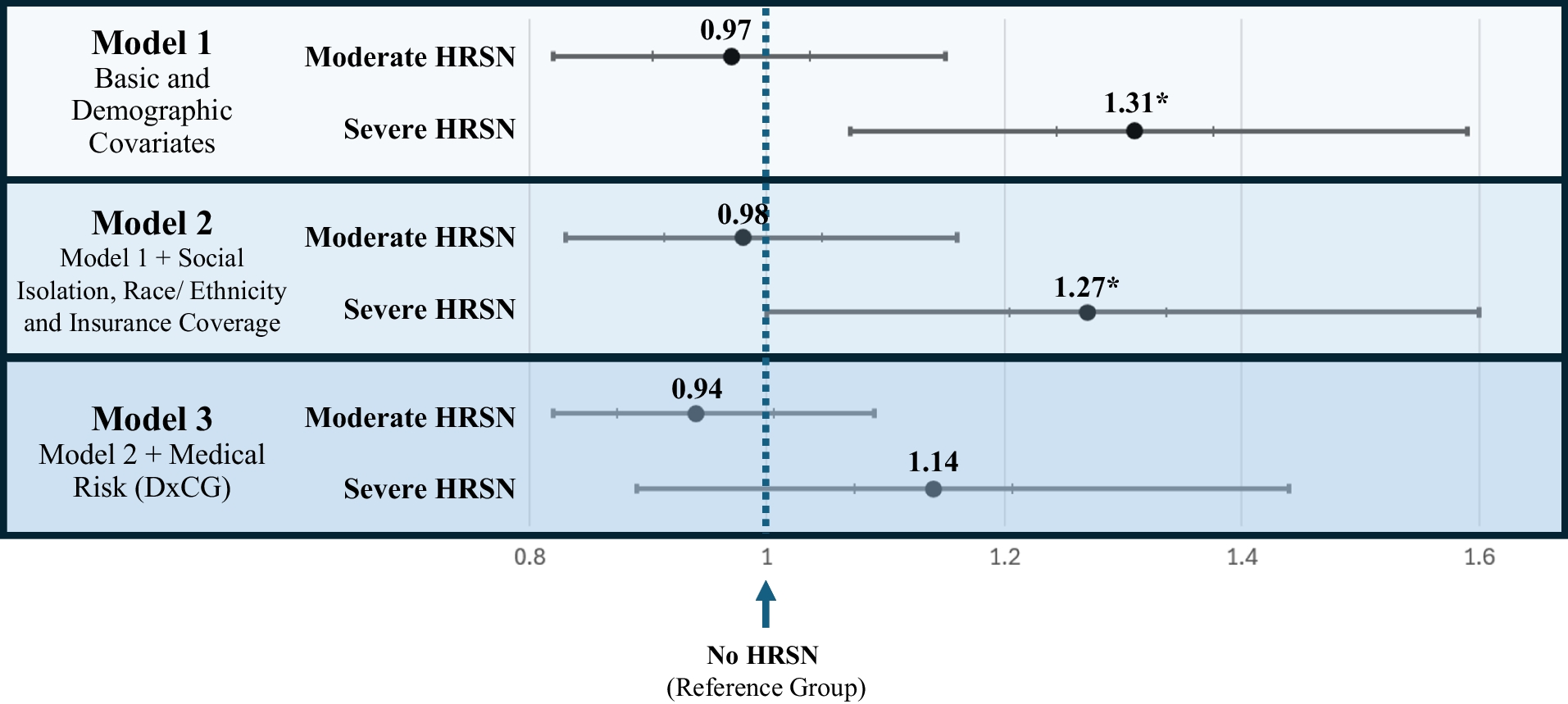
This cross-sectional study of over ten thousand Kaiser Permanente members examined associations between HRSN and total healthcare cost, as well as how these associations change when considering factors such as insurance coverage and medical risk. The results showed a strong and significant positive relationship between “Severe HRSN” and total healthcare cost. When including medical risk, this association was attenuated. Distinctively, this study explores this association using a broad, patient-reported measure of HRSN in a population that approximates the general US population in terms of demographic characteristics23. The data are drawn from an integrated healthcare system, which allows for a more confident measurement of total healthcare cost than may be possible in more fragmented settings. These findings provide a unique addition to the existing body of literature, which largely focuses on specific subpopulations or interventions, and may inform how organizations approach HRSN screening and intervention.
In our analysis, moderate need did not show statistically significant associations with cost, relative to those with no need. However, it is important to note that our cross-sectional study does not follow the progression of patients’ needs over time. Individuals may have moderate needs that ultimately progress in severity, and there may be benefit to early intervention for moderate HRSN. Further, potentially reduced costs represent only one pragmatic motivation for assisting patients with HRSN and do not consider broader health and societal benefits or ethical obligations that healthcare organizations may have to assist patients with HRSN28,33.
Our study illustrates the challenges of studying the complex relationships between medical risk, social risk, and healthcare cost. Our findings of a large magnitude of association between “Severe HRSN” and cost in models controlling for demographic covariates and insurance status are in line with previous findings establishing associations between HRSN and utilization5,6. The attenuation of those results when we introduce a strong control variable for medical risk deserves further investigation, as social risk and medical risk have complex relationships that are often causal and bi-directional in nature. It may be possible that HRSN, even when severe, do not lead to differences in healthcare costs above and beyond the patients’ underlying medical conditions. However, alternative explanations may also be at play. As a risk adjustment scheme, the DxCG essentially uses assigned patient diagnoses and data on prescription drug codes to predict healthcare costs. While some recently developed risk adjustment schemes attempt to incorporate HRSN, the version of DxCG available for this analysis does not directly or separately control for HRSN. Thus, if patients with a given diagnosis also have high levels of HRSN, the DxCG will capture that social risk effect within its index. Consequently, adjusting for DxCG may lead to “over-controlling,” wherein aspects of the independent variable of interest (HRSN) are included in a control variable (DxCG), and true underlying associations between the independent variable and the outcome of interest can be masked. Future studies may be able to provide further clarity on the relationships between medical risk, social risk, and cost. In particular, following patients’ medical and social risks longitudinally may leverage differential changes in each phenomenon over time to better understand independent effects on cost.
Our study may provide insight into challenges of funding efforts to address HRSN interventions. A recent simulation study estimated the costs of screening for and intervening on HRSN in primary care and concluded that costs would likely be higher than what is feasible under current funding mechanisms available to providers29. External incentives, collaborations, and financial support may be required if policymakers wish to support further investigation and development of interventions that might have longer-term or non-financial benefits. For example, novel demonstration projects such as Robert Wood Johnson Foundation’s “Bridging the Gap: Reducing Disparities in Diabetes Care” program have shown promising results on how new payment models and deep community partnership can be used to support cross-sectoral, multi-level, and tailored interventions to address patient HRSNs30,31. Leveraging these types of partnerships may provide opportunities to address patient HRSNs even in circumstances where the current demonstrable health system return on investment is unclear.
Our findings also highlight the importance of evaluations that are designed up-front to address the potential overlapping measurements of medical and social risks. While our demographic and insurance type models may overestimate potential cost savings by not accounting for differences in disease diagnosis between HRSN groups, our DxCG model—and its potential for over-controlling for social risk—illustrates the need for caution when constructing models where adjustment variables may capture aspects of the independent variable of interest. Given the large potential cost implications of addressing HRSN, it will be essential for health systems to gain greater clarity on this issue through further research.
This study has several additional limitations of note. First, it is unable to make any strong causal inferences, nor does it address whether interventions lead to cost reductions. Instead, our work serves as an indicator of a potential magnitude for cost savings opportunity that may be an important point of information for those considering HRSN interventions. Second, the relationships among the social construct of race, insurance, social need, and healthcare costs are complex. SDoH and HRSN are widely recognized as influencers of racial disparities in health outcomes. Systemic and structural racism are known to lead to higher levels of a variety of social needs31,32. Healthcare-seeking behaviors of individuals who identify as members of underserved minority groups may be influenced by unfamiliar cultural norms, community concerns, and/or histories of distrust of medical systems, and evaluation and treatment may be influenced by provider bias33,34. Third, while our study sample is large and diverse, it is nonetheless only comprised of individuals with insurance, and we are unable to comment on the potential relationship between HRSN and cost among the uninsured. Another challenge is that while many low-cost, easily accessible tools are available for HRSN screening, psychometric data on the reliability and validity of these tools is limited22,34. Additionally, patient cost sharing (i.e., co-pays and coinsurance) may influence utilization behaviors, though this was outside of the scope of the current study. Lastly, as detailed in the “METHODS,” we studied only direct costs and excluded indirect costs, and so our dollar estimates may not be a full estimate of all resources that go toward the provision of care or the broader impact that HRSNs have on patients’ lives.
While no empirical model can capture the complex and evolving understanding of these constructs perfectly, our analysis aims to provide timely insight into the associations between HRSN and cost, while controlling for the effects of those complicated dynamics as best as our data allow. As we gain a better understanding of these factors, we can begin to envision a system in which HRSN are effectively identified and incorporated into clinical decision making as well as system-wide resource allocation strategies, perhaps viewing HRSN as another aspect of health maintenance or preventive medicine.

Comments (0)