AD is a chronic, heterogeneous, and inflammatory skin disorder characterized by diverse clinical phenotypes and courses. The pathophysiological mechanisms of AD involve complex interactions between genetics, immune system dysregulation, and environmental factors. AD is predominantly Th2 driven, and other cellular subsets such as Th1, regulatory T cell, Th17, and Th22 cells contribute to immune activation [7]. Development of allergic diseases including AD in a patient received HSCT also has been reported [1,2,3, 8,9,10]. Th2-biased immune reconstitution after HSCT has been suggested. It could be the acquisition of T cells in recipients are biased toward Th2-screwed immune response due to genetic and/or environmental factors in the donors. After HSCT, mature memory cells are replaced by cells derived from donor hematopoietic progenitor cells [11]. Marrow-derived immune cells from allergic donors may transfer allergic diseases [1, 12]. Th2 cytokine like interleukin (IL)-4 and IL-10 may be up-regulated in HSCT recipients [13]. In addition, systemic tacrolimus for post-transplantation immunosuppression was associated with Th1/Th2 imbalance with predominance of Th2 response and was implicated as a potential trigger of allergic disease [14–15]. However, sustained Th2-biased response as a consequence of HSCT is unlikely because allergic disease is not commonly reported after HSCT. The patient in this case did not receive tacrolimus for GVHD prophylaxis, and AD might occur sporadically after HSCT.
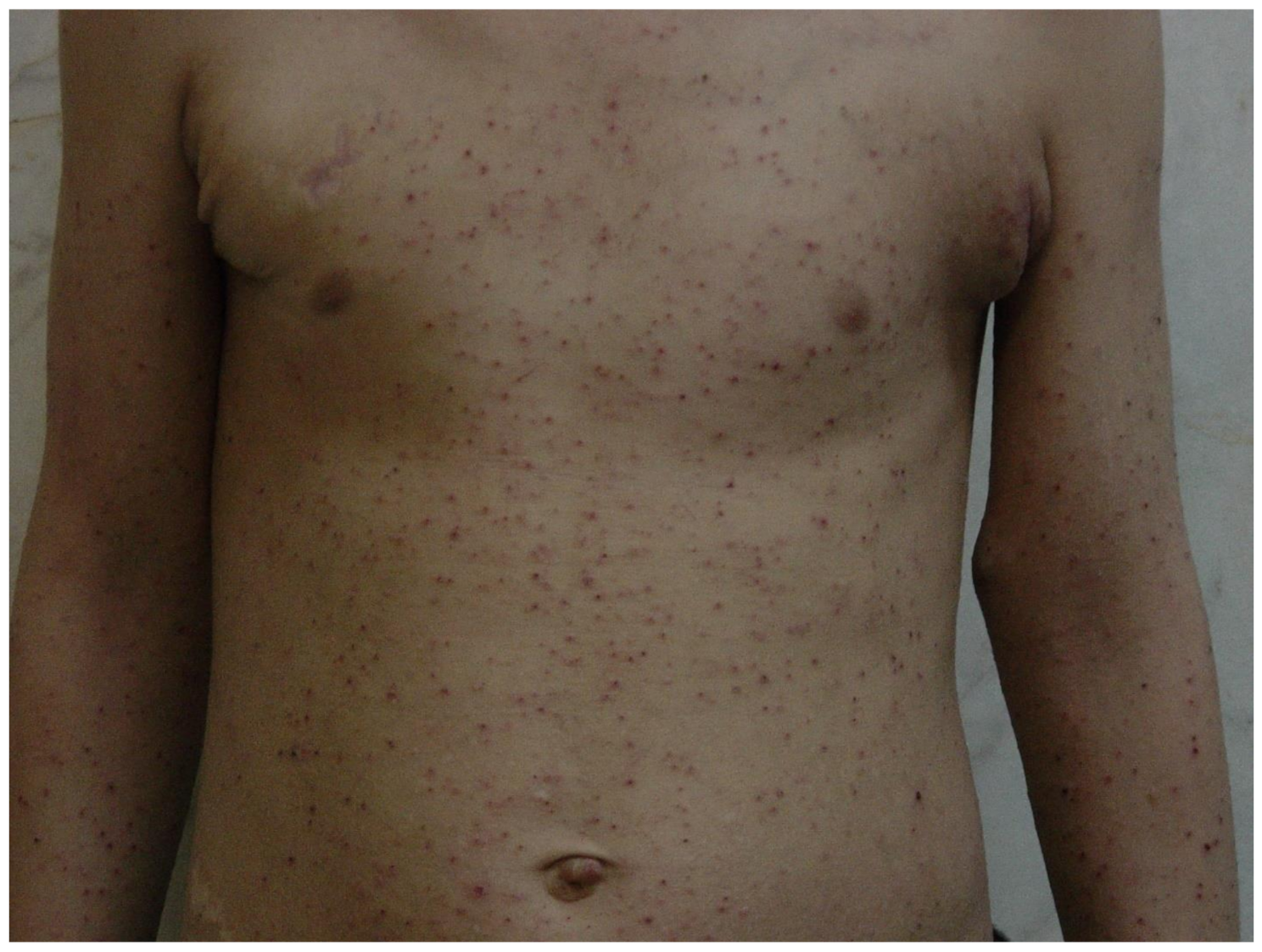
Dupilumab is a monoclonal antibody that blocks IL-4 and IL-13, the key drivers of Th2-mediated inflammation. It was the first biologic approved for moderate-to-severe AD. Dupilumab has demonstrated efficacy and safety in clinical trials and real-life clinical settings. Several cases of AD or AD-like graft-versus-host disease (GVHD) that develop after HSCT have been successfully treated with dupilumab [16,17,18]. In previous reports [16,17,18], eczematous dermatitis developed usually between 1 and 5 months after HSCT. Dupilumab therapy showed a rapid clinical response after 1 month, with nearly complete clearance observed after 4 months, and the discontinuation of other immunosuppressive therapies. The patient in this case experienced AD 3 months after HSCT and was refractory to systemic immunosuppressants, such as corticosteroids, cyclosporine, and methotrexate. However, the patients showed complete resolution of the cutaneous manifestations, and systemic immunosuppressants were discontinued after dupilumab therapy. To our knowledge, this patient had the longest duration of follow-up reported for dupilumab therapy (36 months), without disease flares or adverse reactions. AD-like GVHD, a subtype of GVHD, occurs after HSCT and is similar to de novo AD in terms of clinical and histological features, including a predominant Th2 immune response [19, 20]. Therefore, distinguishing AD-like GVHD from other cutaneous disorders, including AD, eczematous GVHD subtype, or eczematous dermatitis, can be challenging. Patients with AD-like GVHD have clinical features usually characterized by no atopic history, no donor-related atopy, and a good response to conventional treatments, such as systemic corticosteroids and immunosuppressants [20, 21]. However, the patient was refractory to conventional treatments, and the donor had AD prior to transplantation. More than two dermatologists observed the patient for 11 years after the onset of eczema. Finally, the patient was diagnosed as AD based on the clinical evaluations, although skin biopsy was not performed.
AD can develop after HSCT, and dupilumab shows rapid, long-term efficacy and safety in refractory cases.


Comments (0)