanism has yet to be fully understood [46]. However, it is known that HIES patients frequently experience recurrent skin infections with S. aureus, which can develop “cold” abscesses that lack typical signs of inflammation, such as warmth and redness. This is a nearly universal feature of HIES [32, 47].
Healthcare providers need to be aware of HIES symptoms and consider this syndrome in cases of recurrent abscesses.
Cutaneous fusariosisFusarium species are molds found everywhere, which can cause infections in humans, but the risk of infection depends on the person’s immune system. Fusarium infection is usually limited to certain areas, such as the cornea, nails, and skin in people with a healthy immune system.
However, in patients with severe neutropenia, exposure to corticosteroids, or those who have had a hematopoietic stem cell transplant, even minor skin lesions can lead to the spread of the fungus throughout the body, known as secondary disseminated Fusariosis. This can cause necrotic skin lesions and fungemia (the presence of fungus in the blood), which are associated with high mortality rates [48, 49, 50].
A recent report discussed a rare condition known as primary invasive cutaneous Fusariosis, which was observed in four patients with a specific genetic mutation called STAT3 dominant negative (DN). The infection primarily affected the extremities and was characterized by long-term involvement confined to the skin and subcutaneous layers, without spreading to other parts of the body. In all patients, Fusarium solani, a type of fungus, was identified through positive skin fungal cultures. Furthermore, one patient exhibited an eosinophilic inflammatory infiltrate in the deep subcutis [51]. The tissue abnormalities and defects in the immunological skin barrier found in STAT3 DN patients may explain the development of Fusarium skin disease [30]. Research has indicated the essential role of STAT3 in skin remodeling and maintaining its balance. In patients with STAT3 DN mutations, there is an impaired expression of IL-17 and reduced differentiation of Th17 cells. This leads to an increased susceptibility to epithelial infections and an imbalance in the skin microbiota [52, 53].
The clinical presentation and treatment response vary among the patients, underscoring the importance of utilizing multiple therapeutic approaches, such as topical antifungal medications. These case reports offer valuable knowledge about the underlying mechanisms and treatment of primary invasive cutaneous Fusariosis in individuals with STAT3 DN mutations. The findings emphasize the need to consider primary invasive cutaneous Fusariosis as a potential diagnosis in patients with persistent skin lesions and underlying immune deficiencies, particularly those associated with STAT3 DN mutations. Further research is required to comprehensively understand the range of cutaneous fungal infections in immunocompromised patients and to develop effective treatment strategies.
Lesions similar to atopic dermatitisAtopic dermatitis, also called atopic eczema, is a prevalent chronic inflammatory condition that affects many people in wealthy countries, and approximately 20% of children [54]. It causes itching, dry skin, and eczematoid skin lesions [55, 56].
Table 1 A comparison between atopic dermatitis and hyper IgE syndrome in the pediatric populationA combination of genetic, immunological, and environmental factors causes atopic dermatitis. The exact cause is not yet fully understood, but it leads to a compromised skin barrier, allowing allergens, irritants, and microorganisms to enter the skin and trigger an immune response. Several genetic mechanisms have been identified as contributing to the risk of developing atopic dermatitis, with loss-of-function mutations in the FLG gene being the most consistently reported variants. This highlights the importance of the skin barrier, as the filaggrin protein found in the epidermis plays a significant role in its structure and function [58, 59]. Filaggrin is a protein found in the granular layers of the epidermis, and during the process of keratinocyte differentiation, it is broken down into several identical filaggrin molecules. These molecules then combine to create a strong protein-lipid matrix that protects the skin by preventing water loss and blocking the entry of harmless allergens and infectious microorganisms [32].
Eczematous lesions, intense itching, and a chronic or relapsing disease course characterize atopic dermatitis. The distribution of eczematous lesions varies with age. Infants often have acute lesions that appear as poorly defined redness, swelling, blisters, and clear fluid oozing. These lesions can be widespread but typically affect the face, cheeks, and trunk and do not usually involve the diaper area. In childhood (starting at age 2), eczema becomes more localized and chronic, with paler redness, dry skin, and poorly defined lesions that often affect the flexor surfaces and may thicken (lichenification) in chronic areas [60].
Various studies have reported different descriptions of the skin manifestations in HIES. For instance, one study described them as “infected eczematoid skin lesions [63], while others characterized them as a type of dermatitis that resembled atopic dermatitis but had some atypical features [57, 30].
Despite these varying descriptions, all previous studies have consistently reported that almost all.
HIES patients display skin manifestations that resemble atopic dermatitis or eczema [57, 63, 64, 65].
Skin manifestations of both HIES and atopic dermatitis are characterized by high serum IgE levels and eosinophilia. In HIES, the rash is typically papular and itchy and often exhibits lichenification, a thickening of the skin resulting from hypertrophy of the epidermis. The clinical and histopathological features of HIES rash are very similar to those of atopic dermatitis, but there are reported differences in the distribution of the rash. In atopic dermatitis, the rash typically affects the flexural surfaces of the body, while in HIES, it is located on the face and extensor surfaces. However, the location of atopic dermatitis can change with age, so it is unclear, whether or not the previously reported differences are due to an essential difference between the two conditions [61].
Atopic dermatitis is frequently linked to other allergic disorders, including food allergy, asthma, and allergic rhinitis, which are not typically present in most cases of HIES, particularly those involving STAT3 deficiency [62].
Staphylococcal infections are usually superficial in atopic dermatitis, while HIES patients develop deep-seated abscesses. Mucocutaneous candidiasis is also a common complication of HIES but not atopic dermatitis. The onset of skin lesions in atopic dermatitis usually occurs after two to four months of age, while symptoms of HIES typically present before one month [61].
Skin abnormalities in hyper-IgE syndrome (HIES) extend beyond skin lesions resembling atopic dermatitis. Staphylococcus aureus colonization frequently takes place, leading to more severe dermatitis when infection sets in. Although acute episodes can be managed with treatment, recurrent episodes are likely to happen unless prophylactic antibiotics are taken. In addition, many HIES patients exhibit a rough texture in their facial skin, which is thick and doughy, despite having no history of severe acne. The underlying cause of this cutaneous manifestation is not yet fully understood, but it may be related to impaired skin remodeling [32].
A comparison between Atopic Dermatitis and hyper IgE syndrome in the Pediatric Population is provided in Table 1.
Squamous cell carcinomaSquamous cell carcinoma is a type of cancer, originating from keratinocytes, the cells found in the epidermis or squamous mucosal epithelium. It is a malignant tumor that can spread to other body parts if left untreated [66]. Squamous cell carcinoma commonly develops in areas of the skin that have experienced chronic irritation, such as burns or scar tissues, long-standing non-healing wounds, exposure to x-rays, or contact with certain chemical substances like arsenic and petroleum. Factors like chronic and recurrent infections and prolonged suppression of the immune system have also been identified as potential risk factors for the development of squamous cell carcinoma [66].
Recent research has highlighted the crucial role of the immune system in cancer prevention through a process called the immune surveillance [67]. Immunosuppressed individuals, including those with HIES, are reported to have a higher incidence of SCC [68].
Pediatric cases of head and neck carcinoma are infrequent occurrences. If a chronic ulcer displays signs of excessive growth beyond what is normally observed during the healing process, it should raise concerns about potential malignant transformation [66].
HIES patients face an elevated risk of developing malignancies, including lymphomas. Furthermore, patients with DOCK8 deficiency, a subtype of HIES, have shown susceptibility to papillomavirus-induced SCC and lymphomas [69].
The clinical presentation of SCC in HIES patients can vary, with symptoms often manifesting as chronic ulceration or non-healing wounds demonstrating atypical proliferation. The choice of treatment modality depends on several factors, including tumor differentiation, metastasis, size, shape, location, and predisposing factors. Surgical interventions, such as excision surgery, Mohs surgery, cryosurgery, electrosurgery, and radiation therapy, are among the available treatment options [70].
To illustrate the complexities of SCC in HIES, a reported case of a 17-year-old patient with a history of eczema, recurrent middle ear infections, and a family history of leukemia is worth mentioning. The patient demonstrated multiple clinical manifestations of HIES, including immune deficiency, eosinophilia, and elevated IgE levels. Over several years, the patient experienced recurrent otitis media, purulent ear discharge, and subsequent complications, leading to the diagnosis of SCC originating from the external auditory canal [69]. The case underscores the importance of comprehensive management and regular follow-ups in HIES patients.
The association between HIES and skin malignancies, particularly squamous cell carcinoma, highlights the complex interplay between immunodeficiency, chronic infections, and genetic predisposition. Early diagnosis, active surveillance, and appropriate treatment strategies are crucial in managing SCC in HIES patients [68]. Further research is needed to unravel the underlying mechanisms and develop targeted therapeutic approaches to improve outcomes for individuals with HIES and associated skin malignancies. Please see Table 2 for a brief summary and comparison of dermatologic presentations of hyper IgE syndrome in children.
Table 2 A comparison of dermatologic presentation of hyper IgE syndrome in the pediatric population
Comments (0)