Systematic literature review
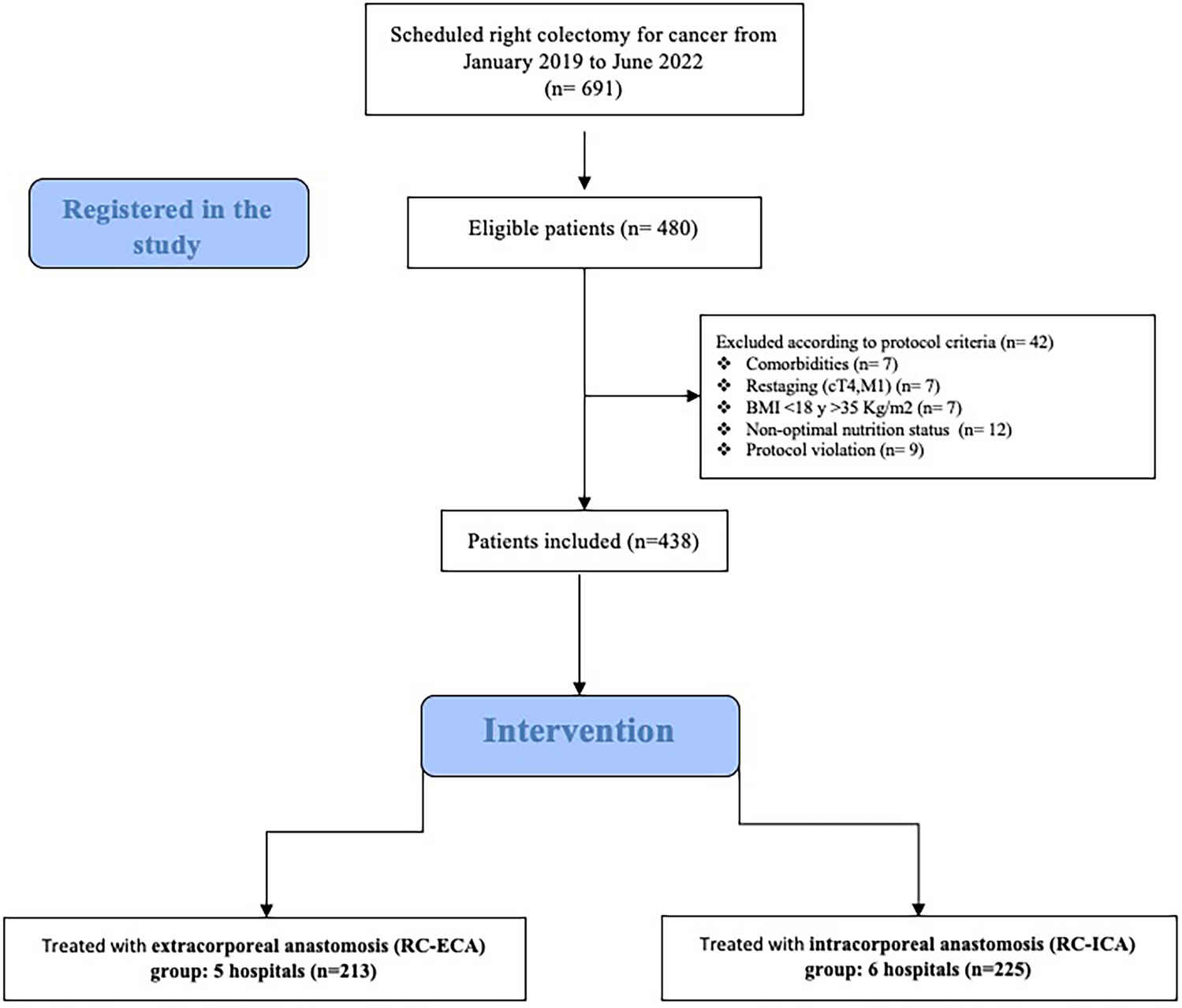
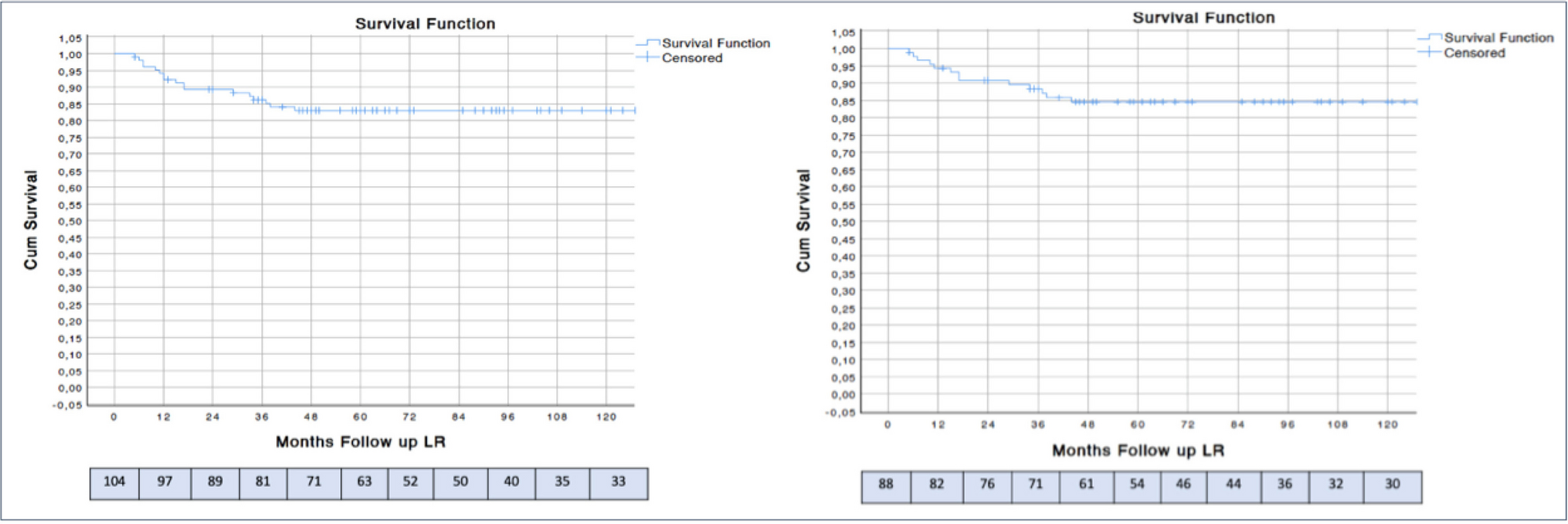
A total of 20 studies met the inclusion criteria and were analyzed in detail [8, 16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34]. Several studies were excluded based on pre-specified criteria: one study was excluded due to its focus on pediatric patients [35], one did not specify the sclerosing agent used [36], and one study used a sclerosant other than polidocanol [37]. Additionally, three studies were excluded as letters to the editor [38,39,40], four were video vignettes [41,42,43,44], and three were editorials [12, 45, 46]. Three meta-analyses [47,48,49] were reviewed to extract additional studies that were not identified in the initial search (Fig. 1).
Nearly half of the studies (9/20, 45%) were conducted in Italy [16, 22,23,24,25, 28, 30,31,32]. The majority were prospective, including six randomized controlled trials [8, 18, 21, 26, 33, 34]. Only three studies were retrospective [22, 29, 32], while eight studies were multicenter investigations [8, 23, 25, 27,28,29,30, 34] (Table 1). Table 1 summarizes the main characteristics of the studies, including clinical indications for polidocanol foam sclerotherapy. Most studies targeted patients with grade I–III hemorrhoidal disease, with particular consideration to cases involving bleeding diathesis, patients unfit for surgery, or those with recurrence after previous treatments such as RBL. The number of treatment sessions ranged from one to three, and clinical success rates varied between 68 and 100%, with low recurrence rates reported at a median follow-up of 12 months. Reported complications were generally mild and self-limiting. Table 2 provides an overview of adverse events, with pain, pruritus, and transient bleeding being the most frequently observed. Serious complications were rare.
Table 1 Summary of studies on polidocanol foam sclerotherapy for hemorrhoidal diseaseTable 2 Postoperative complications following polidocanol foam sclerotherapy for hemorrhoidal diseaseExpert survey study
A total of 30 experts in proctology, colorectal surgery, and minimally invasive treatments for HD participated and completed the survey. The majority were male (25/30, 83.3%), with most participants aged between 40 and 60 years (24/30, 80%). Geographically, the highest number of surgeons came from China (14/30, 46.7%), followed by Italy (11/30, 36.7%), Portugal (2/30, 6.7%) and France, Germany and Poland (1/30, 3.3%), and the majority worked in teaching hospitals (24/30, 80%). Over half were colorectal surgeons (16/30, 53.3%), 5 anorectal surgeons/proctologists (16.7%), 4 general surgeons (13.3%), 4 gastroenterologists (13.3%) and 1 angiologist (3.3%) (Appendix 1).
The survey documented how polidocanol foam sclerotherapy is currently performed in clinical practice. Responses were grouped into five key areas: (1) indications and contraindications, (2) perioperative management, (3) procedure details, (4) postoperative care and follow-up, (5) comparative effectiveness and safety profile.
Indications and contraindications
Most respondents (27/30, 90%) reported using polidocanol foam sclerotherapy primarily for Goligher grade II HD. The procedure was particularly favored in elderly patients with significant comorbidities (23/30, 76.7%). Additionally, 16/30 (67%) of respondents considered it suitable for grade III HD, though its use in grade IV cases was less common (8/30, 26.7%). A relevant subset of experts reported using sclerotherapy in patients on anticoagulation therapy (18/30, 60%). The “bridge to surgery” option, widely adopted during the COVID-19 pandemic, was considered in 13 out of 30 respondents (43.3%). In rare cases, polidocanol foam was employed in patients with inflammatory bowel disease (IBD) (2/30, 6.6%), pregnancy (4/30, 13.3%) or as part of a combined approach with RBL (11/30, 36.7%) or excisional procedures (1/30, 3.3%). Regarding contraindications, the most commonly reported were anal abscess (22/30, 73.3%) and anal stenosis (17/30, 56.7%).
The ISG recommends the use of Sclerotherapy for patients with grade I-III HD (Strong Consensus: 100%). Moreover, the procedure could be performed in elderly patients, in patients on anticoagulation therapy, in medically-controlled-IBD and in combination with excisional hemorrhoidectomy (Strong Consensus: 93.3%). The application of sclerotherapy for patients with grade IV HD must be aimed exclusively at treating symptoms, even with the intent of bridging to surgery (Strong Consensus: 83.3%).
Perioperative management
Preoperative preparation for polidocanol foam sclerotherapy was not standardized, with notable variations in clinical practice among surgeons. The majority of practitioners incorporated some form of medical management before the procedure, with stool softeners being the most commonly prescribed (15/30, 50%), followed by high-fiber diets (12/30, 40%) and systemic flavonoids (11/30, 36.7%). A smaller proportion (4/30, 13%) recommended topical flavonoids. The duration of pre-treatment also varied, with most surgeons opting for a four-week course (6/30, 31.6%), while others preferred a shorter, two-week regimen (3/30, 15.8%).
The setting in which the procedure was performed also differed among respondents. Just over half of the surgeons (16/30, 53.3%) conducted sclerotherapy in an outpatient office setting, while 9/30 (30%) preferred a day surgery unit, and 5/30 (16.7%) performed the procedure in an inpatient setting.
Anesthesia use was another area of variability. Half of the surgeons (15/30, 50%) performed the procedure without any anesthesia, whereas nearly a third (9/30, 30%) used lidocaine gel for local analgesia. Preoperative bowel preparation was also inconsistent: enemas (single or double the night before and a few hours before the procedure) were administered in 22/30 cases (56.7% single; 16.7% double), whereas 7 surgeons (50%) opted to proceed without any bowel preparation.
The ISG recommends the use of a 4-week preoperative therapy with local and systemic flavonoids, stool softeners, high-fibers diet to strengthen the effectiveness of sclerotherapy (Strong Consensus: 100%). A preoperative bowel preparation with single or double enemas could be chosen (Strong Consensus: 93.3%). The procedure must be performed in an outpatient setting if possible and if the local organization allows it using lidocaine gel (Strong Consensus: 100%).
Procedure details
The preferred concentration of polidocanol foam varied among surgeons, with the majority (17/30, 65.4%) favoring a 3% solution. A smaller proportion opted for a lower concentration, with 1% being used in 7/30 cases (26.9%) and 2% in 2/30 cases (7.7%). Foam preparation methods were also diverse, with nearly half of the surgeons (12/30, 46.1%) using the Tessari method, while 10/30 (38.5%) and 2/30 (7.7%) relied on the EasyFoam kit© and automated devices (i.e. Varixio ©), respectively, reflecting the recent evolution of new preparation methods.
Variability was also observed in the choice of injection needle gauge. The most frequently used diameters were 20G (7/30, 23.3%), followed by 22G (5/30, 16.7%) and 23G (4/30, 13.3%). Regarding the injection technique, the majority of surgeons (19/30, 63.3%) preferred an intra-pile approach, while a smaller proportion (10/30, 33%) opted for submucosal injection.
The volume of foam injected per hemorrhoidal pile was typically 2 mL (20/30, 66.7%), though in some cases it was increased to 3 mL (5/30, 16.7%). The total volume administered per session varied, ranging between 6 and 14 mL (26/30, 86.7%), with most surgeons (25/30, 83.3%) adjusting the dose based on hemorrhoidal grade.
The ISG recommends the use of 3% liquid polidocanol to generate the foam, if possible, with an automated, non-operator dependent method, and the injection should be performed intra-pile with an open-ended anoscope and a 20 G needle and with a tailored use of 2–4 cc of foam per pile based on the degree of HD to be treated (Strong Consensus: 83.3%).
Postoperative care and follow-up
Post-treatment care varied among surgeons, with most recommending supportive measures to enhance recovery and symptom resolution. Stool softeners were the most frequently prescribed intervention (23/30, 76.7%), followed by increased water intake (20/30, 66.7%) and systemic flavonoids (17/30, 56.7%).
Patients were typically reassessed within two to four weeks after the procedure, with follow-ups scheduled at two weeks in 10/30 cases (35.7%) and at four weeks in 9/30 cases (32.1%). Treatment success was primarily determined based on patient-reported outcomes (24/30, 80%), often supplemented by anoscopic evaluation (20/30, 66.7%) to assess the persistence of symptoms or resolution of hemorrhoidal disease.
A second session of sclerotherapy was generally not planned as part of routine care. However, in cases where patients continued to experience symptoms, additional sessions were considered on an individual basis (23/30, 76.7%).
Postoperative therapy should be consistent with preoperative therapy and should be administered for at least 4 weeks after the procedure (Strong Consensus: 83.3%). The ISG suggest a follow-up visit within 4 weeks of the injection to evaluate on an individual basis the execution of a possible further sclerotherapy injection (Strong Consensus: 100%).
A 4-week window must be respected between the first and second injection while subsequent procedures can be performed, on a symptomatic basis, after at least 3 months (Strong Consensus: 100%).
Comparative effectiveness and safety profile
Survey responses indicated that polidocanol foam sclerotherapy is perceived as having superior outcomes compared with RBL and dearterialization procedures. Success rates were higher with polidocanol foam (88.3%) compared to RBL (66.7%), while recurrence rates were notably lower for sclerotherapy (16.1% vs. 41.2%) [26]. Additionally, complication rates were reduced in the sclerotherapy group (10.0%) compared to RBL (30.0%) [26]. Postoperative pain was also reported as lower among patients undergoing sclerotherapy compared to those treated with RBL [19, 50]. A meta-analysis comparing sclerotherapy to RBL confirmed these findings, supporting the safety and efficacy of polidocanol foam [48]. When compared to dearterialization and mucopexy, sclerotherapy demonstrated similar success rates but a more favorable safety profile, with fewer postoperative complications such as hemorrhage, thrombosis, and perineal abscess [32, 33]. Mucopexy was found to be associated with a sixfold higher risk of complications compared to sclerotherapy [33].
In terms of safety, adverse events were infrequent (Table 2). Mild pain was reported by 8.0% of patients, typically short-lived and self-limiting. Bleeding requiring hospital admission occurred in four cases, predominantly in patients receiving anticoagulant therapy. Additionally, two cases of rectal abscesses were documented, both requiring surgical drainage. Despite these rare complications, polidocanol foam was generally well-tolerated, reinforcing its safety profile in the treatment of HD.
The ISG recommends the use of sclerotherapy as the first approach in patients with grade I-III HD. A combination with rubber band ligation may be considered in patients who are not at risk of postoperative bleeding (Strong Consensus: 100%).

Comments (0)