In this retrospective cohort study, we evaluated the clinical efficacy of emergency OC and identified factors associated with reproductive outcomes by analyzing six consecutive years of clinical data from our center. The overall CLBR per cryopreservation-thaw cycle was 29.2%. Specifically, among cycles performed for absolute male factor infertility, the CLBR was higher, at 39.5%. However, prolonged infertility duration and the necessity for surgical sperm retrieval from the male partner were significant predictors associated with poorer reproductive outcomes. In contrast, cycles performed for relative male-factor infertility exhibited a substantially lower CLBR of 11.8%. In these cases, advanced maternal age at the time of oocyte retrieval, fewer mature oocytes retrieved, and a previous diagnosis of azoospermia or oligoasthenoteratozoospermia in the male partner emerged as significant negative prognostic factors.
The study found that 62.8% of emergency OC cycles encountered sperm absence due to the male partner’s inability to produce sperm via masturbation or TESA/micro-TESE on the day of oocyte retrieval, mainly because of severe oligoasthenoteratozoospermia or non-obstructive azoospermia. The remaining 37.2% of patients experienced unexpected incidents that prevented timely sperm collection. Compared to a study conducted between March 2009 and October 2017 (unexpected partner absence, 11.0%; unavailable sperm from ejaculate or surgical extraction, 89.0%) [21], the incidence of partner absence increased, likely due to COVID-19 public health restrictions that impeded clinic visits.
Among couples diagnosed with absolute male factor infertility—who constituted the majority of oocyte cryopreservation cases in our cohort—there was a consistent and marked preference for achieving fertilization using the male partner’s own sperm. In instances of failed sperm retrieval, oocyte vitrification served as an interim strategy that prevented the loss of mature oocytes while preserving the opportunity for future use of autologous sperm. Compared with immediate fertilization using donor sperm, this approach was more congruent with the couples’ expressed desire for a genetically related child. One illustrative case involved the only couple in the cohort who underwent two successive cycles of oocyte vitrification and warming. The male partner had been diagnosed with azoospermia on the basis of routine semen analysis and expressed strong opposition to the use of donor sperm. On the day of the initial oocyte retrieval, he underwent TESA, which failed to yield spermatozoa; the retrieved oocytes were thus vitrified. Following warming of this cohort, a second TESA procedure was performed, during which sperm were successfully retrieved and used for ICSI. Despite this, no viable embryos were obtained. A third TESA was attempted on the day of the second oocyte retrieval, which also proved unsuccessful, necessitating another cycle of oocyte vitrification. Following warming of the second cohort of oocytes, fertilization was performed using donor sperm, in accordance with the couple’s updated treatment decision.
Cases of OC attributed to sperm retrieval failure were predominantly observed in younger women presenting with primary infertility, characterized by lower prevalence of diminished ovarian reserve and tubal infertility factors, thus underscoring severe male-factor infertility as the principal indication for OC. Consistent with this, donor sperm was utilized for fertilization in 81.3% of these cycles. Conversely, cycles initiated due to unexpected absence of the male partner were more frequently encountered among women of advanced reproductive age and were associated with higher incidences of female infertility factors, as well as a reduced number of mature oocytes retrieved. Collectively, these demographic and clinical characteristics elucidate important differences between patient groups, providing critical context for understanding subsequent clinical outcomes and identifying prognostic determinants of OC cycles.
The study included both fresh and frozen ET cycles following OC, providing a comprehensive evaluation of embryological and reproductive outcomes in emergency oocyte vitrification. Assessed outcomes included survival rate, fertilization rate, biochemical pregnancy rate, implantation rate, clinical pregnancy rate, miscarriage rate, and CLBR. For the calculation of biochemical pregnancy rate, implantation rate, clinical pregnancy rate, and miscarriage rate, the outcomes of fresh and frozen embryo ETs were combined, as no significant differences were observed between fresh embryo transfer cycles and frozen embryo transfer cycles. Recent large-scale studies on autologous vitrified oocytes have reported survival rates ranging from 80 to 90% [23, 25,26,27, 37, 38], consistent with our study’s survival rate of 84.2%. Although the median fertilization rate (57.7%), clinical pregnancy rate per transfer cycle (36.2%), and CLBR (29.2%) observed in our study are relatively lower than the outcomes reported in these previous studies, this discrepancy is justifiable, as those studies mainly involved oocyte vitrification for women aiming to avoid the gonadotoxic effects of cancer treatment or age-related fertility decline, rather than dealing with infertility problems in either partner. On the other hand, our final outcomes align closely with previous studies on emergency oocyte vitrification, such as those by Fu et al. and Zhan et al., who reported CLBR of 32.5% and 34.1%, respectively [22, 39]. Differences in CLBRs reported in other studies on emergency oocyte vitrification may be due to smaller sample sizes [19, 20] or the use of slow freezing techniques instead of vitrification [18].
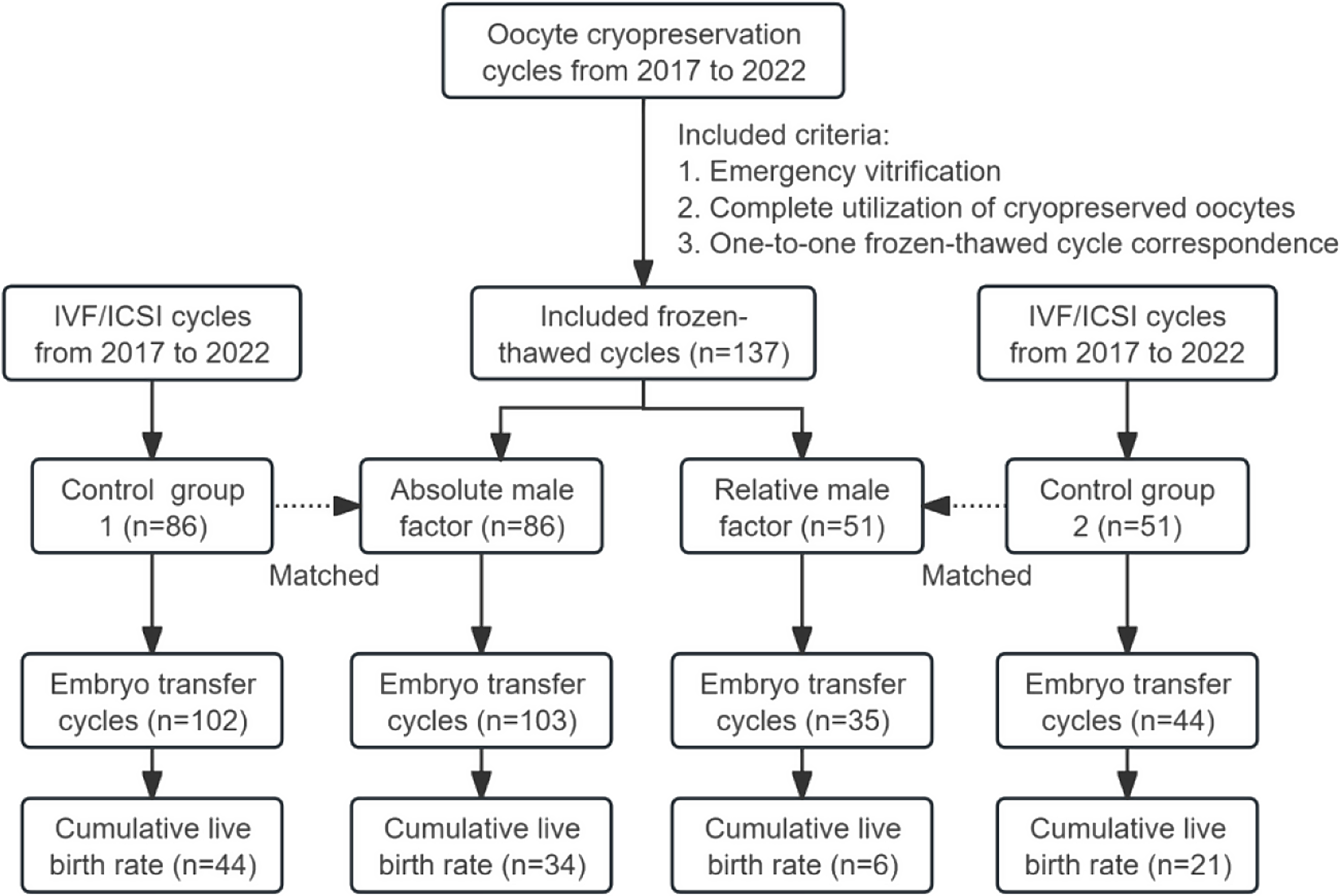
To evaluate the clinical utility of emergency OC, we compared outcomes from vitrification cycles to those from a control cohort undergoing ICSI with fresh oocytes. Due to significant baseline differences between patients categorized as having absolute versus relative male factor infertility, separate control groups were matched for each subgroup to ensure appropriate comparisons. In the relative male factor group, CLBR was significantly lower in the cryopreservation cohort compared to controls. This disparity may be explained by the only significant baseline difference identified between the groups: the number of mature oocytes retrieved. A recent study by Zhan et al. supports this interpretation, reporting that patients undergoing cryopreservation following sperm retrieval failure due to acute, non-permanent events (e.g., stress-induced temporary anejaculation) had fewer oocytes retrieved and lower CLBR compared to those using fresh oocytes [39]. These findings suggest that individuals who opt for emergency OC in the context of relative male factor infertility may have diminished ovarian reserve, leading to fewer mature oocytes and, consequently, reduced reproductive potential. In this context, the poorer outcomes observed in the cryopreservation group may reflect underlying patient characteristics rather than the effect of vitrification itself. In the absolute male factor cohort, no significant difference in CLBR was observed between the vitrified and fresh oocyte groups, suggesting that the delay introduced by emergency OC did not adversely affect reproductive outcomes. Taken together, these findings suggest that emergency oocyte vitrification constitutes a clinically acceptable fallback strategy in situations where sperm is unavailable from the male partner on the day of oocyte retrieval.
Although reproductive outcomes did not differ significantly between patients with absolute male factor infertility and a matched control group—adjusted for female age, infertility diagnosis in either partner, and final sperm source—the majority of patients in the absolute male factor cohort ultimately required the use of donor sperm. Given these findings, the routine use of emergency OC in this population warrants reconsideration, particularly in the absence of demonstrable improvements in cumulative live birth rates. These results underscore the importance of incorporating donor sperm as a planned contingency within OC strategies. Accordingly, the decision to pursue OC should be guided by individualized counseling that takes into account the couple’s reproductive goals, prognosis, and logistical considerations.
Patients undergoing emergency OC have high expectations for treatment outcomes and are particularly concerned with the efficacy and influencing factors of their cycles. Hagege et al., in a discussion on fertility preservation consultation, emphasized the importance of identifying the optimal age and the ideal number of oocytes in OC cycles [12]. In the absolute male factor cohort, a longer duration of infertility emerged as a negative prognostic factor, consistent with prior literature [40,41,42]. Furthermore, cycles utilizing surgically retrieved sperm were associated with inferior clinical outcomes compared to those using ejaculated sperm. However, given the small number of cases in each subgroup (9.3%, 8/86), these findings should be interpreted with caution and warrant further validation in larger, adequately powered studies. In the relative male factor cohort, both maternal age at oocyte retrieval and the number of mature oocytes retrieved—two well-established predictors of assisted reproductive outcomes [22, 23, 26, 27, 29, 37, 38, 43,44,45,46]—were significantly associated with CLBR. Compared with the absolute male factor group, women in this cohort were significantly older and had a lower mature oocyte yield. Notably, while these female-related factors significantly influenced CLBR in the relative male factor group, they did not exert a measurable effect in the absolute male factor group. These findings suggest that, in the relative male factor group, progressive maternal aging and further declines in oocyte yield—superimposed on an already advanced reproductive age and diminished ovarian response—may contribute significantly to the observed reduction in CLBR. Also, we found that the duration of OC did not significantly affect the CLBR of either group, which is consistent with several studies [22, 23, 47, 48].
Our study has several strengths: First, the study includes both fresh and frozen embryo transfer cycles, allowing for the evaluation of CLBR—a clinically meaningful endpoint in assisted reproductive technology—and enabling more precise and individualized patient counseling. Second, to our knowledge, this is among the first studies on emergency oocyte vitrification to systematically investigate the factors associated with CLBR across distinct clinical indications for vitrification, through comprehensive subgroup analyses. Third, the analysis includes all consecutive cases of emergency oocyte vitrification and subsequent warming cycles conducted between 2017 and 2022 at one of the largest ART centers in China, using data extracted from electronic medical records to ensure accuracy and reduce recall bias.
The study has several limitations: (1) The findings are derived from a single-center cohort, which may limit their generalizability to other populations. (2) The sample size is relatively small, necessitating further studies with larger cohorts to validate these conclusions. (3) This is a retrospective study, and conducting randomized controlled trials (RCTs) on emergency oocyte vitrification poses significant challenges. As a result, there may be a paucity of high-level evidence in this area.





Comments (0)