This binational survey provides the most detailed snapshot to date of parastomal hernia prevention and repair practices among colorectal surgeons in Australia and New Zealand. The health systems are mixed public and private and services are geographically dispersed. We observed substantial variability from stoma creation through to elective and emergency repair, which points to a gap between evidence and day-to-day practice and a lack of shared technical standards.
Internationally, variation in stoma construction, prophylactic mesh use at index formation, and operative strategy for parastomal hernia repair appears to be the rule rather than the exception. Surveys from Europe [12] and North America[13] have reported heterogeneous approaches to fascial aperture and maturation technique, selective uptake of prophylactic mesh despite trial and guideline-level support [1], and marked variation in elective repair configuration and mesh strategy. These reports suggest that practice is shaped not only by evidence, but also by training exposure, operative volume, and local infrastructure. In Asia, guidance from the Japan Society of Coloproctology similarly describes prophylactic synthetic mesh as a preventive option at index stoma creation and supports mesh-based repair as standard for parastomal hernia, discouraging primary suture repair or stoma relocation because of high recurrence [14]. Within this broader context, our Australasian findings align with international heterogeneity, while also pointing to potential system-level contributors in geographically dispersed services, including variable access to abdominal wall expertise and differences in prosthetic governance and procurement across public and private practice.
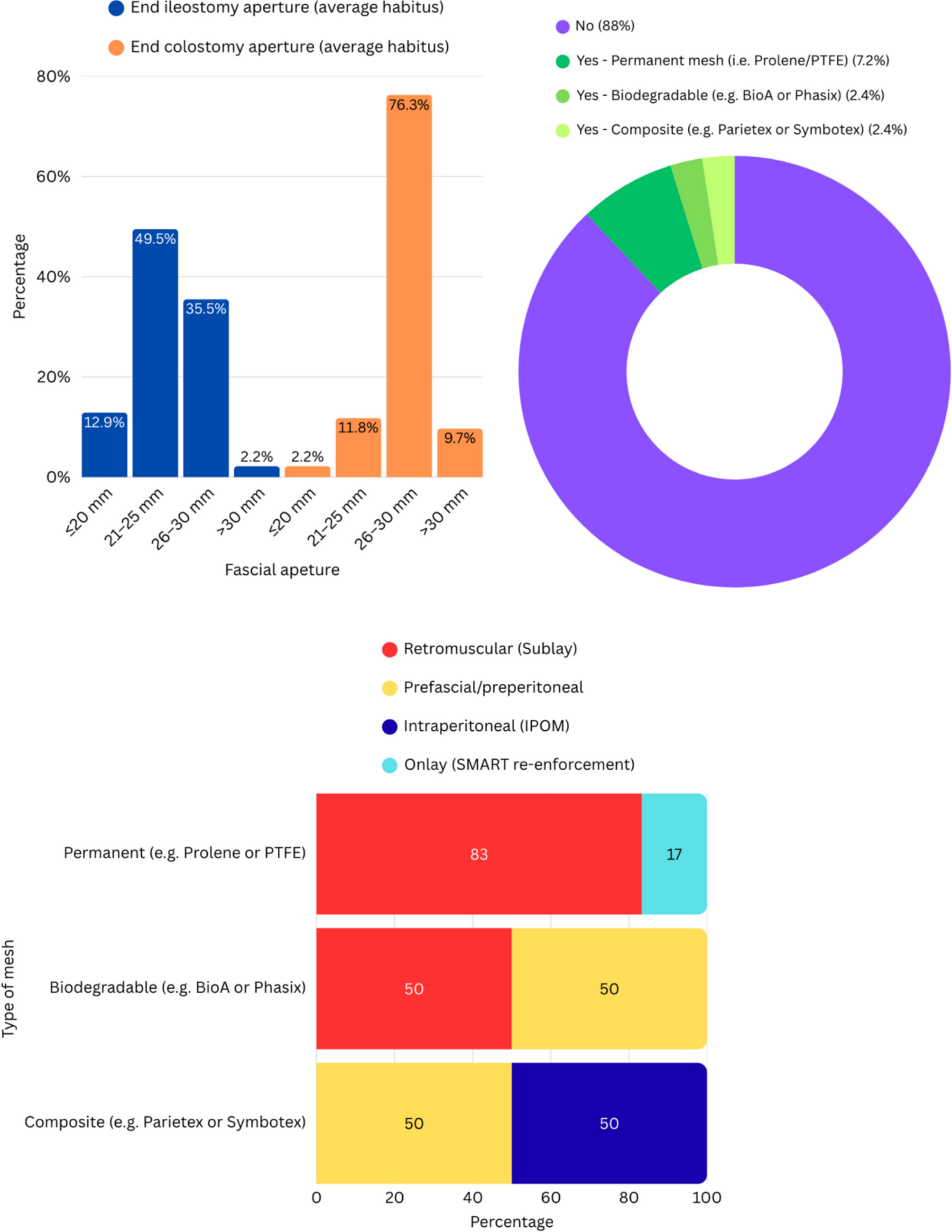
Prophylactic mesh placement at stoma formation remains rare, reported routinely by only 12% of respondents. This aligns with international trends despite high-level evidence from trials such as ROCSS [15], PREVENT [16], and STOMAMESH [17] suggesting safety and efficacy. Concerns about infection, limited exposure to mesh techniques, and medico-legal caution may explain the reluctance [18]. Even among mesh users, there was no consensus on material type or anatomical plane, underscoring the need for procedural standardisation and practical guidance.
In Australasia, implementation barriers may be amplified by system and geography. Services are dispersed across large catchments, abdominal wall expertise may be variably available, and procurement constraints can limit consistent access to composite or biosynthetic meshes, particularly in public hospitals. Operating time, cost sensitivity, and differing local governance around prosthetic use may further discourage routine adoption even where surgeons accept the trial evidence. These factors likely contribute to the observed lack of consensus on mesh material and plane among the minority who use prophylactic mesh.
Routine stoma formation practices were similarly inconsistent. While most respondents favoured vertical fascial incisions and traditional aperture sizes (1.5–2 fingerbreadths), a notable minority opted for cruciate or larger openings. Although subtle, these variations may influence long-term outcomes such as hernia development, and their persistence highlights the lack of operative norms [19]. Consensus-driven checklists and training modules for stoma creation may help reduce this variation.
Elective repair strategies were diverse. While mesh was widely adopted, operative access (open vs minimally invasive) and mesh configuration (e.g., Sugarbaker, keyhole, retrorectus) varied markedly. Notably, open repair was associated with a greater likelihood of keyhole or retrorectus techniques, while minimally invasive access favoured Sugarbaker. This suggests that operative access often dictates technique more than clinical phenotype or evidence, reinforcing the need for comparative data to guide configuration selection.
Several additional observations merit comment. In emergency scenarios, surgeons with > 15 years’ experience were more likely to favour mesh placement, suggesting that decision-making is shaped more by seniority and comfort than consensus or guideline. Geographic disparities were also observed, with New Zealand surgeons reporting lower operative volumes than their Australian counterparts, potentially reflecting differences in centralisation or referral pathways. Overall, 70% of respondents reported fewer than five repairs annually, raising concerns about procedural proficiency and reinforcing the case for collaborative training frameworks and national audit.
Emergency decision-making exhibited the greatest heterogeneity, particularly around mesh use in contaminated fields, stoma re-siting, and redo repair strategies. These responses reflect the lack of high-quality evidence and practical guidance in reoperative scenarios. Given the high stakes and technical demands of emergency and recurrent repair, this domain represents a key target for research, protocol development, and skills training.
This study is strengthened by its structured, scenario-based design and binational scope. Several limitations warrant emphasis. First, the response rate was 25.5%. This is comparable to other surgeon surveys on parastomal hernia prevention and repair [9, 12, 13] but nonetheless introduces a material risk of non-response and selection bias. Respondents were weighted towards senior, metropolitan surgeons, and practice patterns among provincial surgeons or those with less engagement in PSH surgery may be under-represented. Second, the sampling frame was restricted to CSSANZ membership; surgeons undertaking colorectal practice outside the society were not captured, which limits external validity. Third, vignette-based responses standardise clinical context but cannot reproduce real-world constraints such as time of day, contamination, resource availability, and local rostering or supervision models. Accordingly, the observed association between seniority and emergency mesh preference should be interpreted as a difference in stated preference rather than a direct map of institutional decision-making. Finally, subgroup analyses were exploratory, with no correction for multiple comparisons.

Comments (0)