This was a pragmatic, prospective multicenter cohort in which the anastomotic approach (ICA vs ECA) reflected each hospital’s routine practice. The study was designed and reported in accordance with the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) guidelines [13, 14]. To enhance clarity and transparency, our reporting also aligns with key principles of the recently proposed TARGET guidance for observational studies emulating a target trial [26]—explicitly specifying eligibility, time zero (day of surgery), treatment strategies (ICA vs ECA as center-level routine practice), outcomes, and prespecified adjustment for baseline confounders (including propensity score methods). Because exposure was determined at the center level, the design reduces within-hospital selection but may introduce between-hospital confounding.
Participating hospitals were experienced in both techniques, yet each routinely used a single approach. The review board deemed randomization between approaches unethical where one was not the local standard. As Victora et al. [27] have emphasized, randomized trials are not always practical or ethical for evaluating health interventions in real-world settings. Within these constraints, a nonrandomized, center-level exposure design offered the most feasible and transparent approach. To minimize potential between-hospital confounding, we included only certified colorectal units with comparable perioperative pathways and a single standardized anastomotic strategy in routine practice, and we adjusted remaining imbalances—including ERAS adherence, prehabilitation, and extraction-site/incision—using multivariable analyses and propensity-score matching.
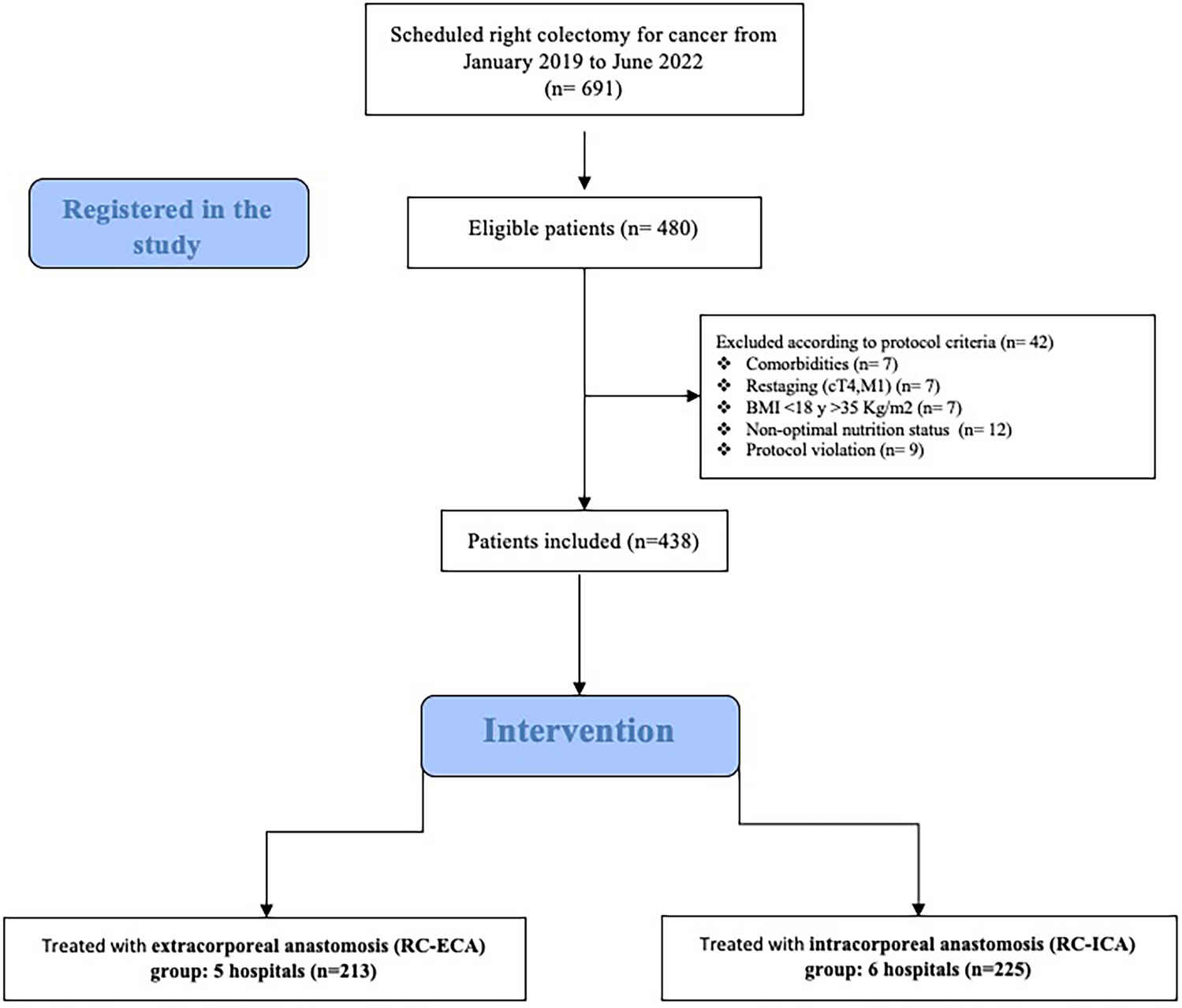
Our primary endpoint showed no superiority between techniques: anastomotic leak occurred in 3/225 (1.33%) after ICA and 3/213 (1.41%) after ECA (p = 1.00), yielding AL < 2% in both groups. For secondary outcomes, ICA was associated with lower conversion to open surgery (2.2 vs 7.5%, p = 0.013) and shorter hospital stay (median 4 days, p < 0.001), while no differences were observed in severe morbidity, SSI, reoperation, or mortality. In propensity score–matched analyses (213:213), no between-group differences reached statistical significance, with directionally similar estimates and wider uncertainty.
To reduce variability, RC-ECA was limited to side-to-side or end-to-side techniques (manual or mechanical), and only laparoscopic approaches were included, excluding robotic surgery. This improves the external comparability of results.
The absence of randomization required the introduction of all possible compensatory mechanisms [26]: the use of selection criteria that excluded factors associated with AL in previous studies [3, 4, 28]; the application of predictive risk models such as POSSUM [20] and CR-POSSUM [21]; the use of an online database managed by an independent firm, the randomized monitoring of 30% of the study data by an independent firm; the logistic regression analysis of the COSC; and the use of PSM statistical analysis.
The ICA technique offers advantages, but these are offset by the need for considerable skill in laparoscopic surgery and the longer learning curve. In our study, the median operative time in the ICA group was 175 min, compared to 110 min in the ECA group, with statistically significant differences, as previously reported [11, 29].
High-quality prospective controlled data directly comparing RC-ICA versus RC-ECA are scarce [29, 30]. Recent meta-analyses are inconclusive regarding superiority, with pooled estimates generally favoring intracorporeal anastomosis or being compatible with noninferiority [31, 32]. Consistent with our findings, the multicenter MIRCAST study reported AL rates < 2% with no significant differences between ICA and ECA [10]. Our study adds value by focusing exclusively on laparoscopic right colectomy for cancer using standardized techniques in high-volume centers, enhancing applicability to routine laparoscopic practice.
Although our hypothesis of ICA superiority for AL was not confirmed, both techniques achieved very low AL rates (< 2%) under standardized, purely laparoscopic conditions [7,8,9]. The unexpectedly low rate observed with ECA contrasts with prior multicenter reports (~ 8%) [4, 5] and likely reflects the study context: specialized coloproctology units, consistent use of each center’s standard approach by experienced teams, prospective monitoring, and predefined eligibility that excluded known high-risk features for leak [7,8,9]. Despite lower uptake of ERAS and prehabilitation in ECA centers, these factors did not show a conclusive impact on postoperative complications in our analyses. Residual between-hospital confounding remains possible, but sensitivity analyses (including propensity-score matching) were consistent with the main findings.
These findings are consistent with contemporary prospective series—including MIRCAST [10]—reporting low ECA leak rates in expert, high-volume units (≈1–6%) [4, 5]. In our cohort, strict eligibility (well-nourished patients without locally advanced disease) and the exclusive involvement of specialized colorectal surgeons using a uniform laparoscopic technique likely contributed to < 2% AL in both groups. While this reflects current optimized practice, it also lowers the number of events and thus reduces the statistical power to detect small between-group differences, as acknowledged among the study’s limitations.
Although ICA theoretically offers advantages by avoiding exteriorization of the bowel ends and minimizing mesenteric traction and colonic manipulation—factors that may improve perfusion and reduce tissue trauma—our data do not demonstrate a lower AL rate compared with ECA. In experienced colorectal units, standardized ECA can achieve similar outcomes, supporting that surgical expertise and adherence to technical principles are more determinant than the anastomotic approach itself. Nevertheless, ICA remains technically demanding, requires advanced laparoscopic proficiency, and may prolong operative time, which should be acknowledged when interpreting its wider applicability.
Overall complications were higher in the RC-ICA group (38.2% vs. 30.5%), though not statistically significant and mostly Clavien-Dindo ≤ II. Surgical complications were more frequent with RC-ICA; however, rectal bleeding rates were similar. Despite shorter incisions in RC-ICA, VAS pain scores on postoperative days 1–2 were comparable. Despite the absence of differences in Relevant Cl-D (Cl-D > II) postoperative complications, hospital stay was shorter in the RC-ICA group, in agreement with other studies [32, 33]. As in most published studies, surgical time was longer in the RC-ICA group, although this did not impact the rest of the variables used to assess postoperative complications.
Infectious complications did not differ between groups. As in MIRCAST [10], the COSC composite (Table 4) showed no between-group differences [34]. In multivariable logistic regression, only VAS > 2 on postoperative day 2 predicted COSC (OR 1.6, 95% CI 1.3–2.1) [35]. Conversion occurred in 4.8%, comparable to other series [7, 10], and was significantly lower with RC-ICA despite greater procedural complexity, in contrast to some series reporting different conversion patterns [32, 33, 36]. In an exploratory post hoc analysis restricted to ECA, conversion appeared higher with end-to-side than side-to-side anastomosis (16.9 vs 0.8%; p < 0.001), with no signal for manual versus mechanical construction. As the study was not designed to test configuration-specific effects and this association is sparsely described in the literature, it should be interpreted cautiously.
Although differences in conversion rate and length of stay were statistically significant, their absolute magnitude was modest and should be interpreted cautiously. Nonetheless, in expert, high-volume centers, even small improvements in these parameters may offer meaningful efficiency and recovery benefits.
This study has several limitations. The allocation of ICA versus ECA was determined at the hospital level rather than randomized at the patient level. Although this approach minimized intra-institutional selection bias, it may have introduced inter-institutional confounding factors that should be considered when interpreting the results. The strict selection criteria, which led to the inclusion of 69.5% of all potentially eligible patients. This increases internal validity but partially limits external validity. In addition, in the RC-ECA group more than one type of anastomosis was occasionally performed. The recruitment period also coincided with the COVID-19 pandemic, which prolonged the study excessively. Resident participation was more frequent in the ECA group; however, this variable was included in both the multivariable and propensity-score models. It was not identified as an independent predictor of anastomotic leak or severe morbidity and was adequately balanced between groups after matching.
Finally, the < 2% anastomotic-leak rate observed in both groups—well below the ~ 8% assumed a priori from contemporary multicenter studies [4, 5]—substantially reduced the power to assess non-superiority for the primary endpoint. Moreover, the very small number of events (n = 6; 3 per group) precluded meaningful adjusted modeling for AL and widened confidence intervals. Consistent with the prospectively registered protocol and good research practice, the pre-specified sample size was not modified post hoc; therefore, estimates for the primary endpoint should be interpreted with caution.
Future studies planned within this project will focus on the relative impact of both procedures on oncologic outcomes, long-term cost-effectiveness—including functional and occupational recovery—and the incidence of incisional hernia. Finally, another limitation is the absence of data on smoking and alcohol consumption as potential risk factors for anastomotic leakage, which were not included in the original study design.

Comments (0)