Addressing the commercial determinants of health, defined as “strategies and approaches used by the private sector to promote products and choices that are detrimental to health” [1], through regulatory actions has been identified as a priority to achieve the sustainable development goals [2]. However, the implementation of transformative and effective policies remains scarce worldwide [3]. The proliferation of International Investment Agreements (IIAs), as the result of globalization, has been identified as one of the factors contributing to this policy inertia or chill on meaningful public health policy action [4,5,6,7].
Bilateral investment treaties (BITs), the most common form of IIAs, are treaties signed by two States to promote and protect cross-border investments [8]. They provide a series of protections to foreign investors under international law, including fair and equitable treatment and the right to obtain compensation in case of direct and indirect expropriation [9]. A key feature of most BITs is the inclusion of an Investor-State dispute settlement (ISDS) mechanism which enables investors to use a form of private international arbitration to pursue compensation from States if governments implement measures that infringe the dispositions of the treaties [10]. This mechanism has been used to challenge health policy measures globally, such as taxation, health insurance, water provision, environmental protection, and anti-tobacco regulations [11, 12].
The BITs signed in the 90s and beginning of 2000s, usually regarded as old generation BITs, included few provisions to protect the states’ regulatory and policy space, i.e., their ability to regulate, the scope and content of the policies and the mechanisms they can use to design and implement policies for achieving certain objective [13]. Three key mechanisms explain this potential negative effect of BITs. First, IIAs can limit the range of policy options available to governments for protecting and promoting health [14]. For example, shifting from public to private provision of health care services as a consequence of the implementation of a BIT can increase inequities with respect to access [15]. Further, provisions protecting patents for medicines can weaken national pharmaceutical policies [16]. Second, BITs can generate regulatory chill: out of fear of capital fright or ISDS cases, governments can alter, modify, or fail to enact effective public health policies [4, 5, 17]. This effect can extend beyond the country directly involved in an ISDS case, as other governments may delay or avoid introducing health policies while awaiting the outcome of similar cases elsewhere [18]. Third, ISDS mechanisms can also enable a high level of industry influence on national health policies by providing them with a strategy to require open participation in decision making [19].
In the wake of a growing number of ISDS cases, new generation BITs emerged in the decade of 2010s to protect the States right to regulate [13]. These BITs include more detailed and precise clauses [20]. One of their innovations has been the inclusion of health safeguards, i.e., specific clauses to protect the State’s right to regulate [14]. Health safeguards can be classified in three main groups: defensive, neutral, and progressive [21]. Defensive clauses intend to shield regulatory and policy space through the inclusion of clause-specific clarifications, exclusions and exceptions. Meanwhile, neutral clauses intend to respect and avoid the erosion of existing health policies. More recently, progressive clauses have emerged as an innovation to impose health-related obligations to foreign investors. This type of safeguards has been used in developing countries such as Brazil and Bangladesh [21, 22].
Recognizing the threat to health of IIAs, the United Nations Trade and Development (formerly known as UNCTAD) and the World Health Organization (WHO) have identified the protection of health policy within IIAs as a priority [13, 15]. Previous studies have analysed the inclusion of health safeguards in BITs [6, 14, 21, 23,24,25]. However, an in-depth understanding of the processes involved in the diffusion of health safeguards in BITs globally and the factors acting as barriers and facilitators for their uptake is still lacking. In this context, the present study intends to fill this research gap by analysing the uptake of health safeguards in the context of Uruguay, a developing Latin American country.
Study context and objectives
This study focuses on Uruguay, a small developing country located in the southeastern region of South America, between Argentina and Brazil. It has a population of 3,444,263 inhabitants and an area of 176,215km2 [26]. With a gross domestic product (GDP) of 23,090 US dollars per capita, it is categorized as a high-income country [27]. It stands out in the region by its low inequality (Gini index = 0.408), high human development index (HDI = 0.809) and political stability [28, 29]. Although Uruguay is classified as a high-income country based on GDP, it remains behind high-income nations in Europe, North America, and Oceania in key areas such as industrialization, infrastructure development, and labour market conditions [30]. As a result, it is generally categorized as a developing country or a developing market economy rather than a fully developed nation [30]. This distinction reflects structural economic challenges, including a reliance on primary industries, less advanced manufacturing sectors, and gaps in technological innovation and infrastructure compared to more industrialized economies.
Foreign direct investment has played an important role in the growth of the Uruguayan economy, contributing to the development and strengthening of its productive structure [31]. The country has made numerous efforts to attract foreign investors and is regarded as one of the least restrictive developing countries for foreign investment [32]. According to the most recent data, in 2023 foreign direct investment corresponded to 3.7% of the GDP (3,551 million US dollars) [33].
As part of the efforts to attract direct foreign investment, Uruguay approved an investment law in 1998, which declares national and foreign investment of national interest and establishes equitable treatment for foreign investors [34]. In addition, IIAs have been one of the strategies implemented by the country to attract foreign investment. It currently has 32 IIAs in effect with 34 developed and developing countries [35], including BITs with the most relevant countries in terms of direct foreign investment between 2022 and 2023: Spain, Finland, Switzerland, USA, Netherlands, Singapore, Canada, Germany [32, 33, 35].
Compared to other Latin American countries, Uruguay has limited experience with ISDS: it has only faced five ISDS cases, four of which have been decided in favour of the State and one is still pending [11]. Despite its relative limited experience with arbitration, the country has faced a high-profile case relevant for health public policy. Uruguay, recognized as a global leader in tobacco control [36], introduced in 2008 a new policy banning different presentations per brand families and mandating health warnings to occupy at least 80% of the package [37]. In response, in 2010, Philip Morris (PM) started an ISDS case against Uruguay claiming that the act constituted a form of indirect expropriation, allegedly infringing the dispositions of the Switzerland-Uruguay BIT (1988) [11]. In 2016, the tribunal dismissed all claims and ordered Philip Morris to pay the trial’s and Uruguay’s legal costs [38]. Considering that governments’ approach to BITs may be shaped by their experience with arbitration [4, 39], this high-profile ISDS case could have influenced the country’s approach to BITs. Previous research has shown that the case introduced policy chill to the anti-tobacco regulation in the country [4, 40]. However, no information has been published on its potential influence on IIAs and particularly the inclusion of health safeguards.
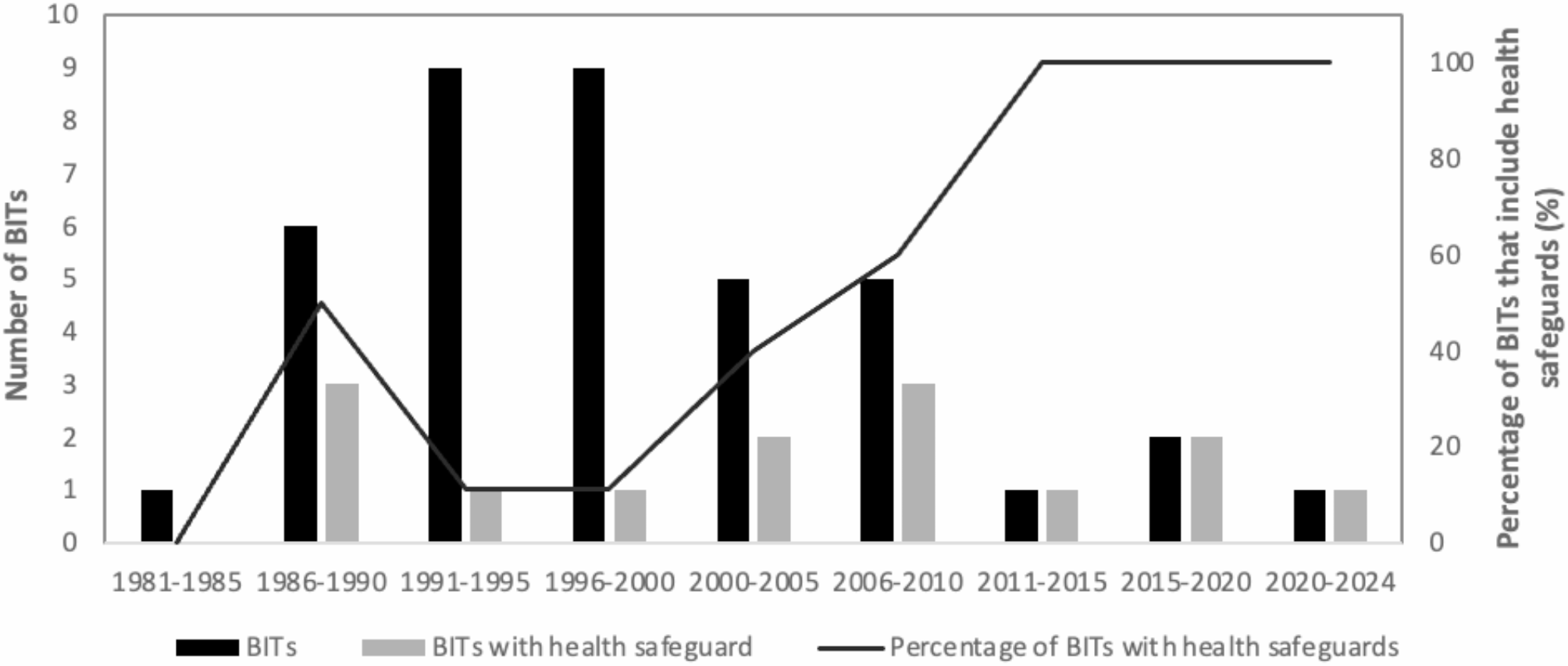
In this context, the objectives of the present work were to: (i) examine the evolution of the inclusion of health safeguards in the BITs signed by Uruguay until 2024, (ii) analyse how Uruguay has approached BITs after the Philip Morris ISDS case, (iii) explore Uruguayan stakeholders’ perspectives on the inclusion of health safeguards in BITs, (iv) identify barriers and facilitators for the uptake of health safeguards in the BITs.
Theoretical framework
The research draws on the diffusion of innovations theory [41]. The uptake of health safeguards in BIT is conceptualized as a policy innovation, i.e., “a novel practice used for policy design and development that result in better problem solving of complex issues” [42]. The diffusion of innovation theory is complemented with insights from theories of policy learning [43, 44], as well as international negotiation theories to account for the fact that BITs are the result of the negotiation between two countries [45, 46].
The theoretical framework suggests that the inclusion of health safeguards, has been gradually adopted by states as a consequence of a diffusion process, i.e., it has been communicated through communication channels over time among states. Therefore, the uptake of the innovation by a State is influenced by: (i) a national network of agents, including State agencies, State officials, and civil society organizations; (ii) internal determinants of policy arrangements, i.e., internal factors of a country that determine willingness to adopt a policy innovation and the characteristics of the implemented public policies, including socio-economic characteristics and institutional structures [41, 46, 47]; (iii) international networks through which diffusion occurs, including State-State interactions, international organizations and transnational bodies [43, 48]; (iv) intergovernmental negotiations between states, which are influenced by power and authority dynamics [46, 49]. This framework recognizes that the decision to adopt health safeguards within a BIT involves negotiation on two levels. First, the national level, where primarily the domestic governance dynamic needs to be investigated (in terms of actors, interests, ideas and discourse, and institutions). Second, on the intergovernmental level, where the negotiation process and the power dynamic between states become highly relevant [46].
Examining the uptake of health safeguards in the Uruguayan context enables the understanding of how diffusion took place in a global context and to identify factors that have acted as barriers and facilitators. Results are expected to provide insights to support the development of resources and tools to support the uptake of strong health safeguards in IIAs.






Comments (0)