
Remember me
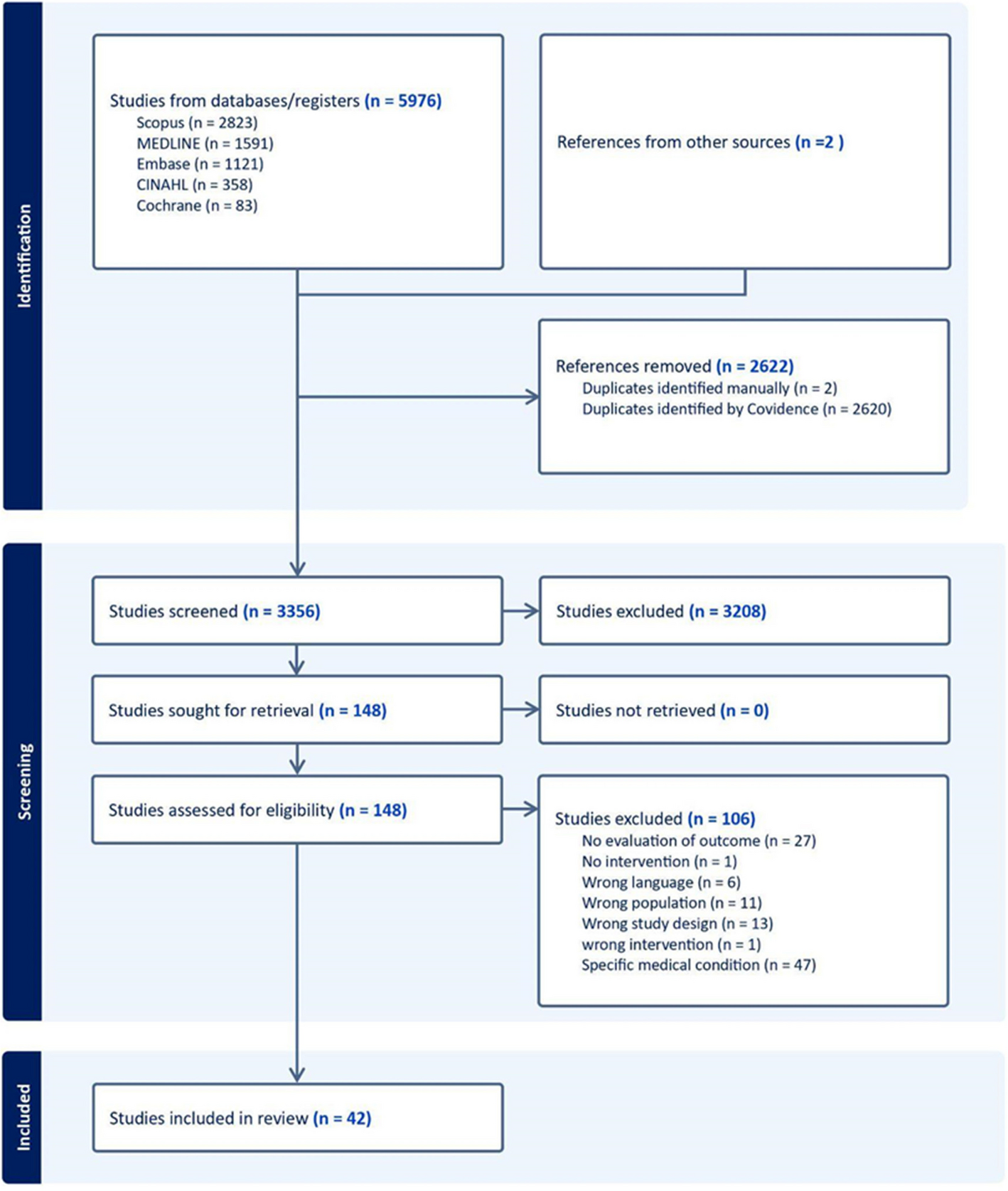





Our systematic search yielded 5976 records. After removal of duplicates, 3356 records remained. Two additional studies were obtained by consultation with experts in the field. After title and abstract and full-text screening, 42 studies were included, evaluating the effect of 38 unique TiC interventions/programs (Fig. 1).
Fig. 1 Characteristics of included studies
Characteristics of included studiesTable 1 displays the summarized characteristics of included studies. Most studies used a pre-post intervention design [21,22,23,24,25,26,27,28,29,30,31,32,33], while nine studies were randomized clinical trials [13, 34,35,36,37,38,39,40,41], four of which had a cluster-randomized design [38,39,40,41]. Most studies were conducted in high-income countries, mainly the United States, Australia, and Germany.
Table 1 Summarized characteristics of included studiesTypes of TiC interventionsDetailed descriptions of the included TiC interventions are shown in Table 2. There exists a range of TiC activities reported as part of the included programs and interventions. Many interventions aimed to support the RIM population in navigating the healthcare systems of host countries. These interventions typically followed one of two approaches: training community members about the healthcare system, available services, and pathways [27, 31, 37, 42,43,44] or utilizing culturally sensitive mediators who guided patients and their families to access appropriate services upon referral by healthcare providers [26, 41, 44,45,46,47,48,49]. Examples of the first approach include educating immigrants about the Danish healthcare system, training community members in the United States about available healthcare services, enhancing healthcare navigation skills among South-East Asian women in Taiwan, educating immigrants in Ontario, Canada about navigating the healthcare system and available services, and training Bhutanese refugee community members to navigate healthcare systems effectively. Examples of the second approach include involving facilitators to provide tailored action plans for refugees in Australia, coordinating care for immigrants in the United States through caseworkers and cultural mediators, supporting immigrant children with cancer and their families through various stages of their disease in Spain, utilizing caseworkers to provide culturally appropriate primary care for refugees in Canada, improving patient flow for refugees and asylum seekers in emergency departments in Australia with the help of nurses experienced in immigrant care, and addressing treatment-related cultural issues through transcultural mediation for families of immigrant children in France. Navigators, or interventions that train individuals to navigate the healthcare system, were among the most studied and effective TiC interventions to improve health outcomes.
Table 2 Description of TiC interventionsEducating and improving RIM populations’ health literacy was another significant activity of many TiC interventions. Some examples of health literacy areas that were targeted by TiC interventions included palliative and end of life care, oral health, mental health, vaccine acceptance, and pediatric health [21, 22, 28, 48, 56, 57]. Few studies showed the effectiveness of improving health literacy; these interventions demand considerable time, resources and patient engagement and health education skills.
There were programs and interventions that provided a combination of services and activities for RIM population, such as comprehensive health assessment and screening, consultation, primary care visit, referrals to other social and medical sectors, providing professional interpreters and culturally adapted and accessible services in specific fields such as mental health, chronic conditions, antenatal care, oral health, cancer and rehabilitation [20, 32, 44, 49,50,51, 55, 60, 61]. Examples of these programs offering a range of services to facilitate the smooth transition of RIM care in host countries include the Healthy Fit Program targeting general health among the Hispanic population in the United States [51], the multi-disciplinary management of non-communicable diseases among refugees in Jordan by Médecins Sans Frontières [50], physical assessments and referrals for newly arrived Latino immigrants in Charlotte, USA [52], the Healthy Kids Outreach Program targeting uninsured immigrant children [49], the AMOR program providing comprehensive care for immigrant children with cancer in Spain, an antenatal care program for immigrant women in Australia [44], a free mental health program for Palestinian refugees in Lebanon [60], and the “Bridging the Gap” initiative focusing on women’s health among refugee women in Australia [61]. These promising, population-focused interventions enhance health outcomes, but they require intensive community collaboration, organizational trust, and time to show TiC improvement.
Target recipients of TiC interventionsThe majority of TiC interventions targeted patients and/or their families [13, 21, 22, 25, 26, 28,29,30,31,32,33,34,35,36,37, 42,43,44, 46, 48,49,50,51,52,53,54,55,56,57,58,59, 61], whereas some interventions targeted both the patient and the provider (Table 1) [23, 24, 39, 45, 47, 50, 60]. For example, in the “Transcultural Mediation Program” which has been conducted in a pediatric hospital in France, both medical staff involved in the care of children as well as immigrant patient’s family were part of the transcultural mediation activities to decide the best management plan that fits the families cultural lived experiences and world views [45]. Similarly, a cultural mediator that was played by a case manager/case worker, facilitated care coordination of patients with limited English language proficiency across outpatient, inpatient, and community settings in United States, by ensuring a mutual understanding of medical information and the values of the patient among the clinical staff and the patients and their families [46]. Another nurse-led initiative aimed at supporting refugee and asylum seeker patients in navigating the health care system in Australia, upon presenting to the emergency department, and improving cultural competency of ED staff [47]. Furthermore, some TiC interventions targeted individuals in the patients’ social network, such as promotoras (i.e., community health workers, belonging to the community they serve) in the United States, who facilitated access to care for Latino immigrants [28] and education sector staff in Australia, who supported refugee families in navigating the healthcare system [42]. Only one intervention focused on providing training to medical staff in Australia to ensure continuity of care for patients from refugee backgrounds across different care settings [40, 41]. Most population-targeted interventions showed improvement in healthcare process outcomes, such as attending appointments and improving communication, but long-term health outcomes were rarely included in studies.
Delivery of interventionDifferent health sectors and health workforce staff were involved in the delivery of TiC interventions including physicians, nurses, pharmacists, dentists, midwives, psychotherapists, students in the health science field, community health workers and other medical staff. One intervention involved international medical graduates in the delivery of responsive and culturally appropriate primary care to refugees [26]. Some interventions engaged non-medical members to provide health-related support for RIM populations, such as language teachers [13, 37]. Communication support, engagement of lay community health workers, and training healthcare providers enhanced patient visits, but coordination is a challenging factor.
Delivery took place in various settings, such as reception centers [19, 37,38,39] refugee clinics [26, 29, 58, 60], walk-in clinics [
Comments (0)