
Remember me
Handedness was assessed using the 10-item EHI (Oldfield 1971). TMS safety screening was conducted using the 14-item TASS (Keel et al. 2001). Participants with contraindications (e.g., epilepsy, metal implants, pregnancy) were excluded.
Electromyography recordingThe electromyographic (EMG) activity of the bilateral First Dorsal Interosseous (FDI) was recorded using Kendall™ 200 series foam electrodes (Cardinal Health, Dublin, OH, USA) positioned 2 cm apart around the midpoint of the FDI muscle. A ground electrode was placed on the ulnar styloid process to reference each hand and reduce interference (Lee and Kruse 2008; Riach et al. 2018). EMG signals were recorded using BIO Amps, which applied a hardware band-pass filter from 10 to 5000 Hz and sampled at 10 kHz. This preprocessing is standard for EMG acquisition and attenuates low-frequency drift and high-frequency noise before digitisation. The signals were then transmitted to the PowerLab/4SP, which was connected to a computer with LabChart 7.
Transcranial magnetic stimulation and neuronavigationA single-pulse monophasic TMS was delivered using a Magstim 2002 stimulator connected to a figure-of-eight coil (two 70 mm loops). The coil was placed over the left motor cortex hotspot for the right FDI muscle, approximately 4 cm lateral and 1.5 cm anterior to Cz (Loporto et al. 2013), tangential to the scalp with the handle angled 45° posterior–anterior.
Neuronavigation was used to guide coil positioning using the NDI Vega ST system and InVesalius 3.1.99998 software (Souza et al. 2018). Participants wore a headband with reflective markers for motion tracking.
To identify the optimal scalp position (OSP), suprathreshold stimulations were delivered in a 1 × 1 cm grid around the motor hotspot using an estimated rMT + 5% intensity. The site producing the largest MEP was marked on InVesalius and used for formal rMT estimation using the MTAT 2.0 tool.
The resting motor threshold (rMT) was estimated using the MTAT 2.0 tool (Awiszus and Borckardt 2011) and confirmed by identifying the lowest stimulation intensity that reliably elicited ≥ 5 out of 10 MEPs ≥ 0.05 mV on the OSP. TMS pulses were delivered at 120% of rMT during the experiment, consistent with prior studies (e.g., Perera et al. 2024; Reid and Serrien 2014).
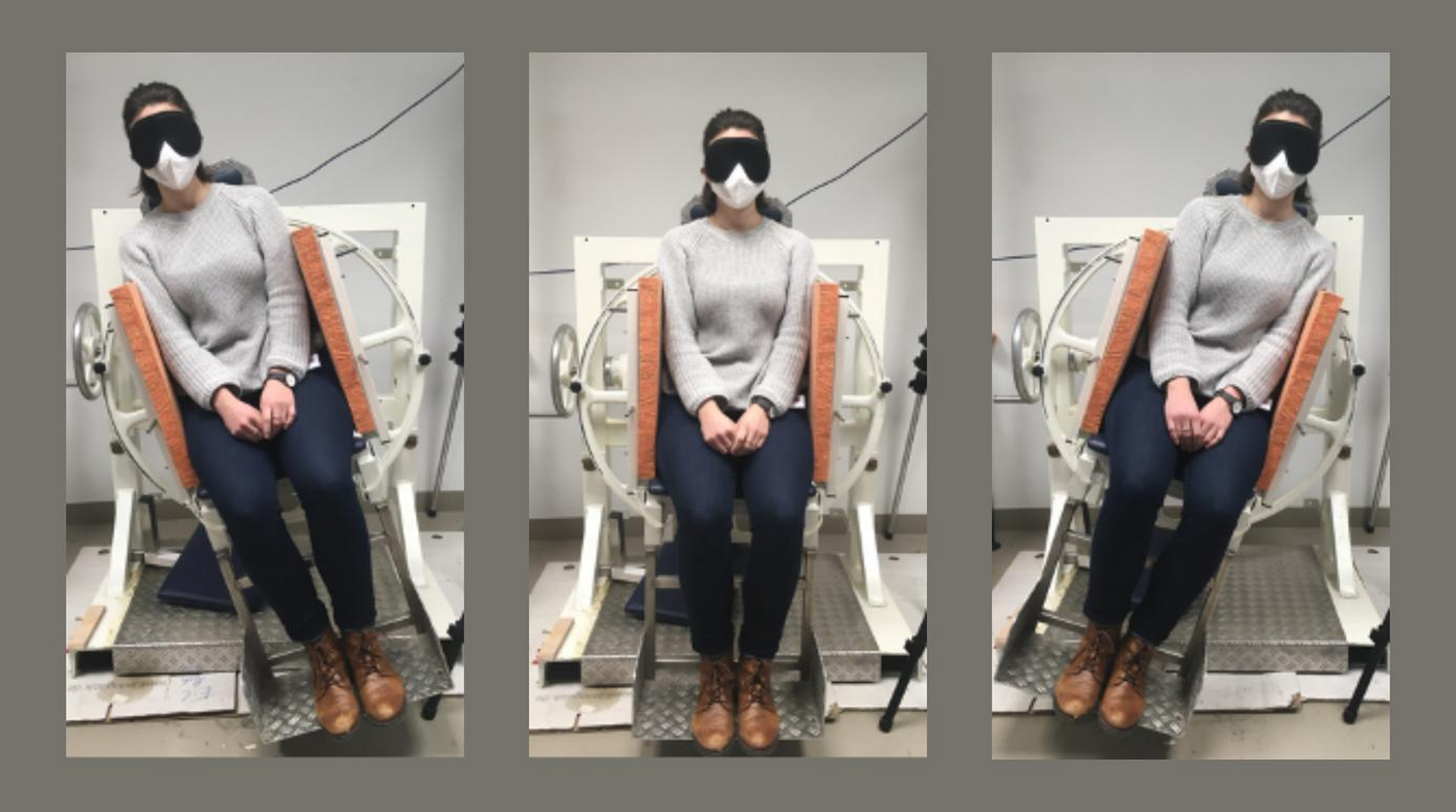
Experimental procedureParticipants completed the EHI and TASS questionnaires before scheduling. On the experiment day, participants were seated roughly 110 cm from the screen and fitted with a headband containing a rigid body for neuronavigation (Souza et al. 2018). After cleaning the skin with isopropyl alcohol wipes, three EMG electrodes were attached to each hand to record MEPs. The OSP and rMT were identified in the left hemisphere. Participants were instructed to remain still and focus on the centre of the screen throughout the session (Wright et al. 2018).
The independent variable was the TMS predictability (predictable and unpredictable). Each condition was presented using E-prime 3.0 (Psychology Software Tools, Inc. 2016) on a 24-inch LCD screen (1920 × 1080, 60 Hz). Figure 1 shows the experimental procedure used to present the experimental conditions.
Fig. 1
Experimental procedure for predictable (moving bar) and unpredictable (static bar) TMS. The static white bar lasts for 5 to 7 s before the program pseudo-randomly chooses between a predictable moving bar or an unpredictable static bar condition, each lasting 3.5 s
Each trial began with a static white bar displayed for a random interval (5–7 s). The program then randomly selected a predictable or unpredictable condition. In the predictable condition, the bar emptied and refilled gradually over 3.5 s, with a TMS pulse delivered at full. In the unpredictable condition, the static bar remained unchanged for 3.5 s before TMS delivery, preventing temporal prediction.
Each condition was presented 20 times using identical visual stimuli devoid of human/animal content to isolate predictability (Fu and Franz 2014; Rizzolatti and Craighero 2005).
Data analysisEMG data were recorded using LabChart 7 (ADInstruments 2023) at a 10 kHz sampling rate, band-pass filtered online (10–5000 Hz), and continuously monitored throughout the experiment to detect spontaneous muscle activity. Trials were segmented offline into 9-second windows (–3.5 to + 5.5 s) and down-sampled to 2 kHz for analysis.
Analysis was conducted using R (v4.4.1; R Core Team 2021). All 20 participants completed the study. No dropout occurred, but 21 trials (2.63%) were excluded due to excessive pre-stimulus EMG noise (± 2.5 SD filter; Loporto et al. 2012; Riach et al. 2018; Wright et al. 2018).
Pre-TMS EMG was assessed in two windows: − 3000 to − 1500 ms (baseline tone) and − 1500 to − 5 ms (anticipatory tension). EMG was quantified as the voltage range (maximum – minimum) per window, and mean values were calculated for each participant per condition. Normality and variance assumptions were assessed using the Shapiro-Wilk and Levene’s tests, and group comparisons were conducted using either a two-sample t-test or Wilcoxon rank-sum test, depending on assumption outcomes.
Peak-to-peak MEP amplitudes were calculated from the high-pass filtered signal (20 Hz, zero-phase Butterworth) on a single-trial basis, then averaged by condition (predictable, unpredictable) for each participant. The primary outcome measure was the raw MEP amplitude from the contralateral FDI muscle. Z-scored MEP amplitudes were also computed to assess the robustness of the effect (Meers et al. 2020; Riach et al. 2018; Vallence et al. 2023). Normality was confirmed with Shapiro-Wilk tests, and paired t-tests were applied to both raw and z-scored data.
Waveforms were grand-averaged and time-locked to the TMS pulse (0 ms) to visualise response timing. These are presented for illustrative purposes only and were not used for statistical analysis.
Finally, linear regression analysis examined the influence of predictability, stimulation intensity, age, gender, and handedness on MEP amplitudes. Residual diagnostics were performed to check for outliers and violations of regression model assumptions. Detailed scripts and steps are provided in Supplementary Material 1.
Comments (0)