
Remember me
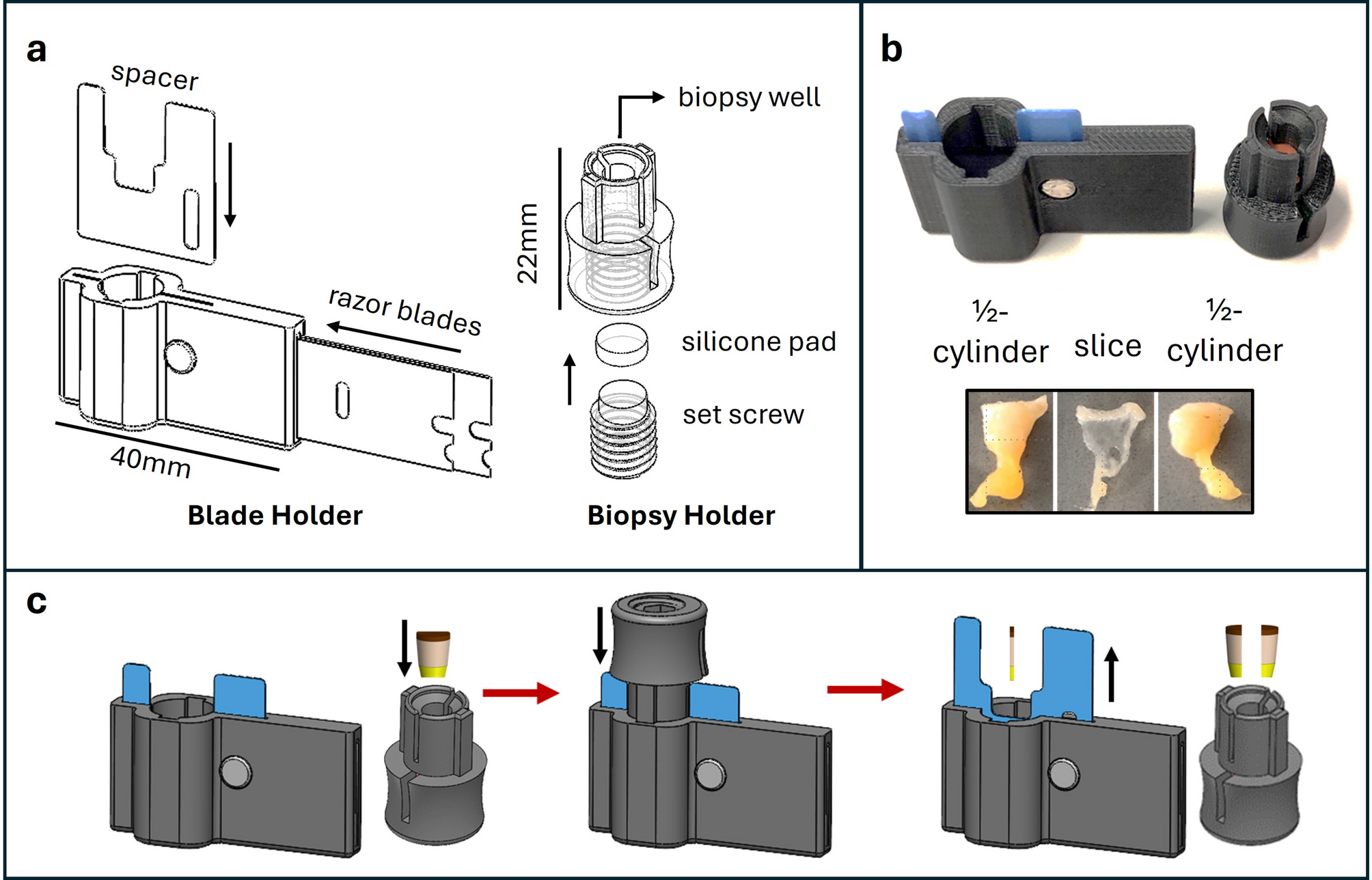
Slicer prototypes were evaluated on whether they completely partitioned skin punch biopsies and the thickness of the cross-sectional tissue slice. In an initial screening, two types of razor blades were assessed with several spacer thickness on thawed, once-frozen punch biopsies from porcine (n = 3) and human (n = 2) tissue. With porcine biopsies, each of the Slicer prototypes demonstrated initial success in producing tissue slices, and increasing spacer thickness generally yielded thicker tissue slices (Fig. 2a). However, with the considerably more elastic human tissue, smaller spacer sizes resulted in larger variations between the two trials (Fig. 2b). Instances where thin spacers produced incomplete cross-sectional slices or even no retrievable tissue prompted the selection of two prototypes with thicker spacers for further testing with eight additional human skin biopsies (Fig. 2c-d). As two of the slices produced by the 0.08 mm blades yielded little to no dermal tissue, the final Slicer prototype design consisted of two 0.23 mm razor blades. The 3D printed spacers were replaced with aluminum parts in the nearest available thickness: 0.40 mm.
Fig. 2
Slicer development on thawed, once-frozen porcine and human skin punch biopsies. Prototypes with varying spacer thickness and razor blade were used on porcine (a) and human (b) skin punch biopsies (n = 3 and 2, respectively). After screening, two versions (shaded bars in b) were selected for further testing with eight additional human biopsies. The slices were evaluated quantitatively (C) and qualitatively (D). Slice thickness was estimated from Eq. 1. Data shown is mean and absolute range for a-b and mean and SD for c
Further testing was performed to assess the consistency of Slicer using larger sets of thawed, once-frozen porcine and human skin punch biopsies (Table 1). For porcine skin biopsies, the mean slice thickness was calculated as 0.57 mm (n = 60, SD = 0.04 mm). For human skin punch biopsies, the mean slice thickness was 0.29 mm (n = 22, SD = 0.05 mm). As each Slicer attempt was successful – defined by the complete partitioning the biopsy and the collection of a slice – Slicer prototypes were next used to partition patient biopsy samples.
Table 1 Slicer testing on thawed, once-frozen porcine (n = 60) and human (n = 22) 5 mm diameter skin punch biopsiesApplication of slicer to patient samplesSlicer prototypes with the 0.23 mm razor blades and 0.40 mm spacers were provided to biopsy service practitioners in Uganda for use on patient skin punch biopsies at the time of collection. The biopsy service practitioners were first trained to use Slicer via a simple two-minute video demonstration and hands-on practice using 5 mm cylindrical pieces of beef. Slicer prototypes were then used to partition the 5 mm diameter skin punch biopsies collected from consecutive participants enrolled in Uganda because of clinical suspicion of KS (Supplemental Fig S3). For 26 biopsies – originating from patient arms (n = 10), legs (n = 12), and one each from the head, abdomen, hand, and genital region – the total biopsy mass and slice mass were recorded to estimate the thickness of each slice (Table 2). The slices, which ranged from 4 mg to 16 mg, averaged approximately 0.46 mm in thickness (SD = 0.10).
Table 2 Slicer testing on fresh biopsies collected from 26 patients with clinical suspicion of KS who presented to a skin biopsy service at the infectious diseases institute in Kampala, UgandaTo provide feedback on the acceptability of Slicer from the user’s perspective, biopsy service practitioners in Uganda completed a survey for the first 25 biopsies. The questions assessed the ease of using Slicer in comparison to manual bisection using either a blade or a scalpel (Supplemental Figure S1). The survey results confirmed that Slicer was simple to use and easier than manual methods (Table 3). Following this positive feedback from the biopsy service practitioners, additional Slicer prototypes were provided for subsequent testing in conjunction with the ColdSHOT extraction.
Table 3 Responses on a 5-point scale from biopsy service practitioners in Uganda when asked to compare using slicer to manual methods for the various stages of biopsy partitioning for the first 25 attempts using slicerColdSHOT optimization for tissue slicesTo maximize ColdSHOT DNA yields from tissue slices, brief optimizations for sodium hydroxide concentration, extraction volume, and incubation time were performed following the application of Slicer to thawed, once-frozen porcine biopsies (Fig. 3). The tissue slices were immersed in 150 µl of 25, 50, or 100 mM NaOH solutions (n = 4 per group). After a one-hour incubation, neutralizing buffer was added proportionally to the NaOH concentration, yielding final volumes of 300, 450, and 750 µl, respectively. To compare concentrations across consistent volumes, the 25 mM and 50 mM solutions were repeated with increased volumes (n = 4 per group). As measured by targeting the porcine GAPDH sequence via LAMP, increased alkaline concentrations resulted in higher DNA concentrations (Fig. 4a). Overall, 150 µl of a 100 mM NaOH solution followed by 600 µl of the neutralizing solution produced the highest DNA yields with a mean of ~ 65,000 copies of GAPDH per 5 µl reaction (logscale: mean = 4.82, SD = 0.11). To determine whether a different incubation time might increase DNA yields, the experiments were repeated using 150 µl of 100 mM NaOH and 600 µl of buffer with varied incubation times (Fig. 4b). The ambient incubation durations included 10, 30, and 60 min as well as 24 h (n = 4 per group). Each timepoint yielded ≥ 30,000 copies of DNA with the one-hour incubation resulting in a maximum yield of ~ 64,000 copies per reaction (logscale: mean = 4.81, SD = 0.07). To maximize the DNA yields, and thereby the sensitivity for KSHV testing, a one-hour incubation was selected for patient sample testing. These ColdSHOT yields were similar to the yields recovered by DNeasy from porcine slices (logscale: mean = 4.76, SD = 0.45, n = 3).
Fig. 3
ColdSHOT optimization on thawed, once-frozen porcine tissue slices. DNA yields, quantitated by a LAMP assay targeting GAPDH, were compared across varying NaOH concentrations and final extraction volumes for a one-hour incubation (a). DNA yields were measured as a function of time using 100 mM NaOH and a final volume of 750 µl (b). Data shown is mean and absolute range
Fig. 4
LAMP data comparing the ColdSHOT and DNeasy yields for KSHV detection in patient samples. KSHV DNA content was quantitated via LAMP using DNA extracted by ColdSHOT (thin slice) and by DNeasy (¼-cylinder). Mean copy number and absolute range are shown with US-based histopathological diagnoses indicated below (a). DNA yields for GAPDH (all samples) and KSHV (KS-present samples only) were compared between the DNeasy (¼-cylinder) and ColdSHOT (thin slice). Mean copy number and standard deviation are shown (b). Bland-Altman analyses were used to compare DNeasy to ColdSHOT for the GAPDH (c) and KSHV (d) assays with 95% limits of agreement indicated
Application of Slicer and ColdSHOT to patient samples: nucleic acid testingSlicer prototypes were used in conjunction with ColdSHOT and real-time LAMP and qPCR assays to quantitate DNA extracted from a subsequent set of 27 consecutively collected patient biopsies. DNA was extracted from the tissue slices using ColdSHOT and from corresponding ¼-cylinder portions using the DNeasy Blood and Tissue Kit. The results of the nucleic acid tests were compared to histopathological diagnoses.
Real-time LAMP testingFor LAMP-enabled KS diagnostics, Slicer and ColdSHOT were evaluated as a rapid sample processing alternative to traditional methods such as DNeasy. For both the ColdSHOT and DNeasy extracts, the LAMP assay detected KSHV DNA in each biopsy interpreted as KS-present by conventional histopathologic interpretation, and no KSHV DNA was detected in biopsies interpreted as KS-absent (Fig. 4a). To compare the ColdSHOT to DNeasy, quantitative analyses included the GAPDH yields for each sample as well as the KSHV yields for the KS-present samples (Fig. 4b). For GAPDH, DNeasy recovered ~ 26,000 copies per reaction (logscale: mean = 4.43, SD = 0.3) versus ColdSHOT’s ~ 6,000 copies per reaction (logscale: mean = 3.79, SD = 0.25). For KSHV, yields averaged ~ 2,400 copies for DNeasy (logscale: mean = 3.37, SD = 0.44) and ~ 800 copies for ColdSHOT (logscale: mean = 2.90, SD = 0.52). A Bland-Altman analysis of the log-scale GAPDH yields revealed DNeasy yields were a mean 0.64 log-10 copies greater than ColdSHOT yields (95% limits of agreement ranging from 0.01 to 1.26) (Fig. 4c). A similar Bland-Altman analysis of the log-scale KSHV yields revealed DNeasy yields were a mean 0.38 log-10 copies greater than ColdSHOT yields (95% limits of agreement ranging from − 0.91 to 1.67) (Fig. 4d).
qPCR testingThe objective of qPCR testing was to evaluate the compatibility of the ColdSHOT extraction with qPCR. Similarly to LAMP, qPCR detected KSHV DNA in each KS-present sample as determined by histopathology (Fig. 5a). However, one KS-present sample exhibited low copy numbers, and two KS-absent samples had one replicate each with detectable KSVH DNA, highlighting the need for quantitative assays for KS diagnostics. To compare the quantitative assays, PCR versus LAMP, Bland-Altman analyses were performed for the yields of GAPDH (Fig. 5b) and KSHV (Fig. 5c). For GAPDH, the PCR yields were a mean 0.30 log-10 copies greater (95% limits of agreement: -0.67 to 1.27) while for KSHV, the PCR yields were a mean 0.21 log-10 copies greater (95% limits of agreement: -1.34 to 1.75).
Fig. 5
PCR data for the ColdSHOT yields from thin tissue slices collected from patient samples. Copies of GAPDH and KSHV were quantitated per 5 µl reaction. Mean copy number and absolute range are shown with US-based histopathological diagnoses indicated below (a). Bland-Altman analyses were used to compare GAPDH (b) and KSHV (c) quantitation via PCR and LAMP for the ColdSHOT extraction with 95% limits of agreement indicated
Comments (0)