
Remember me
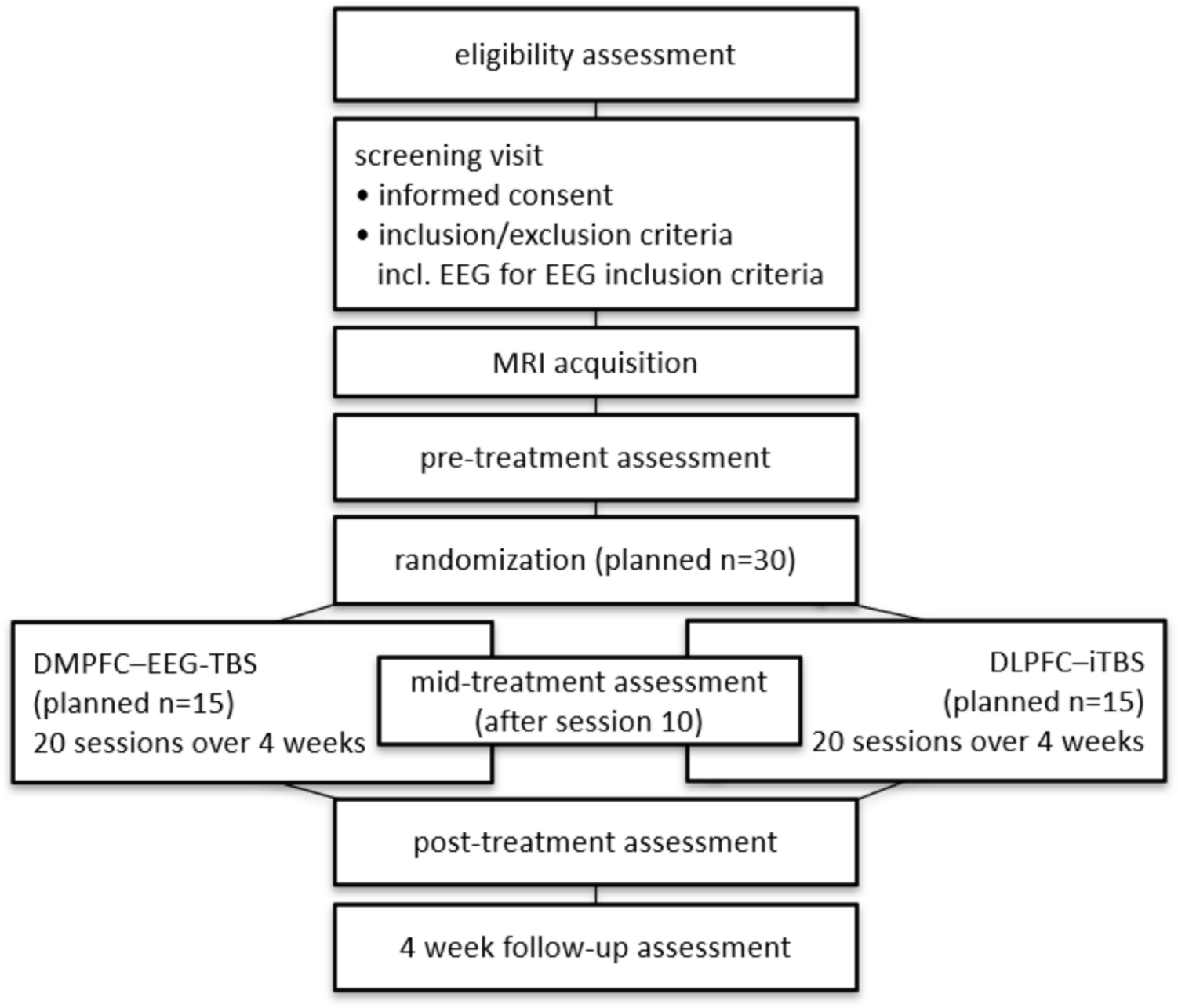
Subjects will be randomized to one of two arms of daily rTMS interventions for four weeks (5 sessions per week on working days, 20 sessions in total). In the experimental EEG-synchronized condition, TMS will be triggered at the trough of the theta oscillation extracted from left DMPFC. The control condition will consist of rTMS therapy applied to the left DLPFC following an FDA approved iTBS protocol [15] (s. Figure 2):
1)Experimental arm (DMPFC-EEG-TBS):
Fig. 2
Schematic comparison of the experimental EEG-synchronized theta-burst stimulation (DMPFC-EEG-TBS) and the control condition with standard iTBS (DLPFC-iTBS)
Triple pulses at 100 Hz are delivered in bursts phase-locked to the trough of the individual theta oscillation (4–8 Hz) recorded over the left dorsomedial prefrontal cortex (DMPFC) (s. figure 2). Although rising or falling phases of theta oscillations may transiently exhibit higher instantaneous excitability, previous work has demonstrated that stimulation precisely at the trough yields the most reliable and long-lasting plasticity-like effects [30, 31, 39]. By adopting 100 Hz we rely on evidence, that higher intraburst frequencies strengthen plasticity-like effects within established safety margins [40, 41]. Extending this rationale, frequency-dependence has been shown with state-dependent bursting in motor cortex, where 100–200 Hz bursts at the trough of the ongoing μ-rhythm reliably increased cortical excitability, whereas 60 Hz did not [39]. In our protocol, bursts are phase-locked to the trough of the endogenous frontal theta oscillation over left DMPFC to exploit a receptive excitability state for plasticity induction [30]. Bursts are triggered on roughly every 15-20th trough, yielding a mean inter-burst interval of approximately 3.5 s, consistent with our prior prefrontal real-time work reporting 3.49 s (SD ± 2.01) . A minimum inter-burst interval of 1.0 s is enforced to ensure artifactfree phase estimation following each burst. Under these constraints the session delivers 600 pulses and lasts about 11 min 38 s, as shown in Figure 2.
2)Control arm (DLPFC-iTBS):
Standard intermittent theta-burst stimulation (iTBS) is applied to the left dorsolateral prefrontal cortex (DLPFC) according to FDA-approved parameters (50 Hz triplets repeated at 5 Hz, 2 s trains followed by 8 s pauses) until 600 pulses are delivered, resulting in a total duration of about 3 min 10 s.
In the experimental arm, bursts of three pulses at 100 Hz are phase-locked to the trough of the ongoing theta oscillation (4–8 Hz), ensuring synchronization with intrinsic brain rhythms. Circles highlight stimulation timing relative to the oscillatory phase. Of note, in the experimental condition, stimulation is not delivered on every detected theta trough but occurs with a mean inter-burst interval of approximately 3.5 s, corresponding to every 15th–20th theta cycle. In the control arm, bursts of three pulses at 50 Hz are delivered in a fixed 5 Hz pattern independent of the EEG signal (open-loop). Hereby each session in the control condition consists of 600 pulses applied in 2 s “on” / 8 s “off” cycles.
In both interventions, 600 TMS pulses will be delivered per session corresponding to 12.000 TMS pulses during the entire 4 weeks of TMS therapy. Stimulation intensity will be set to 120% resting motor threshold (RMT) or the highest tolerated intensity if this is below 120% RMT. If required, a ramp-up period will be used for a maximum of the first three sessions to accommodate patients that don’t immediately tolerate the desired stimulation intensity. Stereoscopic neuronavigation (Localite GmbH, Bonn, Germany) based on individual anatomical MRI data will be used to position the coil, where DMPFC and DLPFC target locations will be pre-determined based on the individual MRI data and identifying the respective target gyrus using standard anatomical methods [42].
To ensure blinding of the patients, all setup components are implemented identically in both conditions, that is, a surface EEG is recorded through a 5-channel equipment during the TMS intervention in both the experimental and in the standard condition. But only in the experimental condition is the EEG used to trigger the TMS pulses; in the control condition, the EEG is recorded but not considered for triggering the TMS pulse. To ensure double-blinding, the rater is blinded as well, as the rater must not be present during the intervention procedure and does not have access to non-rater-related documentation.
Measurement proceduresThe MRI images will be acquired at a Siemens 3 Tesla MRI scanner in the MRI Research Center of Tübingen (Department Biomedical Magnetic Resonance, Prof. Dr. phil. nat. Dipl.-Phys. Klaus Scheffler, Hoppe-Seyler-Str. 3, 72076 Tübingen). Patients are placed in the scanner with earplugs and an emergency ball. Visual and verbal contact to the patients is maintained from the control room. No drugs or contrast agents are used during MRI examinations.
Study participants are evaluated by a medical doctor for MRI contraindications and need to give written informed consent before the scan. Subjects are required to give written consent that if the scan reveals a gross anatomical abnormality, they will be informed and need to take further diagnostic work-up outside of the study. Acquired scans are performed for scientific reasons with parameters optimized according to the requirement of the stimulation and thus do not provide sufficient diagnostic value in case of structural abnormalities.
Study participants will be seated on a comfortable reclining chair with both arms relaxed. A high-frequency capable TMS stimulator (MagPro XP, MagVenture, Denmark) with a figure-of-eight coil (Cool-B65, inner coil winding diameter 35 mm) and a TMS-compatible EEG setup (ActiCHamp, BrainProducts, Gilching, Germany) will be used. For DMPFC-EEG-TBS, TMS pulses will be triggered from a custom real-time digital biosignal processing system based on the ongoing oscillatory theta brain activity in the left DMPFC as recorded by surface EEG.
Stereoscopic neuronavigation (Localite GmbH, Bonn, Germany) will be used to track the position of the coil relative to the head and to determine the appropriate stimulation sites (DMPFC and DLPFC, respectively).
EEG recordings will be carried out using a TMS-compatible, optically isolated amplifier (ActiCHamp, BrainProducts, Gilching, Germany).
For the theta screening and the pre- and post-assessment surface EEG series will be recorded for 5 min with eyes open using a TMS-compatible 32-channel gel filled sintered ring electrode EEG cap (ActiCap, BrainProducts, Gilching, Germany) using the same optically isolated amplifier as described above. Electrode impedances are kept below 10 kΩ, the sampling rate is set to 1,000 Hz with 24-bit resolution, and FCz serves as the reference electrode. The primary purpose of the screening EEG procedure is to evaluate the presence of a detectable theta rhythm in the 4–8 Hz frequency range over midline frontal electrodes. Spectral power is computed in real time, and a graphical representation of the frequency spectrum is generated for visual inspection. A clearly identifiable theta peak is required for study inclusion, as the EEG-synchronized stimulation depends on reilable phase detection in this frequency band. This screening step ensures the technical feasibility of the intervention and serves as an additional eligibility criterion. In addition to the screening EEG, resting-state EEG is also recorded immediately before the start of treatment (pre-assessment) and after the final stimulation session (post-assessment). The purpose of these recordings is to evaluate changes in spectral power and functional connectivity across treatment, with a focus on the theta frequency band. Exploratory analyses will also investigate alterations in other frequency ranges and potential shifts in frontal network dynamics.
For the stimulation sessions, a five-channel setup is employed with an AFF1h-centered Hjorth montage (AFF1h, AFF2h, AFp1, FFC1h, AFF5h) to capture frontal theta oscillations over the left dorsomedial prefrontal cortex (DMPFC) . EEG is recorded with the identical montage and equipment in both conditions as described above, but is not used to control the timing of stimulation in the control condition, thereby maintaining blinding while also enabling exploratory offline analyses.
The real-time pipeline consists of a band-pass filter in the theta range (4–8 Hz), a 50 Hz notch filter to remove line noise, and continuous monitoring for artifacts. Theta oscillations are extracted from the AFF1h channel, and instantaneous phase is computed using a Hilbert transform with latency compensation. TMS bursts are triggered at the trough of the theta cycle, with prediction to compensate the fixed delay of 15–20 ms arising from amplifier buffering, signal processing, and stimulator triggering; the predictor advances the command by ~ 30–45° at 6 Hz [30]. To allow undisturbed phase estimation, a hard refractory period of 1.0 s is imposed after each burst. Thereafter, the next eligible trough is used, selecting every 15-20th trough to obtain a mean interburst interval ~ 3.5 s. Session level phase-locking metrics are computed online to verify timing accuracy (see also Fig. 2). This calibration procedure follows established practice in phase-specific TMS research [30] and recent delay analyses highlighting uncompensated transport latency as a critical determinant of phase-locking accuracy [43]
Surface electromyography (EMG) will be obtained through an optically isolated battery powered biosignal amplifier (ActiCHamp, BrainProducts, Gilching, Germany) using bipolar electrodes from right hand muscles (first dorsal interosseous and abductor pollicis brevis muscles). This enables determining the RMT, which is needed to individualize stimulation intensities during the rTMS protocols. RMT is defined as the minimum stimulus intensity needed to evoke motor evoked potentials (MEP) of > 50 µV peak-to-peak amplitude in the target muscle in at least 5 out of 10 consecutive trials using a figure-of-eight TMS coil oriented 45° away from the midline over the hand representation of left primary motor cortex [44]. Patients will be requested to relax and stay awake during the experiments.
Clinical assessments regarding the severity of the depression before and after the TMS treatment will be performed by a blinded rater using the MADRS and HDRS-17 scales.
Subjects will be asked to complete the Beck-Depressions-Inventory-II (BDI-II) (this will take 5 min) and the Inventory of depressive symptoms-30 (IDS-30) (this will take 10 min) at baseline (pre-assessment), after the 10th session (intermediate assessment), after the last session (post-assessment) and at the follow-up visit four weeks after the last intervention (follow-up assessment). Following each intervention session, a structured self-report will be documented, to assess whether any side-effects occurred from the stimulation. Side effects will be documented on a separate adverse event sheet.
Criteria for discontinuing or modifying allocated interventionsIf the stimulation is not tolerated by the patient, the stimulus intensity will be first adjusted to the highest tolerated intensity and then gradually adjusted to the required intensity over max. 3 sessions. If the patient cannot become acquainted with the treatment conditions (e.g., stimulus intensity) within three sessions, additional participation is not feasible. Withdrawal from the study is also required if the subject misses more than 4 planned treatment sessions. In the case of up to 4 missed planned treatment sessions, the missed sessions will be offered at the end of the intervention period, so that each enrolled patient will receive 20 sessions. However, we strive to keep the number of treatment cancellations and postponements to a minimum. Patients who withdraw from the study will be included in the primary statistical analysis (cf. section “Statistical Methods”).
Strategies to improve adherence to interventionsAdherence to the intervention is considered to be high as patients decide to participate in this brain stimulation study on their own initiative. TMS treatment is non-invasive, painless and is generally considered to be well tolerated. Participation adherence is expected to be also increased by the ramp-up method with a familiarization phase to the stimulation intensity (if required) and the possibility of 4 missed planned treatment appointments.
Relevant concomitant care permitted or prohibited during the trialNo specific antidepressant medication is mandatory. However, if present, the antidepressant therapy must be kept constant, which means that medication at or above the “minimum oral dose” (MOD) specified in the Antidepressant Treatment History Form: Short-Form (ATHF-SF) [45] has to remain unchanged 4 weeks before and 6 weeks during study treatment. Changes below the MOD are considered as uncritical. Changes after the end of treatment are registered in the follow-up sessions. Critical changes during the treatment period lead to exclusion from the per protocol analysis.
Patients are advised not to undergo any concomitant therapies if possible. In the case of ongoing therapies (e.g., psychotherapy), patients are asked to keep these constant in intensity and frequency throughout the study period.
Provisions for post-trial careAncillary treatment is not planned during the intervention period due to confounding influence. In case of severe mental health conditions (e.g., suicidal ideation), requiring immediate standard of care treatment (inpatient, psychotherapeutic), the patient will be transferred to treatment by the established infrastructure. In the same manner, post-trial care is provided in case of severe disease aggravation by the end of trial participation.
If a participant withdraws prematurely from the study, their reasons, circumstances, and final status will be documented where possible. If the patient does not withdraw the consent for further follow‐up, he/she will be followed‐up as planned. If any harm arises from participation, such as an epileptic seizure or headache, standard treatment for the symptoms will be provided at the hospital immediately.
No post-treatment taper phase is included within the present protocol, since the trial was designed to closely mirror the FDA-approved iTBS standard and the addition of taper sessions was not feasible within the capacity of a pilot study. However, outside the study, participants have the opportunity to receive further treatment in our Day Clinic for Brain Stimulation, where standard iTBS is routinely available as part of clinical care. This option does not constitute a study-related provision but reflects the regular treatment pathways available to all patients. This ensures that participants who require continuation therapy can receive it under standard clinical conditions.. Future confirmatory trials will address this issue by incorporating taper phases or maintenance protocols, thereby providing a more complete picture of how oscillation-synchronized TBS can be implemented in clinical practice.
Comments (0)