
Remember me
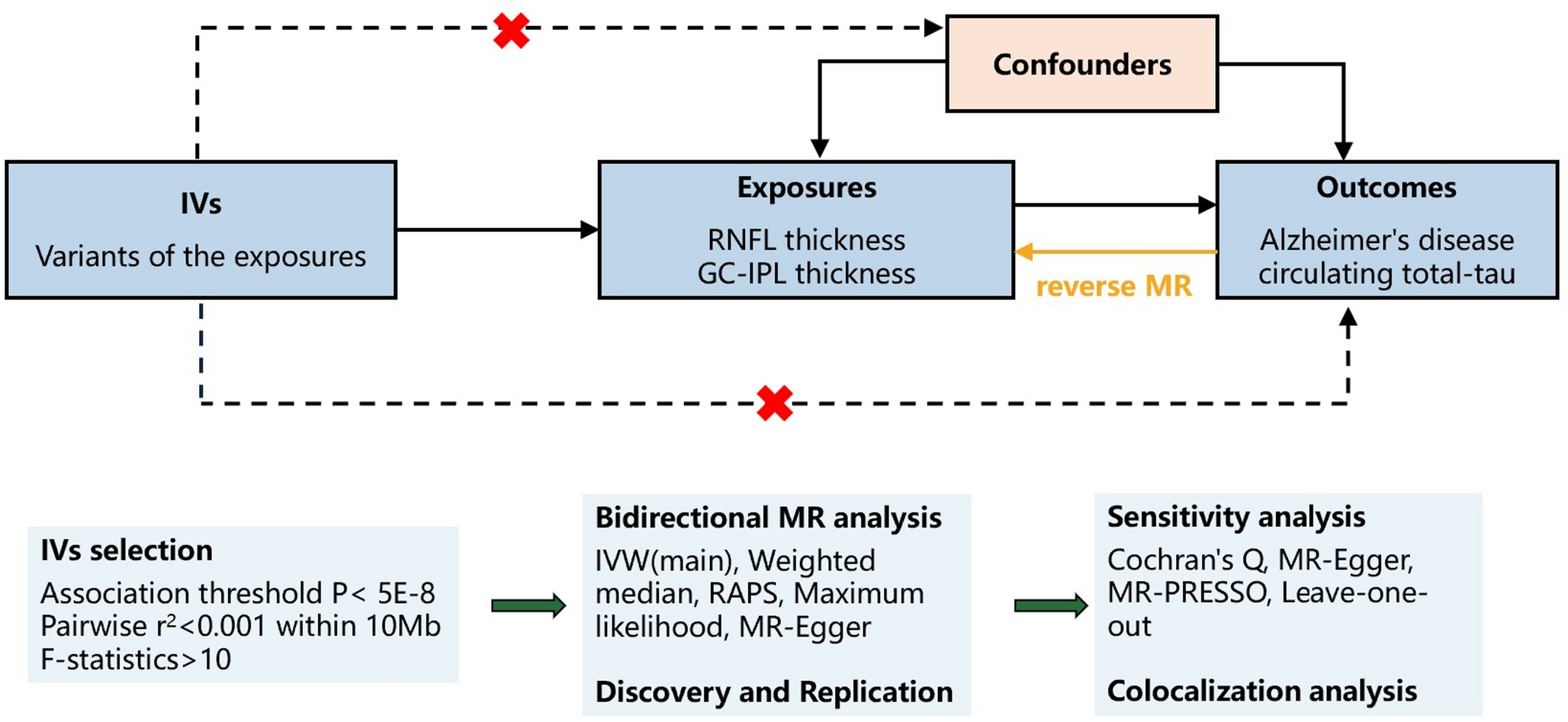
Since the publication of the HTT expansion test in 1993, the recognized phenotype of HD has broadened. This survey aimed to establish what HD experts consider typical and when they might order a genetic test, considering clinical presentation and ethical implications. The results highlight typical HD symptoms—chorea, dystonia, cognitive slowing, apathy, and depression—while emphasising the condition’s heterogeneity, as well as subtle initial cognitive and psychiatric symptoms. Insomnia, dysarthria, and dysphagia are common in HD, while progression usually leads to gait disturbances and falls. Interestingly, 20% of respondents maintained their expectation of a positive HD test, even when symptoms typically associated with other syndromes were present, provided a primary HD symptom was evident. Indeed, this is consistent with our recent study demonstrating that HD and HDPC patients tested for HD, whose test result is negative are clinically indistinguishable [2]However, the emphasis given to chorea was misplaced as the rate of chorea was similar in both the HD and HDPC cohorts [2]. Consistent with HD experts expectations, the lack of any relevant family history of cognitive, psychiatric or motor symptoms currently appears to most strongly indicate a likely negative HD test [2]. Rather than being a result of alleged indiscriminate genetic testing, the increase in negative HD test results therefore reveals the increasing acceptance of HD pleiotropy (Fig. 1).
Fig. 1
Symptoms deemed typical or atypical for HD. This figure shows the symptoms HD experts deemed typical or atypical for HD, with answers for HD shown in black and for HD-like in stripes. Answers are shown as a percentage of HD experts answering positively for each symptom and each category
Genetic testing requires informed consent, which can become complex when patients have cognitive impairments [6]. Predictive testing for neurodegenerative diseases, traditionally managed by clinical geneticists, follows established protocols but can be emotionally taxing. Consequently, uptake rates are typically low, averaging around 20–25% for conditions like HD and prion disease [6, 7]. However, the advent of successful treatment trials for genetic neurological disorders [8] is likely to alter these trends. The number of CAG repeats in the HTT gene inversely correlates with AAO; however, this correlation is non-linear and accounts for only about half of the observed variation [1]. The toxicity associated with the CAG repeat expansion arises from multiple factors, including full-length expanded huntingtin, N-terminal huntingtin fragments, aberrant splicing of intron 1 of the HTT gene, and somatic expansion of the CAG repeat [8]. AAO and disease progression in HD are influenced by genetic loci within DNA repair genes, such as FAN1 [9, 10], whose proteins influence somatic CAG repeat expansion [11]. Although the phase 3 efficacy trial for Tominersen, an antisense oligonucleotide, was halted due to poorer clinical outcomes and increased serious adverse events in the high-dose group [8], targeting HTT and its genetic modifiers remains promising. These approaches aim to address the molecular root of HD, potentially paving the way for curative treatments for HD and other expansion disorders in the future [12]. The study is limited by the subjective nature of the survey and low or zero cell counts in some symptom categories, which may affect the robustness of the Chi-square tests. The approach was retained for analytic consistency, and the study remains representative of usual clinical practice given the respondents’ expertise.
Comments (0)