This study provides a comprehensive analysis of the global burden of endometriosis from 1990 to 2021 using data from GBD. Our study indicated that during the period of 1990–2021, the global ASIR, ASPR, and age-standardized YLDs rate for endometriosis showed a widely decreasing trend, but EAPC varied across different SDI regions and GBD regions. The burden of surgically confirmed endometriosis is mainly concentrated in women aged 20–30 years, and declines with increasing SDI levels. The result of decomposition analysis reveals the global numbers of incidence, prevalence, and YLDs of endometriosis significantly increased over the past 30 years, and these upwards are primarily driven by population growth. Conversely, epidemiological changes, reflecting reductions in incidence, prevalence, and YLDs, mitigated these increases.
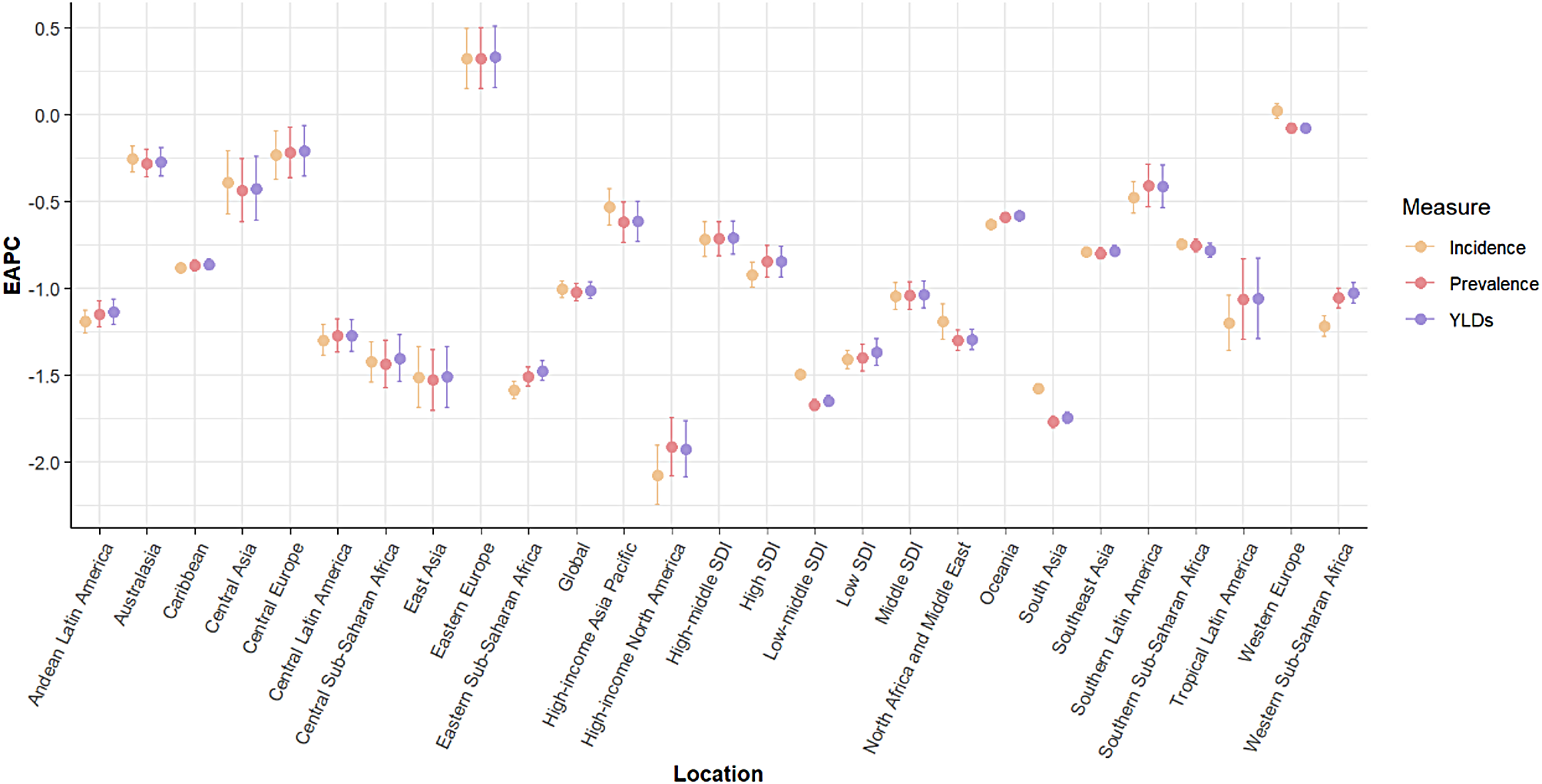
The joinpoint regression analysis shows that from 1990 to 2021, the burden of endometriosis has decreased year by year in most SDI regions. However, high-middle and middle SDI regions experienced fluctuating trends: declines from 1990 to 2010 and 2015 to 2021, but an increase from 2010 to 2015. This fluctuation may be due to changes in medical therapeutic patterns or therapy guidelines. For example, a German study indicated that the proportion of endometriosis patients treated with dienogest significantly increased between 2010 and 2019, and during the same period, the prevalence of endometriosis also significantly increased [18].
The analysis of the burden of surgically confirmed endometriosis by age groups in 2021 reveals critical insights into the demographic distribution of the disease. The global age-specific incidence rate and the number of incident cases peaked in the 20–24 age group. The global prevalence rate and the number of prevalent cases, as well as the YLDs rate and the number of YLDs, peaked in the 25–29 age group in most SDI regions. The peak burden in women aged 20–30 highlights its impact on quality of life and reproductive health. Thus, this period is a critical time for intervention. We should focus on the the prevention and comprehensive management of the 20–30 age group, and improve the ability of early diagnosis and treatment. However, in the high SDI region, the highest prevalence and YLDs rates were concentrated in the 40–44 age group. Previous studies have shown that cesarean section and induced abortion are important risk factors that cannot be ignored for developing endometriosis [19, 20]. The average childbearing age in developed countries is higher than in less developed countries, and the prevalence of cesarean and abortion procedures is very high. This may be an important reason why the age of onset in high SDI regions is later than in other regions.
By analyzing the relationship between SDI levels and endometriosis burden, we found that the average expected values of the burden of endometriosis decreased with increasing SDI levels. This contrasts with some previous studies [21, 22], but also shows the same trend as the conclusions of others [23, 24]. In fact, the true incidence of endometriosis is difficult to determine, because the gold standard for the diagnosis of endometriosis is the combination of laparoscopy visualization and histologic confirmation of the presence of endometrial glands and/or stroma [25, 26]. However, laparoscopy is an invasive procedure, and clinicians in some regions typically prefer other non-invasive techniques, such as ultrasound and magnetic resonance imaging (MRI), to identify endometriosis, but their accuracy is limited [27]. Furthermore, the nonspecific nature of endometriosis symptoms and the tendency to normalise them may contribute to the delay in diagnosis. For example, non-specific symptoms such as dysmenorrhea have often been treated with hormonal drugs without consideration of endometriosis [28]. Thus, clinicians’ skills, awareness of endometriosis, and economic and geographic access to care will all affect diagnostic outcomes [29, 30]. In high-level SDI regions, the increased medical management of endometriosis reduce the need for surgical treatment, thereby decreasing the incidence of surgically confirmed diagnoses. Moreover, the operative treatment and diagnostic procedures concerning fibroids in particular, and also female sterilization and infertility, have decreased during the years, decreasing the possibility to diagnose endometriosis as an incidental finding. These changing treatment trends may reduce the incidence of surgically validated endometriosis [23]. Additionally, oral contraceptives have been proven to significantly reduce menstrual flow and may prevent the occurrence of endometriosis by interfering with the implantation of retrograde endometrial cells [31, 32]. The use of the pill is more widespread in developed regions, which reduces the incidence of endometriosis to some extent [33,34,35]. Meanwhile, multiple studies have shown that environmental toxicants such as dioxins, phthalates, bisphenol A, or organochlorinated pollutants play a significant role in the development of endometriosis [36,37,38]. Compared to high-level SDI regions, low-level SDI regions generally have poorer environmental governance. Activities such as waste incineration or metal smelting release large amounts of dioxins, increasing the likelihood of exposure to harmful chemicals. These warn us that regions with lower SDI may face more severe challenges. Addressing these disparities requires multifaceted approaches, including promoting access to healthcare, enhancing health education, improving living environments, and implementing targeted public health strategies.
Furthermore, we employed decomposition analysis to disentangle the contributions of population aging, population growth, and epidemiological changes to the disease burden. High SDI and High-middle SDI regions experienced declines in numbers of incidence, prevalence, and YLDs, primarily driven by favorable epidemiological changes. This indicates that disease prevention and health promotion can effectively mitigate the challenges posed by demographic changes (population growth and population aging) to endometriosis. Low SDI and Low-middle SDI regions saw increases in incident cases, prevalent cases, and YLDs cases, with population growth being the dominant factor. Statistically, the 47 least developed countries are among the fastest growing countries in the world, and many of them are expected to double their populations from 2019 to 2050 [34]. Overall, in the coming decades, population growth will have a greater impact on some low SDI and lower-middle SDI regions, leading to a continued increase in the burden of endometriosis, while the impact on high-level SDI regions will stabilize. Therefore, when formulating or adjusting health prevention measures, international organizations or national governments should consider the potential impact of population growth on health in different regions.
To the best of our knowledge, this study is the first to comprehensively analyze the global burden of surgically confirmed endometriosis from 1990 to 2021, using robust statistical methods to assess trends and correlations. With each iteration of the GBD, the disease classification methods have become more standardized, and more in-depth systematic evaluation methods have been used to obtain country-specific information, providing reliable data sources for this study. Methodological advancements have enabled GBD 2021 to produce estimates more easily than in previous iterations; however, as with any study of this scope, there are several important limitations to acknowledge. First of all, inconsistencies in the availability of primary epidemiological data remain a limitation and source of instability within GBD analyses. The estimates of disease burden depend on the out-of-sample predictive validity of modelling processes in cases where data are insufficient to produce burden estimates for all 204 countries and territories (by year, sex, and age). Although this approach cannot fully replace high quality primary data, it ensures that populations or causes with no or little data are not excluded from important benchmarking exercises intended for burden estimation. In addition, with any given GBD release, there might be extant data not identified or incorporated, which is a key part of the rationale for ongoing cycles of releases, rather than a single update. For the primary data available, the data processing methods account for known sources of variation wherever possible, but fully disentangling variation in estimates is not always possible due to measurement error and reporting inaccuracies. There are problems with the quality and collection of primary data, such as flawed methodologies and potential under-reporting of illnesses, which is a recurring limitation for GBD that can be continually improved on by strengthening data-collection systems [39]. This study also has some limitations. First, sparsity of data or unreliability of data from specific regions, time periods, or age groups can influence the accuracy of the endometriosis burden estimates, particularly poor data quality and coverage from western, eastern, southern, and central sub-Saharan Africa and south Asia [40]. Second, the disease burden may be underestimated in some low- and middle-income regions due to limited data or lack of gold-standard diagnostics like laparoscopy. Third, as our study spans three decades, changes in the diagnostic criteria for the disease may impact the temporal trend analysis. Finally, in the decomposition analysis, the selection of driving factors may not be comprehensive enough, attributing only to population aging, population growth, and epidemiological changes. Due to the lack of relevant data, other influencing factors such as environment, diet, lifestyle, or genetic susceptibility were not included temporarily, future research may focus on this issue.





Comments (0)