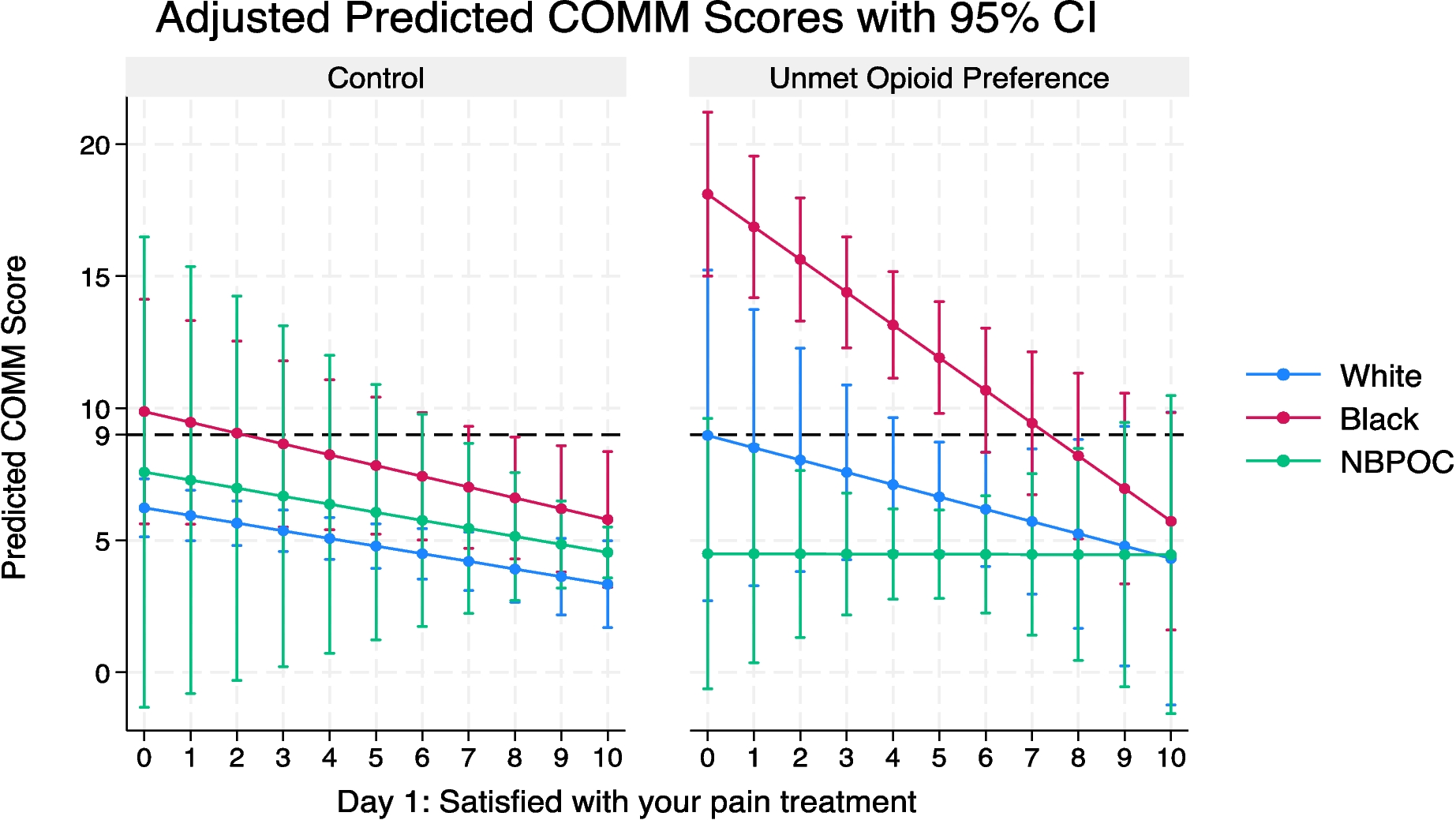
Our study has three main findings. First, among patients presenting to the ED with acute back or kidney stone pain, Black patients had greater opioid misuse risk 90 days after the initial encounter based on a previously validated measure. Second, unmet opioid preference was significantly associated with increased opioid misuse risk, but only among Black participants. Third, satisfaction with pain treatment was independently associated with lower opioid misuse risk, with the most potent effect on Black participants who experienced unmet opioid preference.
The finding that unmet opioid preference had a unique effect on opioid misuse risk among Black participants is consistent with our prior analyses of this cohort, in which we found that receiving a prescription for opioids at discharge was associated with lower odds of reported non-prescribed opioid use.13 Non-prescribed opioid use is a unidimensional measure, and confirming the effect of unmet opioid preference using the COMM score, a validated, multidimensional measure, is a novel contribution to the literature.
Similarly novel to our study is the finding that satisfaction with pain treatment significantly mediates the impact of unmet preference on opioid misuse, especially among Black participants. A few potential explanations may underlie this finding. While unmet preference may lead some individuals to seek relief through nonprescribed opioids, various factors during a clinical encounter may mitigate such risks, such as the expression of empathy, patient-centered communication, and patient education about effective therapies and opioid risk. Prior studies have found that physicians use less patient-centered language and show a lower level of positive affect with Black patients compared to White patients.19 These aspects of a clinical encounter can, in turn, be interpreted by patients negatively, and impact their satisfaction and follow-through with adherence to guidance including safe medication use.
It is possible that Black patients’ pain was underappreciated and thus undertreated in the acute setting, leading those with unmet preferences to seek relief via non-prescribed opioids. Evidence suggests that undertreated acute pain increases patients’ risk of developing chronic pain and persistent opioid use. Additionally, other studies have found, although different from “unmet preference,” that perceived discrimination in medical encounters is associated with greater odds of reporting illicit drug use.8,20 Perceived discrimination in medical settings has also been associated with more distrust in conventional medical settings and more favorable attitudes toward complementary or alternative medicine among Black people.7 For example, in the treatment of opioid use disorder, the use of non-prescribed buprenorphine to treat opioid use disorder was due to unmet needs and preferences from the care delivery system.21,22
Our findings have multiple implications. First, unmet opioid preference in the acute setting may be an overlooked pathway through which some Black people become vulnerable to opioid misuse. This is especially concerning given the evolution of the opioid overdose epidemic2,23 and increasingly unsafe opioid supply.24 Second, aspects of clinical encounters that shape patients’ satisfaction with their pain treatment may be among the tools to leverage to reduce adverse opioid events, especially among Black patients. Further studies should seek to understand factors that shape patients’ satisfaction with pain treatment and their potential impact on opioid misuse and adverse opioid events.
The racial and geographic diversity in our sample is a strength, as is the longitudinal nature of the study. We used satisfaction with pain treatment measured the day after the encounter, expecting the most accurate recall, and administered the COMM 3 months after the encounter, not simultaneously, which strengthens the argument for a causal relation between satisfaction with pain treatment and opioid misuse. Limitations of this study include the use of the COMM score, which was validated in a non-representative sample (83% White, 61% women, and 87.3% high school graduates).25 As a result, the assessment of opioid misuse risk may not be as valid an assessor of aberrant drug behavior in the racially diverse sample used in this study. However, we have previously found similar results using single metric measures of opioid misuse, such as non-prescribed opioid use. Participants in this study were followed for only 3 months with significant attrition, and opioid misuse risk as an outcome may not be as clinically significant over this timeline. A longer-term follow-up with this cohort would be necessary to confirm the clinical significance of our findings.

Comments (0)